
Abstract
Background
Acute appendicitis is possible for any pediatric patient with abdominal pain. At our tertiary care center, patients are transferred for surgical management with unnecessary or excessive imaging. We hypothesize that using the Alvarado score (AS) to clinically stage patients will identify patient groups that could be transferred prior to imaging.
Methods
Retrospective review of pediatric patients transferred to our hospital for suspected appendicitis between 11/2020 and 3/2022 was performed. Variables collected included AS, imaging, and pathology. Alvarado score was calculated for each patient, and patients were grouped into low score, intermediate score, and high score groups. Positive predictive values (PPVs) were calculated for patients who underwent CT.
Results
196 patients (age 2-17, 58% male) were transferred with suspected appendicitis. CT was obtained in 67% of patients and was not significantly different between groups. The low-score group (n=35) had a rate of appendicitis of 14% and the PPV of CT was 33%. The intermediate-score group (n = 74) had a rate of appendicitis of 62% and the PPV of CT was 88%. In the high-score group (n = 87), the rate of appendicitis was 92% and PPV of CT was 98%.
Discussion
Our data show that patients with low, intermediate, and high AS undergo CT at similar rates. We suggest that patients in the low score and high score groups may not benefit from reflexive CT given the likelihood of appendicitis based on the Alvarado score. We propose that CT in these groups be performed at the discretion of the pediatric center in order to expedite transfer and spare children excess radiation.
Key Takeaways
• CT scans are not equally useful for all pediatric patients when evaluating for appendicitis. • Low Alvarado score patients have a low likelihood of appendicitis and CT has low PPV, so should be ordered selectively. • High Alvarado score patients have a PPV of >90%, making CT an unnecessary confirmatory test which should be ordered at the discretion of the tertiary center. • Stratifying patients by Alvarado scores can reduce the radiation exposure by CT and allow for early transfer to pediatric centers.
Introduction
Appendicitis is one of the most common causes of acute abdominal pain in pediatric patients. 1 Despite its prevalence, diagnosis guidelines have not yet been established, and there are varying clinical pathways using a combination of clinical judgment, laboratory findings, and radiologic imaging. 2 The workup of patients with suspected appendicitis must balance appropriate levels of vigilance to avoid missed diagnosis, with judicious use of harmful ionizing radiation and unnecessary hospitalization.
Imaging modalities used to diagnose appendicitis include ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI). Since its inception in the 1970s, CT use has increased exponentially, with the greatest increase over the past decade being in pediatric cases. 3 Though CT increases diagnostic accuracy, it exposes patients to ionizing radiation which may be particularly harmful to pediatric patients as cells are rapidly dividing.4,5 Several studies have observed a relationship between low-dose radiation exposure from CT scans and long-term health implications, including leukemia, brain tumors, and other cancers. 6
There is a large variation in the rate of CT utilization among hospitals depending on their imaging algorithm for suspected appendicitis. 7 A study comparing the rate of CT for transfers vs non-transfers in the evaluation of pediatric appendicitis was 73.5% vs 26.4%, respectively. 8 This demonstrates an area of possible improvement in the management of pediatric patients with abdominal pain.
Clinical scoring systems, such as the Alvarado score, can predict the likelihood of appendicitis based on the patients’ history, physical exam, and laboratory findings.1,9,10 One retrospective cohort study demonstrated that Alvarado score <3 for negative appendicitis had a sensitivity of 96.2% and specificity of 67%, while Alvarado scores >7 had a sensitivity of 77% and specificity of 100%. 9
Stratifying patients based on Alvarado score group may help predict certain groups that do not benefit from a reflexive CT at transferring facilities. We reviewed our pediatric patients transferred for suspected appendicitis to evaluate the utility of CT when patients are stratified by Alvarado score. We hypothesize that using the Alvarado score to clinically stratify patients will identify patient groups that could be transferred without undergoing imaging.
Materials and Methods
A retrospective chart review of pediatric patients (age<18) that were transferred to our tertiary care academic institution for abdominal pain were identified from transfer center logs between November 2020 - March 2022, after approval from the institutional review board at Cooper University Hospital. All patients with acute appendicitis in the differential diagnosis were included. There were no exclusion criteria.
Electronic chart review was used to identify patient demographics including age, sex, and race/ethnicity. Additional clinical variables were collected including laboratory Tests, vital signs, all imaging modalities, and length of stay. Components of the Alvarado score including presence of anorexia, nausea, or vomiting; migration of abdominal pain to the right lower quadrant (RLQ); RLQ tenderness; and rebound tenderness were ascertained from notes from both the transferring hospital and our institution. The operative and pathology reports were collected as well.
The diagnosis of acute appendicitis was verified by clinical course with either surgical intervention with positive pathologic evidence of appendicitis or nonsurgical medical management with hospital stay for antibiotic therapy. No patients were treated with oral antibiotics for outpatient medical management for appendicitis at our institution.
Alvarado Score.
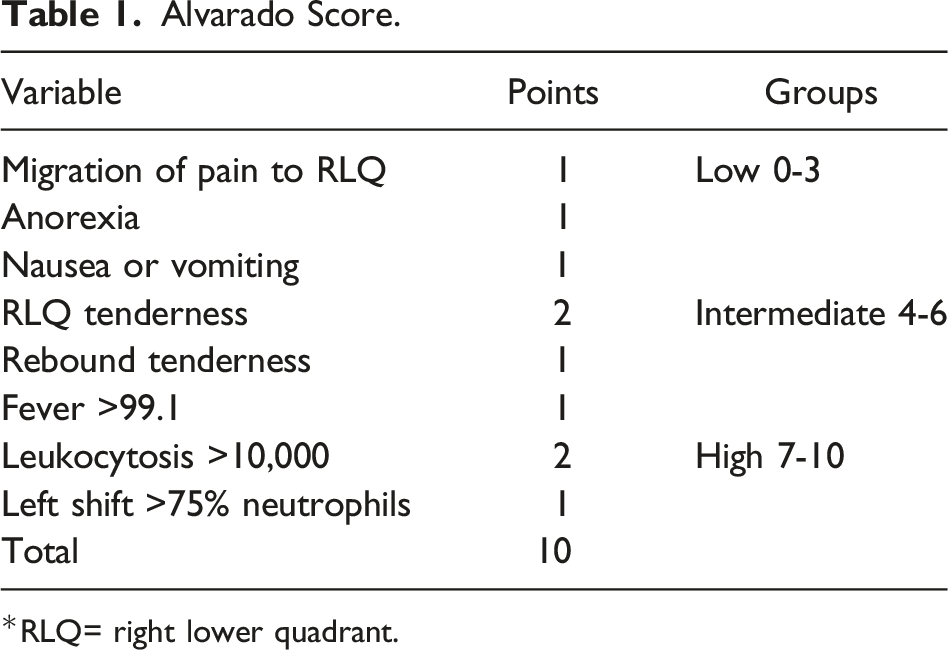
*RLQ= right lower quadrant.
Results
Over the 17 month period of data collection, 196 pediatric patients were transferred to our tertiary care center with a concern for appendicitis. The average age was 11 years, with a range of age 2-17, and 114 patients were male (58%). Race/ethnicity was recorded, in which 53 patients (27%) were white, 28 patients (14%) were African American, 85 patients (43%) were Hispanic, 7 patients (4%) were Asian, 5 patients (3%) were multiracial, and 18 patients (9%) were considered other/unknown. There were no statistically significant differences between the low score, intermediate score, and high score groups.
The low-score group (0-3) included 35 patients (18%), the intermediate-score group (4-6) included 74 patients (38%), and the high-score group (7-10) included 87 patients (44%) (Figure 1). In total, 131 patients (67%) had a CT scan. The rate of CT scans across Alvarado score groups was similar, with 25 patients in the low-score group (71%), 52 patients in the intermediate-score group (70%), and 54 patients in the high-score group (62%). Appendicitis by Alvarado score.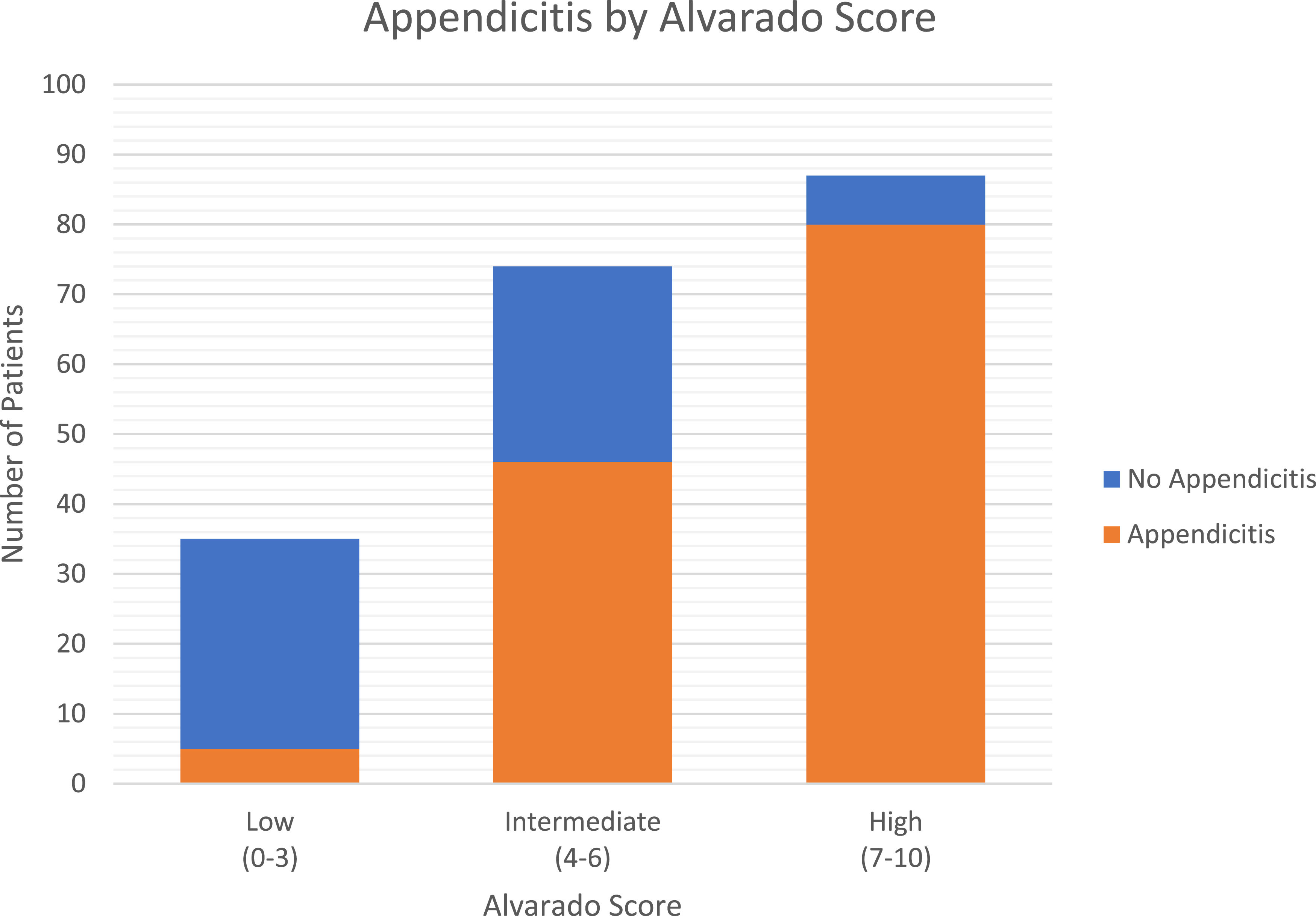
Overall, appendicitis was diagnosed in 131 (67%) of patients. In the low-score group, the rate of appendicitis was 14%. The NPV of the Alvarado score for appendicitis was 86%, and the PPV of CT was 33%. Negative predictive value was used for the Alvarado score in the low-score group as it is a “rule out” group, clinically suspecting no appendicitis, and CT reads are clinically useful based on the positives being correct, as seen with a PPV.
In the intermediate-score group, the rate of appendicitis was 62%, and the PPV of CT was 88%. Alvarado score in this group is not predictive of appendicitis so no NPV or PPV was calculated.
In the high-score group, the rate of appendicitis was 92%, and the PPV of the Alvarado score was 92%. In this group, 62% of patients underwent CT scan, and the PPV of CT was 98% (Figure 2). CTs by Alvarado score.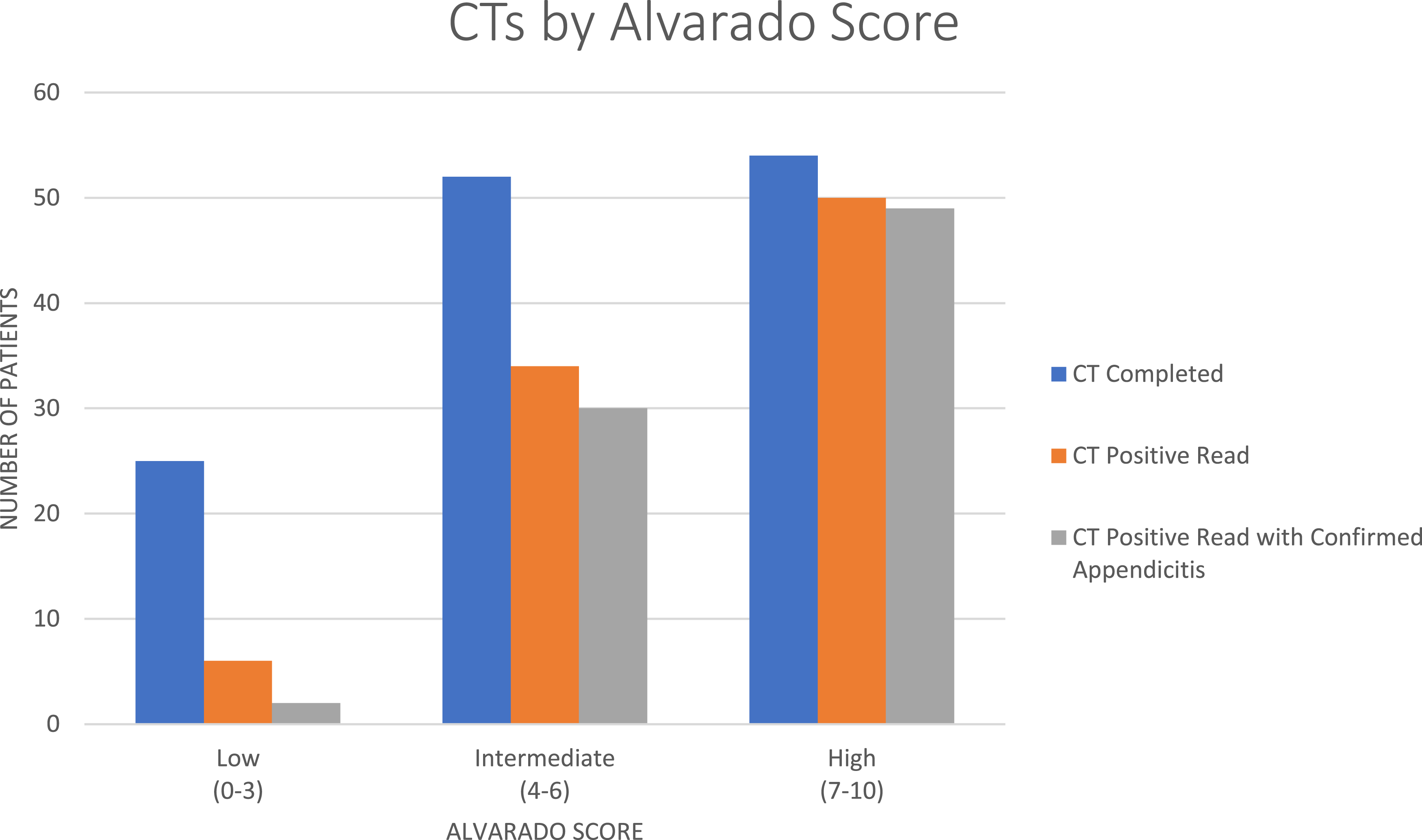
The average length of stay was 1.4 days for all patients. 128 patients (66%) went to the operating room for appendectomy or had a drain placed by interventional radiology. Two patients from the intermediate-score group were discharged after a PO trial and re-admitted for appendectomy, neither had a CT performed but had MRIs completed on re-admission. One patient from the low-score group underwent a negative appendectomy, no CT was performed, and ultrasound was performed at the outside hospital and read as acute appendicitis.
Discussion
We sought to assess the rate of CT utilization for the diagnosis of appendicitis in patients transferred to our pediatric hospital. Furthermore, we used the Alvarado score to stratify patients into groups to identify populations which benefited from CT. In our study, we found that CT prior to transfer was being performed at similar rates, 62-71%, regardless of Alvarado score. We found that Alvarado scores were predictive of appendicitis, and the CT diagnosis from the transferring facility had less utility in the low and high Alvarado score groups.
In our population, patients with low Alvarado scores did not benefit from CT. The rate of appendicitis is so low that CT had a PPV of 33% for the subset of patients. For the same group, the Alvarado score had an NPV of 86%. More information about the patients in order to identify or rule out appendicitis can be obtained with observation or ultrasound imaging. 11
A limiting factor for examining the low-score group is that our study population comprises only the patients that were transferred. There are unaccounted for patients who were able to be discharged from the transferring center following a negative CT or admitted without the concern for appendicitis. While the value of a negative CT is not overlooked, patients who do not meet discharge criteria may be safely observed without CT.
Patients in the high-score group had a PPV of 92%, making the argument that these patients can be reliably diagnosed without CT. CT is more accurate with a PPV of 98% but is likely not necessary to determine treatment. We would argue that taking a patient to the operating room without confirming imaging is at the discretion of the surgeon. Also, the imaging modality could be more pediatric friendly with a fast MRI or abdominal US, both of which eliminate radiation. Lastly, these patients would not experience a delay in transfer waiting for imaging. The decision to order further imaging should be based on evaluation at the treating center.
Widespread use of CT for the diagnoses of appendicitis in the pediatric population is being challenged given the clear drawbacks. CT imaging may not add clinically useful information for patients with high or low pretest probability of appendicitis, as radiologists at non-pediatric hospitals have difficulty interpreting these studies, and radiation associated with cross-sectional imaging has a higher risk in the pediatric age group than adults.12-14 CT use in the diagnosis of appendicitis has also been shown to significantly increase time to surgery, which increases the risk of perforation, leading to postoperative complications and poor outcomes.15,16
The patients with intermediate Alvarado scores are less clear. Only 62% of the population that was transferred for appendicitis had appendicitis, but CT improved the PPV to 88%. These patients benefit the most from imaging. In situations where CT could triage patients that needed transfer vs those who could be admitted at their primary institution, performing a CT would save time and cost. In situations where the patient would require transfer regardless of the CT, there is a benefit from early transfer and early evaluation by pediatric surgery.
CT has a low but established carcinogenic risk. Even with modern CT scanners and “as low as reasonably achievable” principles, radiation doses cannot be reduced to zero, and prior studies have strongly indicated an increase in leukemia, brain cancer, or fatal cancer in general following CT imaging in pediatrics. These risks appear to exist even in “low” radiation doses under 50 mSV.17,18 Considering that 60% of our patients with CT imaging prior to transfer fall into the high- or low-risk category, more than half of the CT scans obtained to evaluate for appendicitis in the local community need not have been obtained.
Additionally, accuracy in reading pediatric imaging is worse at adult hospitals compared to pediatric centers, so CTs obtained at the referring institutions may not be correctly guiding management, despite the harms of the radiation that was supposedly traded for increased diagnostic accuracy.
13
While unnecessary transfers should indeed be minimized, increased use of CT imaging does not appear to be a successful method of doing so, and instead we propose following clinical scoring systems like Alvarado in triaging patients for transfer (Figure 3). Flow diagram of appendicitis workup (created with BioRender.com).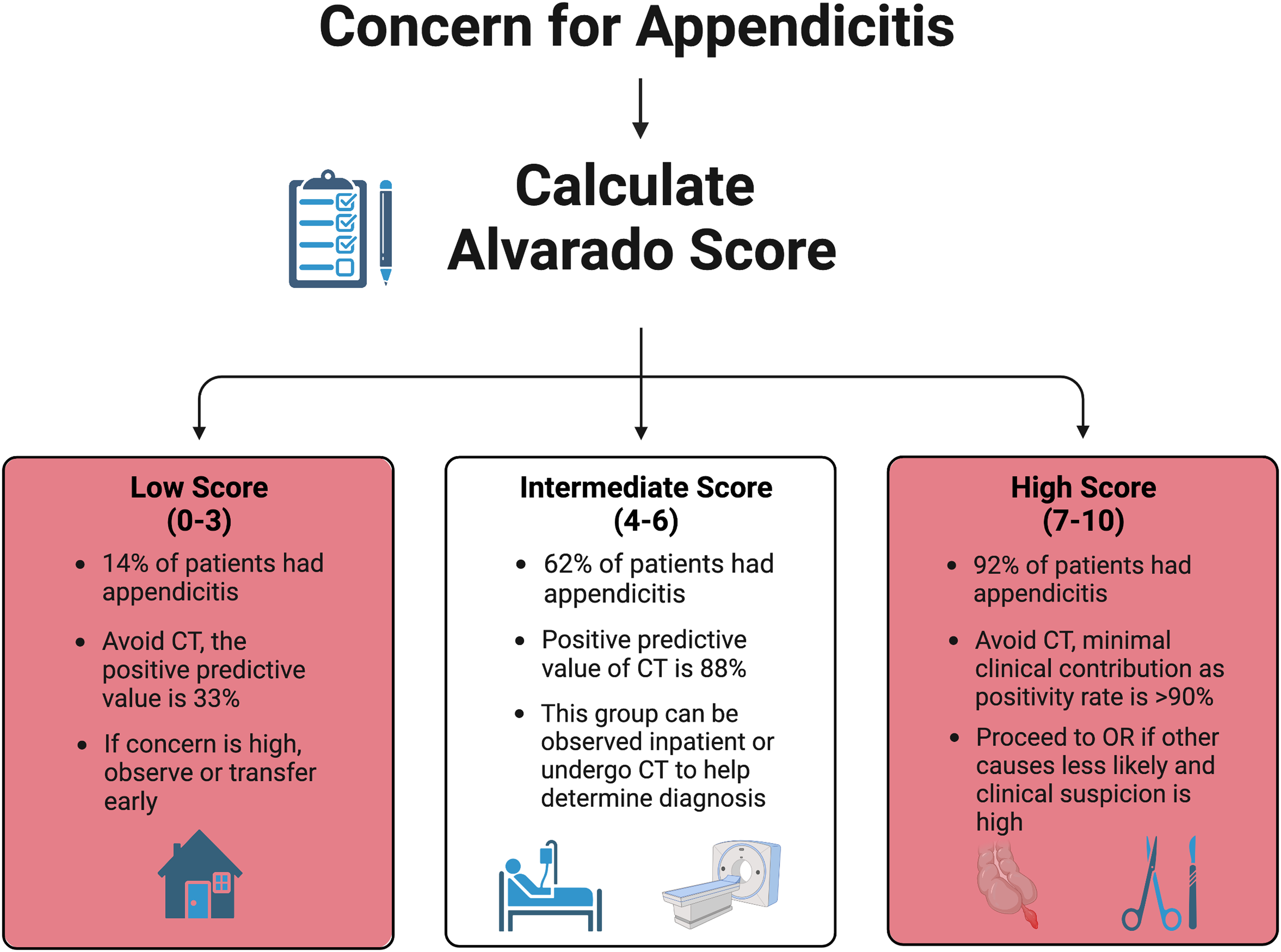
Our study does have some limitations. Alvarado scores were retrospectively calculated from chart review, and absence of data was assumed to be absence of symptom; thus, Alvarado scores in all categories may have been higher with more complete information. This could potentially push some low-risk patients into intermediate risk and justify their CT imaging, or conversely push intermediate-risk patients into high risk and remove their indication.
We were also inherently limited by our study population, evaluating patients that were transferred. It may be that community hospitals are only scanning a minority of patients they see, or are discharging many patients after imaging that is read as negative at their facility, both of which would alter our assessment of community hospital imaging and transfer practices. A future direction of our group’s research will include patients whose initial presentation is at our institution as a tertiary care pediatric center to determine if there are differences in rate of CT and patient outcomes based on Alvarado group.
Nevertheless, even within our dataset of patients who were transferred, there is room for improvement in reducing radiation to these patients. Providers at pediatric centers should strive to work with transferring institutions to standardize workup protocols that minimize radiation and prioritize use of clinical risk scores and imaging without ionizing radiation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.