
Abstract
Percutaneous cholecystostomy (PC) tube insertion has been shown to be an effective treatment of acute cholecystitis (AC) as a temporary step to subsequent laparoscopic cholecystectomy (LC). However, the optimal time gap between PC implantation and LC has not been identified. Adult patients who underwent PC followed by LC for the treatment of AC between 2016 and 2020 were retrospectively reviewed and analyzed. One hundred twelve patients, consisting of 59.8% males, were included and received LC after a median of 65 [48 - 96.5] days following the PC placement. No deaths or reoperations occurred within 30 days, but 16 (14.3%) patients were readmitted, and 16 (14.3%) required subsequent reintervention. Although a longer interval between PC and LC had no effect on perioperative outcomes, it was associated with considerably longer intensive care unit (ICU) stay. According to these findings, patients may benefit from early LC following PC for the treatment of AC.
With a lifetime prevalence of 10 to 15%, acute cholecystitis (AC) is one of the most prevalent surgical diseases in the United States. 1 Laparoscopic cholecystectomy (LC) is the gold standard therapy for AC in low-risk individuals. Nonetheless, perioperative mortality is increased in older patients with severe comorbidities or critical illness. Percutaneous cholecystostomy (PC) tube placement has been shown to be an effective treatment of AC in high-risk patients as a bridge therapy to subsequent cholecystectomy. Specifically, LC reduces PC complications and is the recommended therapy for individuals who are regarded eligible surgical candidates after their recovery from the AC. 2
Previous studies have analyzed the results of individuals having LC after PC implantation; however, the optimal time gap between the procedures has not been identified. A recent study evaluating the timing of LC after PC placement found that LC within 8 weeks is associated with a higher risk of overall surgical complications and a longer length of stay, with no significant differences in 30-day readmissions, emergency department (ED) visits, or common bile duct injury. 3 The purpose of this study was to present the experience of a tertiary academic center regarding PC placement followed by LC in critically ill patients and investigate how the time interval between the 2 procedures affects patient outcomes.
Data from adult patients who underwent PC followed by LC for the treatment of AC between 2016 and 2020 were retrospectively reviewed. Only patients with definite or suspected AC, based on the Tokyo guidelines, were included. 4 Patients with a history of hepatobiliary surgery, common bile duct stones, cirrhosis, active malignancy, or chronic immunosuppressive therapy were excluded from the study. Additionally, cases with PC insertion and LC procedure during the same hospitalization, failure of PC to control the inflammation, or aborted LC were excluded. After obtaining institutional review board approval, patient baseline characteristics, PC and LC hospitalization data, and perioperative outcomes following LC were collected.
Binary variables were presented as absolute or relative frequencies, whereas continuous variables were presented as mean +- standard deviation or median [Q1-Q3]. Logistic and linear regression models were used to study the effect of the interval between PC and LC on intra- and postoperative outcomes. For all tests, P < .05 was considered significant. All analyses were performed using STATA 16.0 software (STATA Corporation, College Station, TX, USA).
One hundred twelve patients, consisting of 59.8% males and with a mean age of 64.6 ± 14.8 (mean ± SD) years, were diagnosed with AC at our academic center and met the study’s inclusion criteria. Using the TG18/TG13 guidelines, 4 54.5% of patients had mild (grade I), 36.6% moderate (grade II), and 8.9% severe AC (grade III). Based on patient’s previous history, the mean Charlson Comorbidity Index (CCI) was 4.7 ± 2.8, while the emergency surgery score was 7 ± 3.1 at the time of index admission. The most common indication for drainage was mild AC with severe comorbidities (22.3%), followed by moderate AC with severe comorbidities (12.5%), severe AC with severe comorbidities (10.7%), severe AC with negative prognostic factors (8.9%), and other (45.5%). Most patients had a history of previous abdominal surgery (52.7%).
All patients underwent PC placement on average 1.9 ± 2 days after the AC diagnosis and received antibiotic treatment for 9.2 ± 7.5 days. The length of hospital stay during index hospitalization was 11 ± 8.9 days, whereas 17% of the patients required to be transferred to the intensive care unit (ICU) for 9.6 ± 10 days. No mortality was reported during the hospitalization for PC insertion, with 75% of patients being discharged to their homes and the rest in rehabilitation centers, skilled nurse facilities, etc.
Additional imaging was performed in 88 (78.6%) patients before the LC, with 70 (62.5%) repeating a CT scan, 42 (37.5%) a cholangiography, and 7 (6.3%) an MRI/MRCP. The median duration between the PC implantation and the LC was 65 [48 - 96.5] days, with most cases being elective (97.3%). In 96.4% of patients, the cholecystostomy tube was removed at the time of the LC, while 9 cases (8%) were converted from laparoscopic to an open approach. Intraoperatively, 14 (12.5%) cholangiographies were performed, and none of the patients required an endoscopy. Overall, 15 intraoperative events (Class I) occurred, corresponding to 13.4% of patients. In 14 cases, accidental gallbladder puncture occurred, while the the colon serosa was damaged superficially in one case.
The biliary leak rate within 30 days following the procedure was 3.6%, with all 4 incidents classified as type A (bile leak from the cystic duct or liver bed without further injury). Additionally, one of them had undergone fenestrated cholecystectomy, which increased the rate of biliary leak significantly. All cases were treated successfully with ERCP shpincterectomy and stent placement. None of the patients were reoperated, 18 (16.1%) visited the ED within 30 days from LC and were readmitted for complications related to the procedure. Finally, 16 (14.3%) patients required further reintervention. Specifically, CT-guided drainage collection in the gallbladder fossa was conducted in 13 (11.6%) cases, and biliary interventions (ERCP) in 4 (3.6%). Three of the patients requiring fluid drainage and one needing ERCP had undergone fenestrated cholecystectomy.
Univariate linear regression of the intra- and peri-operative outcomes during the LC hospitalization.
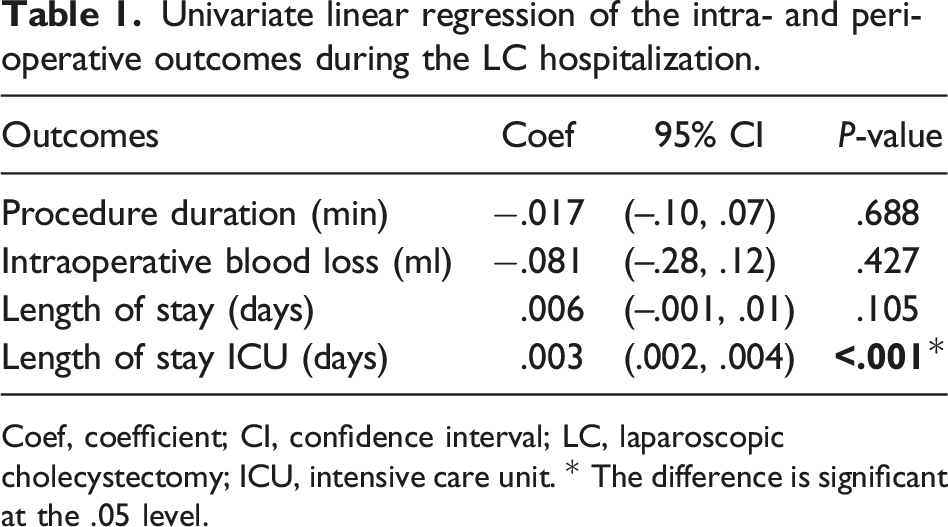
Coef, coefficient; CI, confidence interval; LC, laparoscopic cholecystectomy; ICU, intensive care unit. * The difference is significant at the .05 level.
To conclude, PC placement followed by LC in critically ill patients diagnosed with AC is safe, effective, and with favorable complication rates. Although a longer interval between PC and LC had no effect on perioperative outcomes, it was associated with a considerably longer ICU stay. Patients may benefit from early LC following PC for the treatment of AC. However, multi-institutional studies are required to corroborate these findings.
Footnotes
Authors’ Contributions
The authors confirm contribution to the paper as follows:
Study conception and design: Stefanidis D. and Giannopoulos S;
data collection: Makhecha K., Madduri S., Garcia F., Baumgartner C.T., and Giannopoulos S;
analysis and interpretation of results: Giannopoulos S. and Stefanidis D;
draft preparation: Giannopoulos S. and Stefanidis D;
critical content revision: Stefanidis D., Giannopoulos S., Makhecha K., Madduri S., Garcia F., and Baumgartner C.T.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
Dr. Dimitrios Stefanidis has received institutional research support from Becton Dickinson and Intuitive and is consultant with applied medical which are not related to this study.