
Abstract
We describe the case of a 32-year-old female who presented to the emergency department (ED) with a 3-day history of severe epigastric abdominal pain accompanied by nausea, vomiting, and constipation. Past medical history was significant for known right hydrosalpinx and previous pelvic inflammatory disease (PID), without past surgical history. Clinical examination revealed a hemodynamically stable patient with a soft but distended abdomen, tenderness in the epigastric region, without signs of peritonitis. Bloodwork including white blood cell count, electrolytes, and lactic acid was unremarkable. Initial computed tomography (CT) scan of the abdomen and pelvis with contrast demonstrated a small bowel obstruction (SBO) with a transition point in the right lower quadrant, accompanied by mesenteric edema and free fluid. Exploratory laparotomy was performed and revealed obstruction secondary to dense adhesions involving the terminal ileum, appendix, sigmoid colon, and right ovary. Lysis of adhesions, appendectomy, and excision of a right paratubal cyst were performed. Histopathology demonstrated endometriosis of the appendix and a benign paratubal cyst.
Keywords
Small bowel obstructions (SBOs) account for 2-4% of emergency department visits, 15% of hospital admissions, and 20% of emergency surgical operations for abdominal pain. 1 The majority of SBOs are secondary to adhesions from prior abdominal surgery, complex hernias, or neoplasms. 4 Less frequent causes include underlying inflammatory bowel disease, gallstones, volvulus, and intussusception. Obstructions in the absence of previous abdominal surgery are unlikely to resolve with conservative measures and may warrant surgical intervention; suspicion for pathological etiology increases in the absence of surgical adhesions.
SBOs secondary to gynecologic processes such as pelvic inflammatory disease (PID), endometriosis, and ovarian cancer are rare but important etiologies to consider. Pelvic inflammatory disease is an infection of the female reproductive tract caused by sexually transmitted bacteria, which can damage the fallopian tubes and cause hydrosalpinx, a fluid blockage in the fallopian tubes. Endometriosis occurs when ectopic endometrial tissue deposits outside of the uterus. It is known to involve the bowel in rare cases, including the appendix, which can present with nonspecific symptoms that may worsen during menstruation. 3 Pelvic inflammatory disease and endometriosis have both been reported as causes of SBO in female patients; however, there have been no documented cases of SBO secondary to both processes occurring simultaneously. We present a unique case of small bowel obstruction secondary to right hydrosalpinx in the setting of previous PID, as well as endometriosis of the appendix.
A 32-year-old female, with past medical history of right hydrosalpinx and previous PID, presented to the emergency department (ED) with 3-day history of severe epigastric abdominal pain associated with multiple episodes of non-bloody, non-bilious emesis. She denied any past surgical history. Physical exam findings were significant for a softly distended abdomen with epigastric tenderness. Bloodwork was unremarkable for any associated leukocytosis, lactic acidosis, or metabolic abnormalities. Computed tomography (CT) of the abdomen and pelvis revealed multiple dilated and fluid-filled small bowel loops with a transition point in the right lower quadrant, associated mesenteric edema around the distal ileum, and free fluid (Figure 1). Notably, a right hydrosalpinx was present and noted to be present on prior imaging, in addition to a fibroid uterus. Appendix with surrounding free fluid and mesenteric edema (white arrows), with associated small bowel obstruction evidenced by dilated loops of bowel with transition point in the right lower quadrant (red arrow).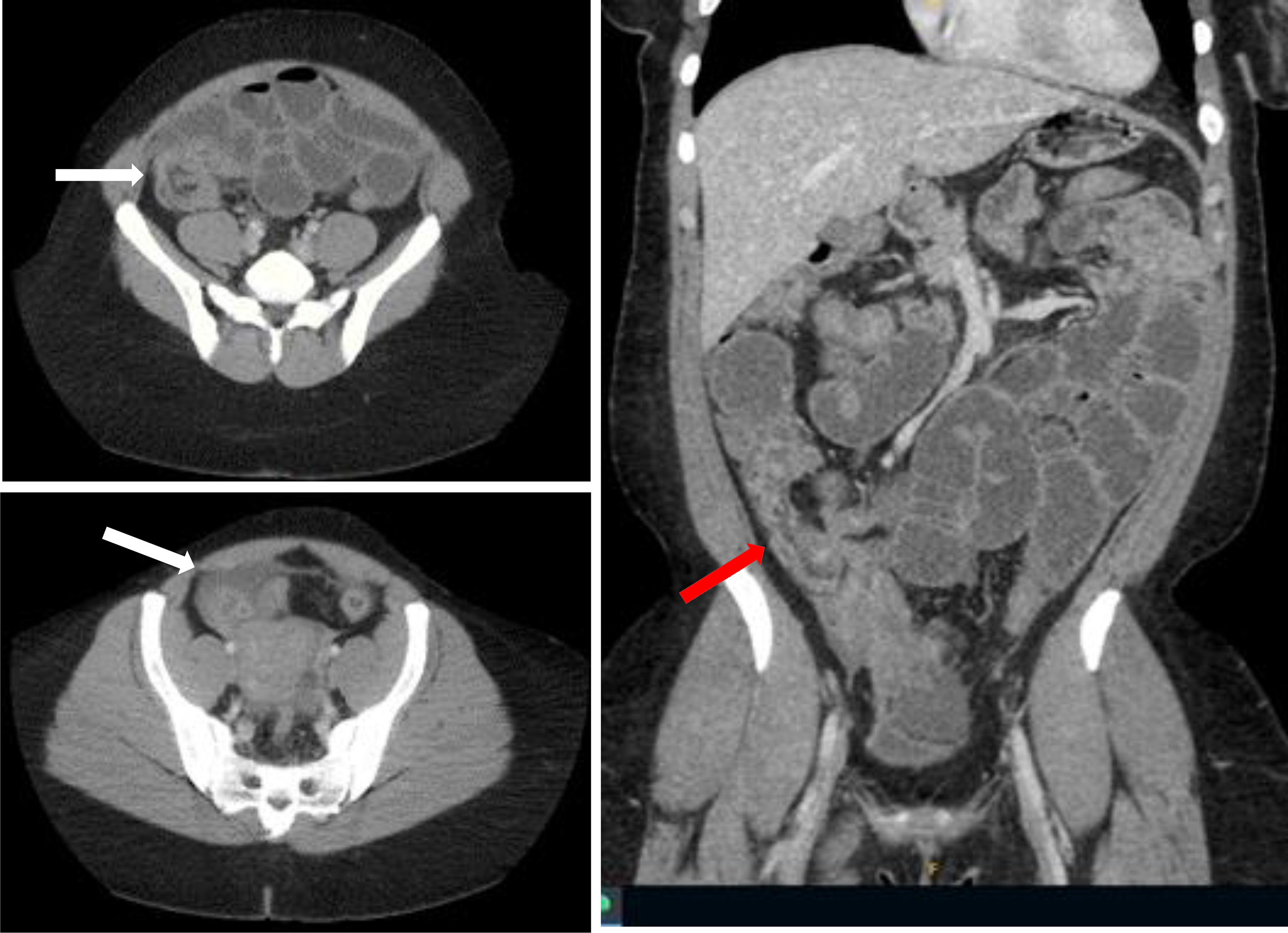
Given these findings, in conjunction with her history of present illness, she was taken to the operating room. Intraoperatively, she was found to have dense adhesions in the right lower quadrant involving the terminal ileum, appendix, sigmoid colon, and right ovary containing a paratubal cyst. An intraoperative gynecology consult was placed, and it was noted that these dense adhesions were likely secondary to pelvic inflammatory disease. Ultimately, a lysis of adhesions, appendectomy, and excision of right paratubal cyst were performed. The patient did well postoperatively and was discharged home on postoperative day (POD) 7 with a 14-day antibiotic treatment for PID. Final pathology showed endometriosis within the appendix and a benign paratubal cyst. She has since seen general surgery and gynecology at 2-week follow-up visits and doing well with plans for elective right salpingectomy.
This is the first case of a small bowel obstruction secondary to adhesions caused by chronic hydrosalpinx in the setting of PID and appendiceal endometriosis. Although gynecologic processes, such as pelvic inflammatory disease and endometriosis, are commonly seen in the hospital setting, they are rare but significant causes of SBO. These etiologies should be considered in the differential diagnosis of a female patient presenting with small bowel obstruction, especially in the absence of surgical history. Few cases have been described in the literature,1-4 and there are currently no recommended guidelines for the management of these patients. Although both successful non-operative and operative approaches have been reported, a thorough history, complete with obstetric, gynecologic, and sexual history, and physical exam are essential when evaluating female patients with small bowel obstructions to aid in clinical decision-making and to prevent such rare etiologies from going unrecognized.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.