
Abstract
Basal cell carcinoma (BCC) is the most common skin cancer, and most of the reports have involved the head and neck, but it is rare for it to be highly invasive, with an invasion of long bone being extremely rare. A 73 year old woman presented with a giant BCC on her right arm. Magnetic resonance imaging suggested the involvement of the right humerus. Biopsy confirmed the nodular type of BCC. The patient underwent BCC excision including hemicortical humerus excision with fibula allograft and latissimus dorsi flap with a split-thickness skin graft. Excluding a transient radial nerve palsy, the patient’s postoperative course was otherwise uncomplicated. Although BCC invasion into the long bone is extremely rare, the gold standard treatment is, as a rule, en bloc surgical resection with a wide variety of reconstructive techniques. This treatment is only possible through the collaboration of general surgery, orthopedics, and plastic surgery.
Basal cell carcinoma (BCC) is the most common skin cancer, presenting most commonly on the head and neck. Basal cell carcinoma is also highly locally aggressive and can extend into bone with most reports involving the skull and facial bones. However, a diameter greater than 10 cm or invasion into long bones is extremely rare, and its reconstruction can be more complicated.1,2
The patient is a 73-year-old female, initially presented to clinic for the evaluation of a large, fungating mass on her right anterolateral upper arm. The patient previously sought out care at an outside health care facility 5 years ago and stated she was told it was basal cell carcinoma. Patient was a poor historian, and the reasoning behind the lack of follow-up was unclear. At the time of presentation, mass was noted to be fungating and ulcerative with fleshy everting edges and appeared fixed to the humerus.
Subsequently, an incisional biopsy was performed, pathology confirmed basal cell carcinoma nodular type, and a magnetic resonance imaging (MRI) showed a 7 × 3.1 × 7.2 cm enhancing cutaneous mass with soft tissue extension to involve the adjacent deltoid and biceps muscle, abutting the adjacent humerus with mild periosteal reaction present (Figure 1). Computed tomography (CT) showed no evidence of distant metastasis. MRI showing a 7 × 3.1 × 7.2 cm enhancing cutaneous mass with soft tissue extension to involve the adjacent deltoid and biceps muscle, abutting the adjacent humerus with mild periosteal reaction present.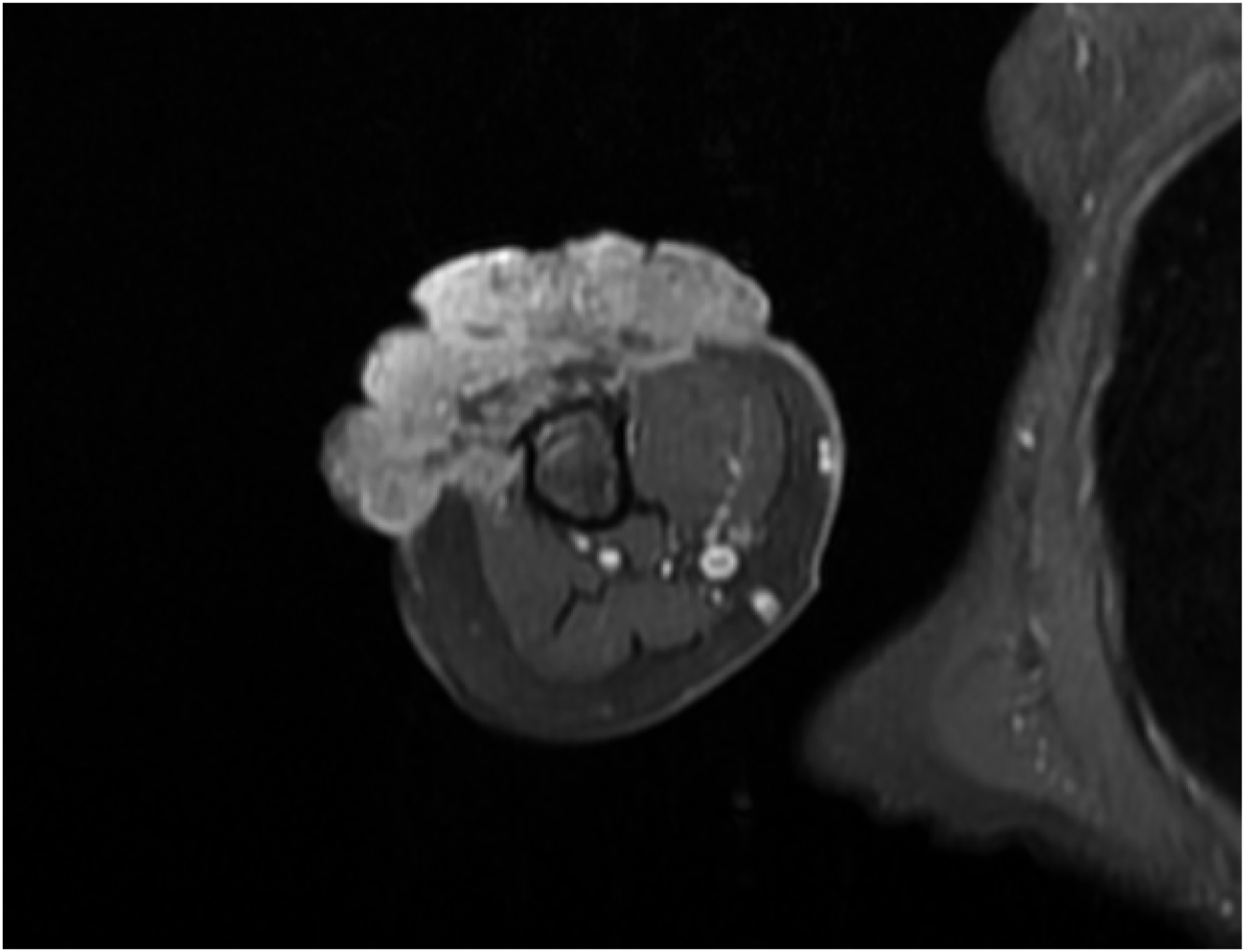
The patient was presented at Tumor Board, and it was collectively determined, due to the chronicity and extent of the lesion with bony involvement, the best care for this patient would require collaboration and surgical planning by general surgery, orthopedic oncology, plastic and reconstructive surgery, and medical oncology to establish an optimal treatment plan.
The patient underwent excision of the malignancy with sufficient margins, including hemicortical excision of the humerus. Reconstruction included a fibula allograft, plating, and finally a latissimus dorsi flap with split-thickness skin graft for primary closure. To ensure the viability of the flap, indocyanine dye spy perfusion was performed which verified excellent inflow and robust perfusion of the flap. Final pathology showed basal cell carcinoma, nodular type, with negative margins. Complication of the surgery included a radial nerve palsy with impaired extension of the right wrist and phalanges. Three months postop, the patient began limited physical therapy of the right arm and has gained improved extension of the wrist. The patient stated that she is overall very pleased with her outcome.
Basal cell carcinoma is a localized, slowly progressive tumor, and cases of distant metastasis or invasion into surrounding tissues are uncommon.1,2 The risk of recurrence and prognosis vary depending on tumor size, location, histological subtype, and immunosuppressive status. Based on these factors, the treatment plan may vary from patient to patient, but surgical resection is currently the standard treatment for BCC. Locally advanced cases with invasion into a long bone are extremely rare but still curable by resection, and the subsequent reconstruction can be more complicated, depending on the site. 3 Radiation therapy may be the treatment of choice if the patient is not a good candidate for surgery. Radiation therapy is also used as an adjuvant therapy in cases where surgical treatment may cause nerve injury. Recently, the efficacy of Hedgehog pathway inhibitors has also been reported in locally advanced inoperable cases, metastatic cases, and postoperative recurrent cases. 4
Although BCC invasion of a long bone is extremely rare, the gold standard treatment is, as a rule, en bloc surgical resection with a wide variety of reconstructive techniques. Multidisciplinary surgical treatment of locally advanced cases such as the present case is only possible through the collaboration of general surgery, orthopedic oncology, and plastic and reconstructive surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.