
Abstract
Background
In rural state trauma systems, management of the obstetrical trauma patient often defaults to transfer to level I trauma centers. We evaluate the necessity of transferring obstetrical trauma patients without severe maternal injury.
Materials and Methods
A retrospective 5-year review of obstetrical trauma patients admitted to a rural state-level I trauma center was conducted. Injury severity measures such as abdominal AIS, ISS, and GCS were correlated with outcomes. Furthermore, the impact of maternal and gestational age on uterine compromise, uterine irritability, and the need for cesarean section intervention are presented.
Results
Twenty-one percent of patients were transferred from outside facilities with a median age of 29 years, average ISS of 3.9 ± 5.6, GCS of 13.8 ± 3.6, and abdominal AIS of 1.6 ± .8. Outcomes included maternal fatality of 2%, fetal demise of 4%, 6% experienced premature rupture of membranes, 9% experienced fetal placental compromise, 15% had uterine contractions, 15% of cesarean deliveries, and fetal decelerations occurred in 4%. Predictors of fetal compromise are strongly associated with high maternal ISS and low GCS.
Discussion
The frequency of traumatic injury in this unique population of patients is fortunately limited. The best predictor for fetal demise and uterine irritability is maternal injury severity, measured by ISS and GCS. Therefore, without severe maternal trauma, obstetrical trauma patients with minor injuries can safely be managed at non-tertiary care facilities with obstetrical capabilities.
Introduction
Trauma is the leading cause of non-obstetric death in pregnant women, impacting up to 7% of pregnancies. 1 Of these traumas, motor vehicle collisions (MVCs) account for about 55%, falls for 22%, and assault and burns for 1%. 2 Although MVCs are the most common cause of trauma in pregnant people, adverse fetal outcomes and fetal death are more likely to occur in the presence of increased crash severity, improper seat belt use, and severe maternal injury. 3 Traumas resulting in orthopedic injuries have higher associations with preterm birth, placental abruption, fetal instability at birth, infant death, and even maternal death. 4 Adverse fetal outcomes and demise after trauma have been shown to depend on several different factors, regardless of the category of the trauma.
Although the vast majority of traumas during pregnancy (90%) are considered minor, an alarming 60-70% of those minor traumas result in fetal death. 5 In contrast, traumas categorized as “major” have been associated with 9% maternal mortality and 80% fetal mortality if the woman presents in shock. 6 After a penetrating abdominal injury, those statistics change to 66% and 73% chance of mortality for the fetus and mother, respectively. 7 Al Mulhim et al. defined the three most important predictors of poor fetal outcomes or demise as traumas occurring in the second trimester of pregnancy, placental abruption, and a high maternal injury severity score (ISS). 8 Theodorou et al. further defined a high ISS as a score of >9 and found it to be a predictor of poor fetal outcome. 9 This study also found that pregnancy of fewer than 23 weeks in conjunction with ISS of >9 increased fetal mortality by 5-fold. 9 Hoff et al findings supported Theodorou et al but also observed increasing face and abdominal AIS, fluid requirements, maternal acidosis, and maternal hypoxia to be significantly associated with fetal demise. 10 In the face of these negative predictors, Mendez-Figueroa et al. reference that the highest impact upon fetal death is the necessity to perform emergency cesarean extraction immediately following traumatic injury. 11
After a pregnant woman experiences trauma, the most accurate representation of fetal status is electronic fetal monitoring. 12 Although there is no official guideline for the recommended length of fetal monitoring, one study found that after minor trauma, the fetus should be monitored for 4-24 hours using tocodynamometry. 5 Certain risk factors help guide the type and length of fetal monitoring following trauma. Symptoms such as contractions, signs of preterm labor, or vaginal bleeding indicate risk to the fetus and would warrant more extensive monitoring for a longer period of time, but patients without any of those symptoms can be monitored for 6 hours and then safely discharged home. 13 In addition to electronic fetal monitoring, ultrasonography should be performed. 5 This is important because although it has low sensitivity, it has high specificity for placental abruption, which is a significant risk factor for poor fetal outcomes. 5 To determine the degree of fetomaternal hemorrhage, a Kleihauer-Betke test should be performed after trauma, and this test is important regardless of Rh status. 5
In a rural state with one level 1 trauma center, the transfer of all obstetrical patients following trauma is burdensome, taxing the availability and allocations of resources. Furthermore, the displacement of patients from their community and support systems can be challenging to the patient’s emotional well-being and financial burdens associated with such transfers at times exceeding 8 hours. This investigation will collaborate and explore to identify maternal/fetal indicators that warrant transfer to level 1 trauma center vs those that will allow the patient’s care to be a continuum of available resources in their community hospital system.
Materials and Methods
A retrospective 5-year review of obstetrical trauma patients admitted to a rural state-level I trauma center was conducted. Using the trauma registry, patients were selected for inclusion, meeting the criteria of suffering a traumatic injury during pregnancy. Patient demographic, injury characteristics, and outcome measures of both maternal and fetal outcomes were collected. Injury severity measures such as Injury Severity Score (ISS), Abbreviated Injury Scale (AIS), and Glasgow Coma Scale (GCS) were correlated with outcomes. The frequency of fetal monitoring and ultrasound use and their findings were assessed. Furthermore, the impact of maternal and gestational age on uterine compromise, uterine irritability, and the need for cesarean intervention are also presented. Data were analyzed in Rstudio 14 using descriptive statistics and regression analysis. This study was approved by the MaineHealth Institutional Review Board, and the approval number is 1740395.
Results
Injury Characteristics.
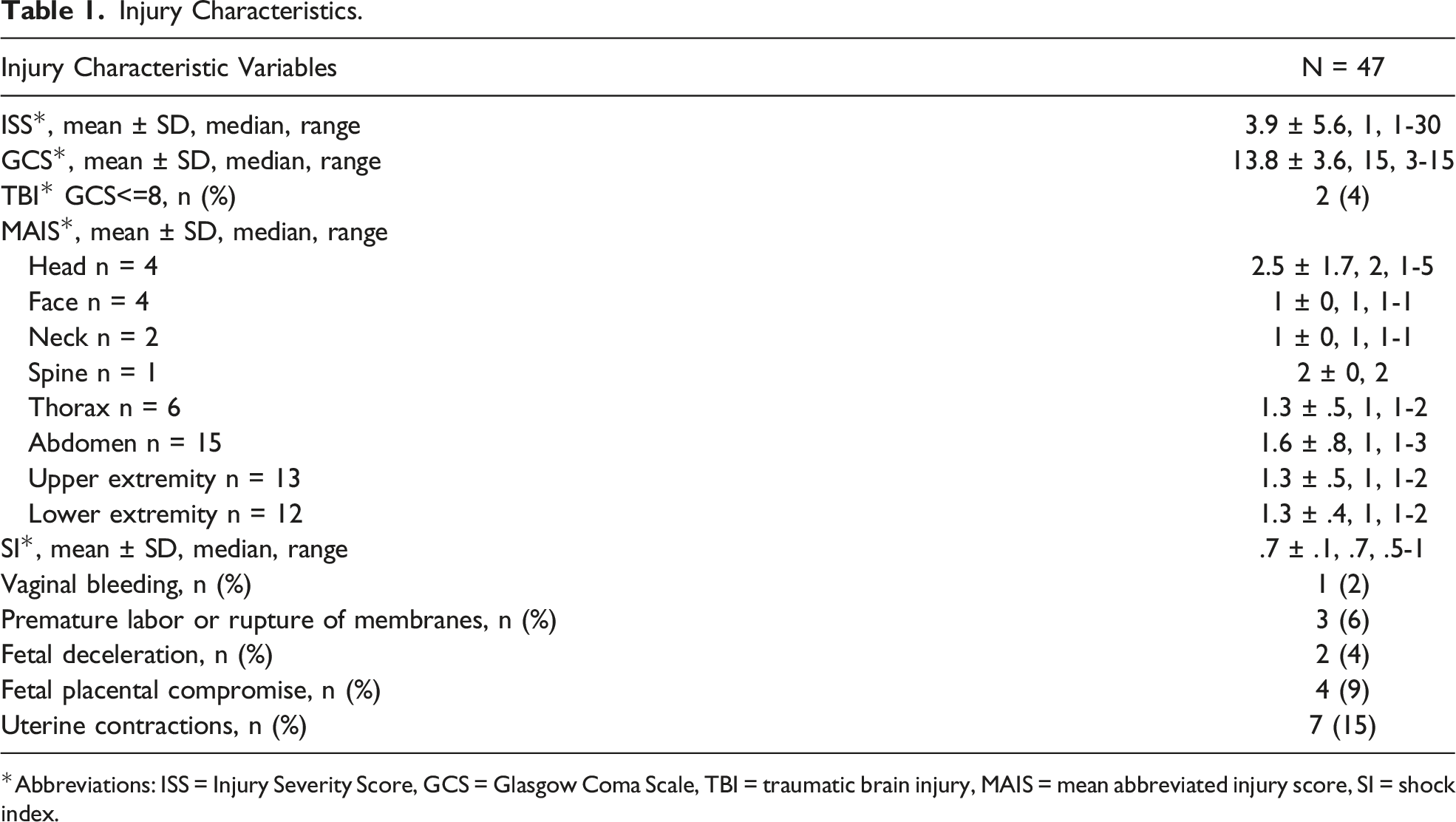
*Abbreviations: ISS = Injury Severity Score, GCS = Glasgow Coma Scale, TBI = traumatic brain injury, MAIS = mean abbreviated injury score, SI = shock index.
Hospital Outcomes.
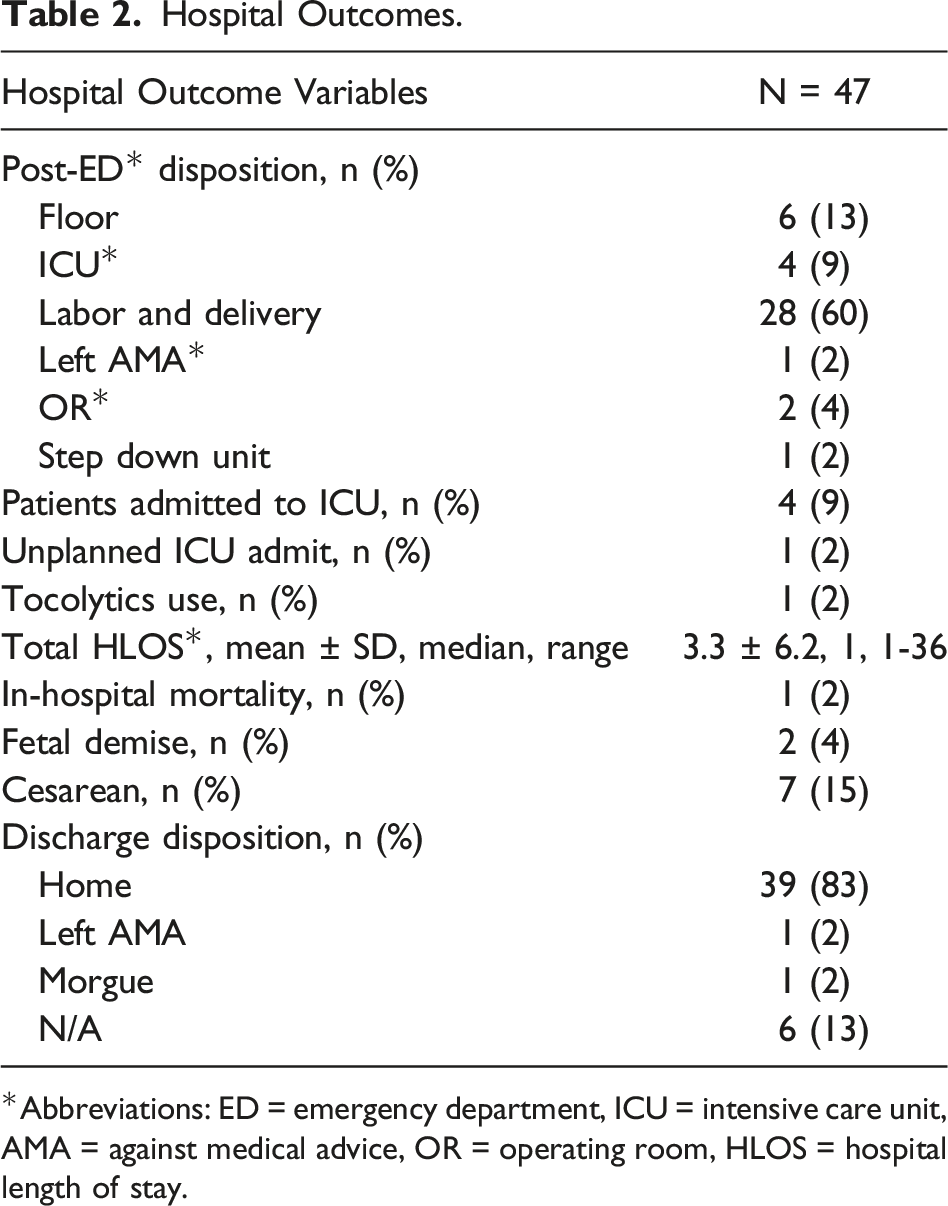
*Abbreviations: ED = emergency department, ICU = intensive care unit, AMA = against medical advice, OR = operating room, HLOS = hospital length of stay.
The statistical analysis supports that high ISS (P = 8.64e-09) and low GCS (P = .001) increase the risk of maternal mortality and blood product utilization. Low maternal GCS is a positive predictor of fetal demise (P = .051), placental compromise (P = .001), and premature rupture of membranes (P = .001). No statistical correlation was found between abdominal AIS and fetal demise (P = .666). However, abdominal high AIS was statistically associated with premature labor (P = .005). A high maternal ISS (P = .011) and increased gestational age (P = .017) following injury demonstrate a higher rate for same hospital admission cesarean delivery. The greater the gestational (P = .002) and maternal age (P = .040), the greater the risk following trauma for uterine contractions.
Discussion
As a level 1 trauma center with over 3000 traumas per year averaging approximately 10 (.3%) obstetrical trauma victims severe enough to be captured in a trauma registry annually, suggests that this patient population suffering injury in this rural state is rare. This low obstetrical trauma frequency represents that the study was completed in the state with the oldest population, Maine, with the average frequency reported in other studies to approximate 5.3%. 15 This study population had a mean age of 28.6 years compared to other studies approximating 25 years of age.7,13 All patients in this study suffered blunt trauma from motor vehicle crashes. The ISS average for our population was 3.9 ± 5.6, far below the threshold of greater than or equal to 16 for predicted high risk of mortality, 16 with an SI of .7 ± .1. Rogers et al report a higher threshold of 50% mortality with an ISS more significant than 25, 17 which supports that our study population would be categorized as victims suffering minor trauma given we only had 1 patient with an ISS >25. There were a total of 2 fetal fatalities with maternal ISS of 5 and 15, below the threshold, with a GCS of 15 and 3, respectively, still demonstrating a statistical difference in comparison to fetal survivors of traumatic injury for both ISS and GCS. Kissinger et al in a multi-institutional study demonstrated that low GSC was associated with poor fetal outcomes; however, Aboutanos et al did not find GCS to be a predictor of fetal outcomes comparing women with injury to those with uncomplicated pregnancy. 18 Cusick and others would support that low GCS, in conjunction with other variables, contributes to poor fetal outcomes in obstetrical trauma.2,13 This investigation would agree with Cusick identifying low GCS as a statistically significant (P = .05) positive predictor of fetal demise, placental compromise, and premature rupture of membranes. Worthy of mention is that each of the fetal fatalities had at least one elevated marker of high risk, ISS or GCS.
Curet et al and others have identified an ISS greater than or equal to nine as a risk factor for fetal demise. 13 Kady et al collaborate these findings, noting that high ISS may result in worse outcomes, but low ISS equally has been associated with adversity to the fetus outcomes. 19 These investigators further note that adverse outcomes to the fetus in minor maternal traumatic injuries can be seen up to 5 to 25% of the time. 13 In a micro-analysis of our two fatalities, no vaginal bleeding occurred, no rupture of membranes was noted, no placental compromise was seen on ultrasound, and all occurred in the absence of uterine contractions known to threaten fetus viability. It is important to note that placenta abruption can occur in even minor traumatic injuries. 2 Deceleration in fetal tocodynamometry monitoring was only present in one of the fetuses in our study that had a fatal outcome. Even though minor trauma does not usually produce a maternal injury that compromises fetal viability, mortality in minor trauma can be as high as 60% to 70%. 5 Because of this, fetal monitoring is recommended even in women suffering minor traumatic injuries. 5 The literature would support worse outcomes in obstetrical trauma with advanced gestational age; in this study, the gestational ages were 36 and 29.5 months at the time of fetal demise. The risk of uterine injury once entering the second trimester would be expected given that it leaves the protection of the pelvic rim, exposing the uterus and fetus to direct blunt injury during deceleration. 13 With a mean gestational age of 27.5 ± 6.4, this study population is at the cusp between second and third trimesters, giving them maximal vulnerability by fetal age for injury. This correlates to this study’s statistically significant finding of premature labor with high abdominal AIS, P = .005. This study further demonstrated that with greater gestational (P = .002) and maternal age (P = .04), the risk of uterine contractions was statistically significant for this population.
Fetal ultrasound is one of the standards of care in evaluating the pregnant trauma patient. This allows for the detection of fetal movement and potential uterine rupture. In this study, 94% of the 47 patients had fetal ultrasounds, with 4 (9%) demonstrating fetal placental compromise. With placental abruption, a frequency of 65 to 75% fetal demise has been reported; therefore, immediate cesarean delivery is warranted. 1 Fetal ultrasound has been found to be inaccurate, only recognizing 24% of placental abruptions. 5 On the other hand, fetal monitoring for a minimum of 4 hours with 8 or more contractions is 100% accurate in predicting placental abruption and fetal compromise in utero.20,21 Fetal monitoring should be performed for a minimum of 6 hours in minor trauma, but if admitted for significant injury, a period of 24 hours or greater should be utilized. 13 Consistent with this concern, 96% of the patients in the study had fetal monitoring, with decelerations occurring in 2 patients and contractions recorded in 7. A total of 7 patients (15%) had emergent cesarean deliveries during the study for maternal-fetal compromise.
Following traumatic injury, obstetrical trauma patients most likely will travel through a continuum of care for injuries sustained. Frequent contact with the health care community should be inclusive with close monitoring of the obstetrical progression of their pregnancy. Sperry et al. report that even in the face of minor trauma, there appears to be an increase in low birth weight infants and preterm deliveries. 22 Management of the obstetrical trauma patient should follow the adage that the best care for the fetus is aggressive, attentive care of the mother. The resuscitation of the mother optimizing the physiology of oxygen delivery via a balanced resuscitation and expedited surgical control and management of injury will ensure the best outcome for both mother and child. In addition, the literature and our study support the early application of fetal monitoring to assess for at-risk tocodynamometry patterns necessitating early cesarean recovery of the fetus, which may have positive attributes to the resuscitation of the mother. The use of ultrasound should not be underutilized but not solely relied upon as a determinant of uterine compromise.
The decision to transfer a patient to a level 1 trauma center should be based on physiological parameters outlined by the American College of Surgeons Committee on Trauma. This study’s findings support that minor obstetrical trauma in the absence of physiological criteria may be appropriate to be assessed and managed at non-level 1 centers with appropriate resources to care for the patient. These resources should include the ability to perform fetal monitoring, maternal assessments of obstetrical risk to include ultrasound and biochemical assessments for maternal-fetal violation of circulation, Kleihauer-Betke testing, and emergency surgical deliveries of fetuses. A robust transfer agreement to a higher level of care must be in place if positive risk findings are discovered while monitoring the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.