
Abstract
Sclerosing encapsulating peritonitis (SEP), also referred to as abdominal cocoon syndrome, is a rare cause of bowel obstruction characterized by a thickened fibrous peritoneum that encapsulates the intestines. The exact etiology is idiopathic but may be associated with long-term peritoneal dialysis (PD). In the absence of risk factors for adhesive disease, preoperative diagnosis can be difficult and may require operative intervention or advanced imaging to diagnose. Thus, the inclusion of SEP in the differential diagnosis for bowel obstruction is essential for early detection. Existing literature is focused on renal disease as an origin, but it can be multifactorial. Here, we discuss a case of sclerosing encapsulating peritonitis in a patient without known risk factors.
Sclerosing encapsulating peritonitis (SEP), also referred to as abdominal cocoon syndrome, is a rare condition indicated by chronic inflammation of the peritoneum. 1 Sclerosing encapsulating peritonitis is characterized by a thickened fibrous peritoneum that encapsulates the intestines. The proinflammatory agent transforming growth factor b1 (TGFb1) is believed to increase the transcription of collagen type 1 alpha 1 (COL1A1) and fibrogenesis within the mesothelium. 2 The cocooning of fibro-collagenous elements causes reoccurring small bowel obstructions secondary to compression of the enclosed bowel. 1 Like this pathology, SEP often presents as a distended and painful abdomen. Due to its uncommon nature, it is often misdiagnosed.
The cause of SEP is largely idiopathic. The broad scope of symptoms decreases preoperative diagnosis, which often requires advanced imaging or surgical intervention to confirm. The inclusion of abdominal cocoon syndrome in the differential diagnosis is essential for early detection. Sclerosing encapsulating peritonitis has often been associated with long-term peritoneal dialysis (PD), attributed to dialysate’s acidic pH and hyperglycemic nature. 3 Existing literature is focused on nephrological disease as an origin, but it can be multifactorial. In this case report, we discuss a case of sclerosing encapsulating peritonitis in a patient without risk factors.
The patient is a 67-year-old male with a history of COPD, hypertension, CAD, previous stroke on Aggrenox, and type II diabetes mellitus who initially presented with severe, diffuse abdominal pain, nausea, and vomiting concerning for a small bowel obstruction. He had reported two previous self-limited episodes of similar symptoms in the recent past. His last bowel movement was earlier that same day. He reported a normal colonoscopy within the past few years and no prior intra-abdominal surgery. On exam, his abdomen was distended and tympanic but without peritoneal signs. His laboratory studies were unremarkable besides a serum creatinine of 1.7 and lactate of 2.5. Imaging studies were consistent with small bowel obstruction, and an NG tube was placed with 1600 cc of bilious output over the first 24 hours. The patient began to pass copious amounts of flatus on hospital day one, and his distention subsequently improved. The patient had a normal small bowel follow through with contrast in the colon at three hours on hospital day four. That same day, he began to have multiple bowel movements, and the NG tube was removed the next morning. The patient improved greatly and was discharged home on a regular diet on hospital day five.
Two months later, the patient again presented with similar symptoms. His laboratory studies at that time were unremarkable but noted in his CT abdomen pelvis with IV contrast were “several small bowel loops in the mid to lower abdomen appearing to be grouped together around central mesenteric vessels,” as seen in Figure 1. Upon review of imaging performed on first admission, the small bowel loops were noted to be in a similar configuration. Due to this finding and the fact that the patient had continued to have intermittent symptoms since his previous admission, the decision was made to take the patient to the operating room for exploration. Computed tomography findings of distended bowel loops in a similar configuration to imaging from previous admission. This finding prompted diagnostic laparoscopy leading to the diagnosis of sclerosing encapsulating peritonitis.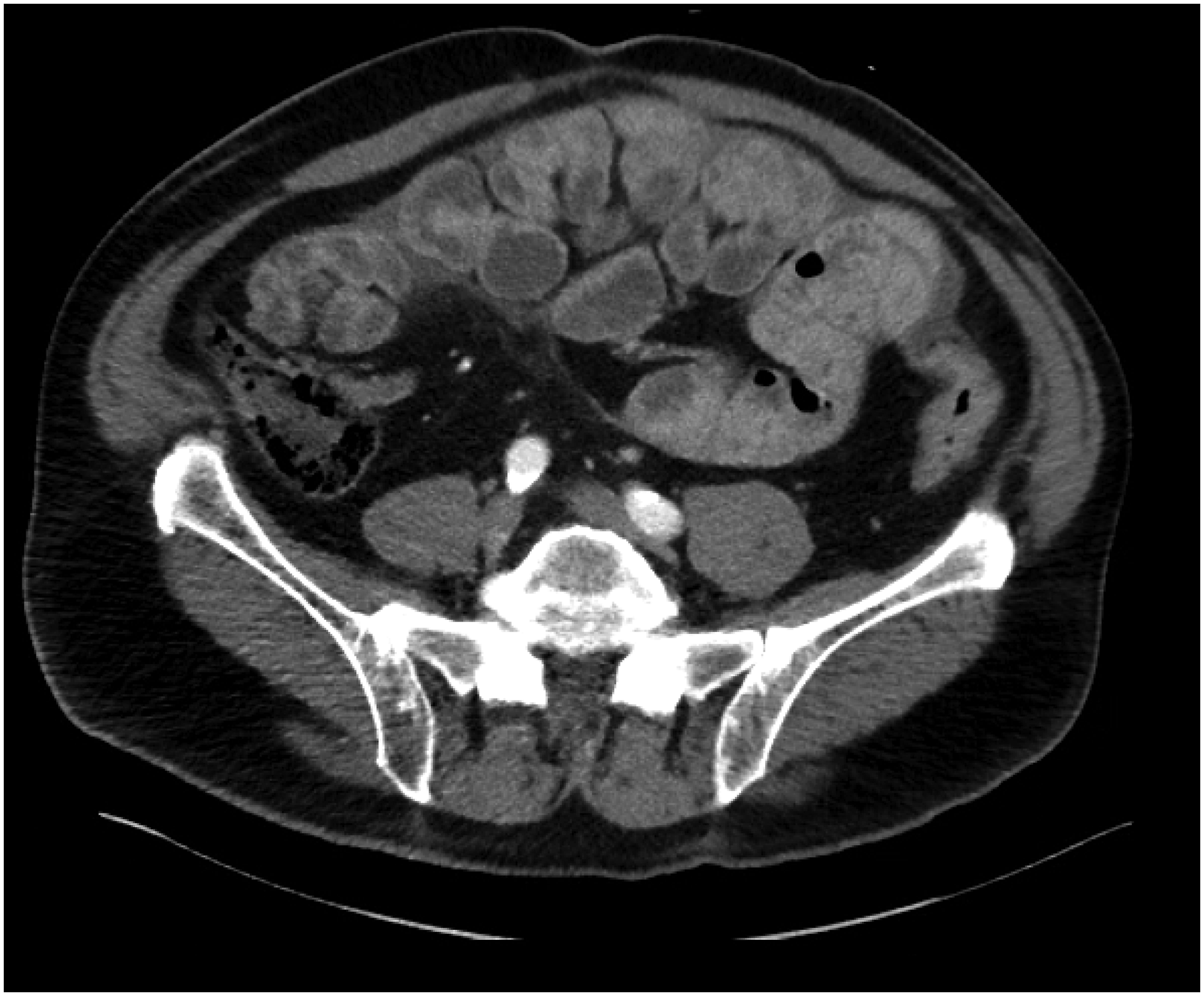
Upon gaining laparoscopic access, a large mass of small bowel was noted, and vision of the remaining abdominal structures was impaired. The peritoneal lining was noted to have a smooth white coating, and there were several nodules noted on the liver. At that time, we converted to an open procedure. Along the course of the operation, the entire small bowel from the ligament of Treitz to the terminal ileum was found to be adherent to itself with a fibrous coating resembling peritoneal lining as seen in Figure 2. A specimen from the peritoneal lining as well as an incidental liver lesion were both sent for frozen section analysis which returned as benign fibrous tissue without the evidence of dysplasia or malignancy. These findings were determined to be consistent with SEP. Given the chronic nature of this condition, the decision was made to place a decompressive gastrostomy tube, and the operation was completed. Intraoperative findings of a fibrous coating encasing the entire length of the small bowel from the ligament of Treitz to the terminal ileum, consistent with sclerosing encapsulating peritonitis.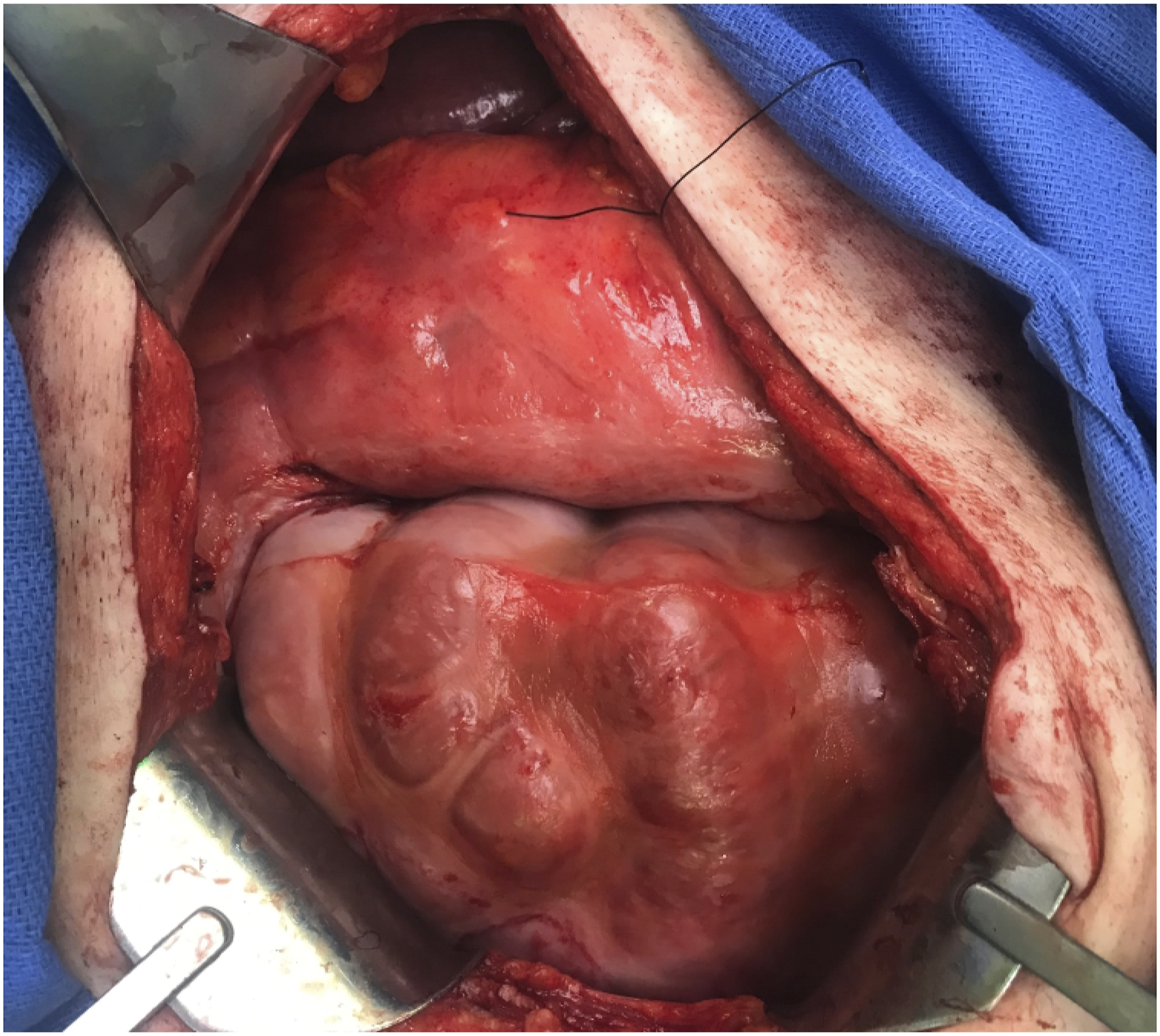
Upon review of the literature, tamoxifen was deemed an adjunct treatment along with an extended steroid taper. The hematology/oncology service was consulted for additional recommendations and long-term follow-up. On postoperative day 1, the patient had a repeat small bowel follow through which showed normal transit of contrast to the colon. The gastrostomy tube was clamped on postoperative day 3, and the patient’s diet was advanced as tolerated. Per oncology recommendations, the patient was then discharged home on hospital day four on tamoxifen 20 mg twice a day and an extended prednisone taper beginning at 100 mg every day for one month followed by a yearlong taper. The patient and his wife were instructed to allow venting of the G-tube should symptoms recur. Additionally, a referral was made to a quaternary care center for further management where exploratory laparotomy for the lysis of adhesions was recommended. Unfortunately, his comorbid conditions were determined to be prohibitive, and no further intervention has been performed to date.
Sclerosing encapsulating peritonitis is a rare but potentially devastating disease of widespread etiology. While secondary SEP is more common and predominantly due to peritoneal dialysis, primary or idiopathic SEP often results in a delayed diagnosis given the absence of risk factors. 2 Many etiologies including retrograde menstruation or gynecologic infection have been proposed, but these are unlikely the most common causes given the disease’s male predominance. 1 A “two-hit” hypothesis has been proposed with an initial insult causing peritoneal injury followed by chronic serosal injury leading to simple sclerosis. The formation of a fibrous cocoon and subsequent encapsulation of the bowel follows a second hit, such as cessation of PD or kidney transplantation. 4 Primary SEP, as seen in this case, does not appear to have any definitive causes.
The presentation is non-specific, with most patients complaining of abdominal pain followed by distension. This can contribute to delayed diagnosis, particularly in the absence of renal disease or surgical history as exhibited in this case. CT imaging is the most used modality and often displays an enveloping, thickened peritoneum with the tethering of small bowel loops. 2 Definitive diagnosis is often determined by surgery with peritoneal biopsy. 1 Due to the rare nature of the disease, there is a lack of standard treatment or guidelines, although observational studies have noted improvement with glucocorticoids, tamoxifen, and nutritional support. 3 Surgical intervention can include enterolysis alone, in conjunction with a Noble plication (suturing of the intestines to each other), or peritonectomy and enterolysis (PEEL). 2 Given the complexity of surgical intervention, it is recommended that conservative management be attempted before surgical referrals are made to quaternary care centers. 3 This case highlights an incidence of a rare disease in the absence of known risk factors. It remains critical to the general surgeon that a high index of suspicion be exhibited when managing recurrent small bowel obstructions without surgical history or evidence of hernias. Additionally, conservative management can be attempted in a rural setting while reserving operative intervention for facilities with extensive experience managing the patient’s disease and postoperative care. Lastly, placement of a decompressive gastrostomy tube has not been described, but it has allowed our patient to manage symptoms of distention and emesis without requiring hospitalization admission. It should therefore be considered whenever SEP is encountered, particularly when comorbid conditions may be prohibitive of more invasive intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.