
Abstract
Rib plating has been shown to be beneficial among certain populations, such as patients with flail chest and failure to wean from the ventilator in patients without primary pulmonary pathology. Surgical intervention has been shown to decrease ventilatory requirements, decrease pain management modalities, and lower costs. A retrospective data analysis was done to determine the efficacy of rib plating in elderly trauma patients with rib fractures on a total of 244 patients, 63% male and 37% female, mean age is 64 ± 18.5 years, 76% had an associated comorbid condition, such as Diabetes Mellitus (DM), Chronic Obstructive Pulmonary Disease (COPD), Coronary Artery Disease (CAD), Chronic Kidney Disease (CKD), or any combination, with 111 (46%) on anticoagulant therapy. 95% patients presented to the emergency department (ED) with Mild GCS range (13-15). Moderate GCS (9-12) was 4% and 3% of patients Severe GCS (3-8). The overall mortality rate was 4.5%.
Rib fractures in the elderly are one of the most common injuries in trauma patients admitted to the hospital, accounting for over 350 000 patients annually in the United States. 1 Medical management of these cases has not improved the poor outcomes of these patients. Rib plating has been in practice for many years; however, this method has not been popular until recent improvements in technology, which contributed to the current exploration of this technique. 2 The data from various surgical and trauma societies in the United States in support of this procedure has also added to its popularity. Not until recently, the guidelines for rib plating remained unsettled, especially in the elderly patients with rib fractures. 1
Rib fractures are commonly acquired during blunt force trauma to the chest wall. These are typically managed via pain control and oxygen support. More recent support has been given for surgical rib fixation, that is, plating. Rib plating has been shown to be most beneficial among certain populations, such as patients with flail chest, pain refractory to conservative measures, chest wall deformities, and failure to wean from the ventilator in patients without primary pulmonary pathology. As early surgical intervention has been shown to decrease ventilatory requirements, decrease the need for pain management modalities, and lower costs, and with the wake of the current opioid dependence epidemic, it is important to utilize approaches that limit the use of pain medications. This is a retrospective data analysis to determine the efficacy of rib plating in elderly trauma patients with rib fractures.
The medical records of 253 consecutive patients presented to the trauma department at our community hospital with accredited level II trauma, with rib fractures were analyzed from January 2015 to December 2021. Data and variables collected included age, sex, comorbid conditions, anticoagulant therapy, length of stay in both the hospital and ICU, surgical intervention including rib plating, analgesia used, GCS and ICS, and mortality. These patients were divided into 2 groups. Group I consisted of patients who received open reduction and fixation of the fractured ribs, and Group II was patients managed conservatively without surgery. Statistical analyses were used to detect significance at ≤ .05 using Student’s t-test and Chi-square test. Institutional Review Board approval was obtained for this study.
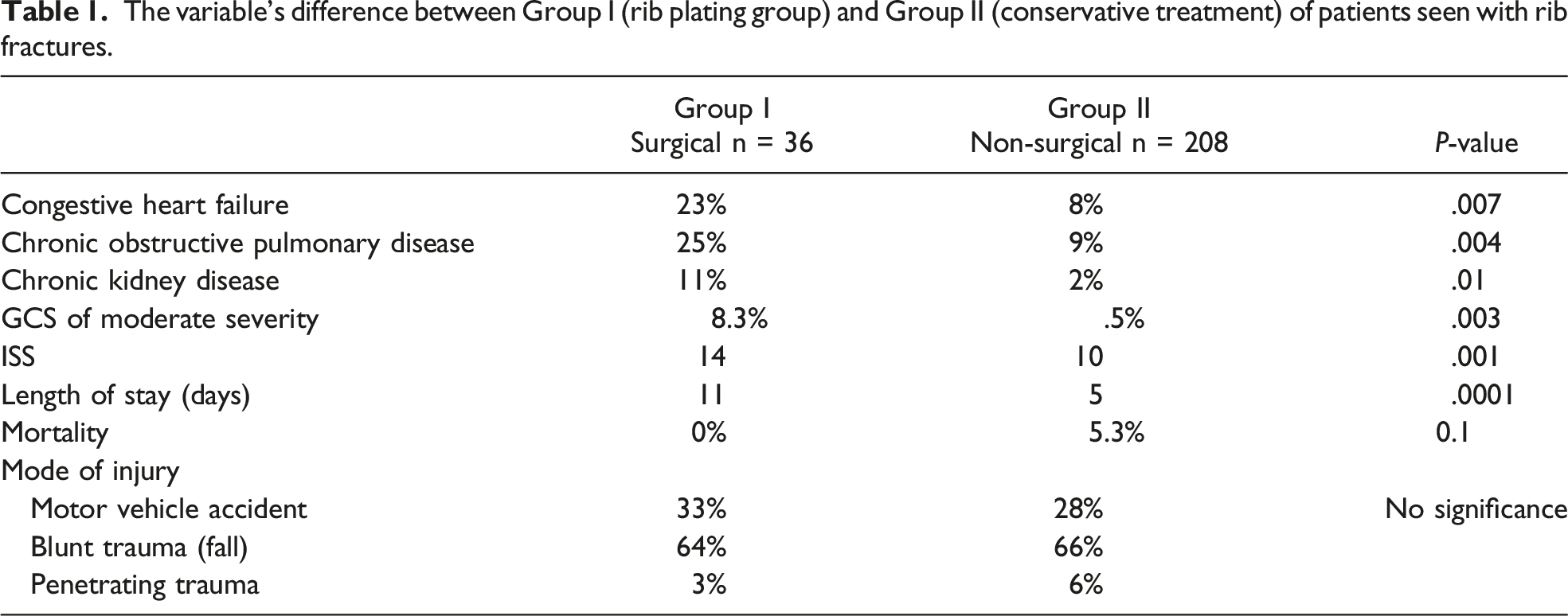
The variable’s difference between Group I (rib plating group) and Group II (conservative treatment) of patients seen with rib fractures.
The idea of rib fixation is not a new concept, as previously wires were used to approximate the ends of fractured ribs together and to reduce unsynchronized mobility of the rib fragments and thus reducing pain. As technology improved, various types of plates and screws were used to approximate and immobilize the fractured ribs, thus adding to the stability of the traumatic chest wall. Despite the popularity of the procedure in recent years, a clear criterion for application remains at most vague and ill-defined. 1
The geriatric population, with their statistically higher rate of osteoporotic fragility fractures and comorbidities, remains the most desirable group of patients to use the surgical approach to rib plating for. This is due to the procedure’s ability to reduce morbidity and mortality by increasing the early mobility of trauma patients. 3 Since early mobility is the prime target for any trauma patient to reduce complications and improve outcomes, rib stabilization combined with early mobility and physiotherapy undoubtedly will result in better results. 4
When considering our experience in rib plating in the elderly patient, the early data showed mortality rate is significantly improved, despite the fact that these patients had higher rates of comorbidities, however, the tradeoff, not surprisingly is a longer length of stay in both the hospital and in the ICU settings.
Early timing of surgical intervention in patients with rib fracture is critical to the success of the procedure, 1 as dissection of the fracture site becomes more tedious and time-consuming once healing starts within 48 hours, with fibrous tissue build up creating more bleeding and difficulty in isolating the ends of the fractured rib.
We elected to offer the procedure to the elderly patients with rib fractures early in admission to the trauma service (within 48 hours) which will undoubtedly benefit the patient as earlier mobility and physiotherapy will aid in reducing pulmonary complications and deep vein thrombosis, which often accompany chest trauma and fractured ribs.
Geriatric patients with multiple comorbidities (as in our patients) including CHF, COPD, Diabetes, CKD, and osteoporosis make them a vulnerable population to fragility fractures. Initial management following admission includes pain control, aggressive pulmonary toilet, and monitoring for complications. Therefore, the prospect of rib plating in this vulnerable population undoubtedly has the ability to improve outcomes. As noted, the majority of our patients who underwent rib plating had higher comorbidities and ISS scores, thus contributing to longer length of stay (Table 1). Nonetheless, the mortality rate of this group was low.
Rib plating in elderly trauma patients with multiple rib fractures has shown to be beneficial in terms of mortality. Furthermore, geriatric patients with comorbidities will benefit from early open reduction and fixation of rib fractures, though a larger study is needed to establish clearer criteria for rib plating.
In addition to being a retrospective study, the sample size limited the study from identifying the relationship of various contributing factors to the outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.