
Abstract
Background
In many academic centers, opioid prescribing is managed primarily by residents with little or no formal opioid education. The present study evaluates intern knowledge and comfort with appropriate opioid prescribing 7 months after an organized opioid education effort.
Materials and Methods
A repeat knowledge and attitude survey was sent to surgical interns who had completed an initial opioid education training session 7 months before the study. Results were compared to post-education assessment results in the same cohort.
Setting
16 general surgery and podiatric surgery interns at a single academic medical center.
Results
The mean percentage of correct answers on follow-up was 67.6% identical to the average post-session score of 67.6%. Interns reported comfort with opioid prescribing increased to a mean score of 5.9 (out of 10) on follow-up compared to post-session score of 5.19.
Conclusions
Surgical interns have significant gaps in knowledge for optimal prescribing and management of opioid prescriptions. Targeted education demonstrates significant and lasting improvement in opioid assessment scores, but there remains room for improvement.
Key Takeaways
• Opioid education has a sustained impact on knowledge and comfort in prescribing • Clinical patient care activities of interns do not increase opioid knowledge or comfort with opioid prescribing
Introduction
The opioid epidemic has resulted in both increased overdose-related morbidity and mortality as well as devastating financial consequences for the United States of America.1-3 Studies estimate that the opioid epidemic has annual societal costs of $53.4 to $55.7 billion; with an estimated annual $23.7 billion in health care associated costs, and $25.6 billion to $42 billion in workplace costs.4,5 Further, the Centers for Disease Control and Prevention (CDC) reports that over 90 000 people have died as a result of drug overdose in the United States in 2020 with opioids accounting for increasing rates of drug overdose deaths. 6
Opioid pain medication accounts for over a third of all prescriptions written by surgeons. 7 In academic medical centers, postoperative discharge instructions and prescriptions are commonly completed by resident physicians, and often are the responsibility of junior residents who have the least training and experience with pain management and prescribing narcotics. A study on pain education in North American medical schools found that pain management education is often fragmented and lacks dedicated sessions or skills training. 8 However, graduating medical students heading into their intern year are expected to start residency with a knowledge base that allows them to write safe and appropriate opioid prescriptions. Additional studies report that under 10% of surgical residents complete formal opioid education and instead report modeling prescribing habits based on their attending or senior resident’s preference. 9 Another study reported that only 20% of surgical residency training programs mandated formal opioid prescribing education sessions. 10 It is reported that there is wide variability in the number of opioids prescribed for common outpatient surgical procedures. 11 Survey studies have demonstrated that surgeons prescribe more opioid medications following a procedure than patients consume with 67-77% of patients reporting surplus unused opioids, and 61.5% of all prescribed opioids were not used by patients.12,13 This modeling of prescribing behavior by junior surgical residents is argued to be a major factor in the continued trend of inappropriate opioid prescribing.
Another study by Walk et al. investigating the perceived number of narcotics prescribed compared to actual number of narcotics prescribed demonstrated that residents, attending surgeons, and advanced practice providers (APPs) prescribe twice as much narcotics as they thought. Further, all three groups prescribed more narcotic than the current guidelines recommend with a median of 120 morphine milliequivalents for laparoscopic appendectomy and cholecystectomy. 14
The previously mentioned studies demonstrate that there is a lack of formal opioid education for surgical prescribers, and most prescribers are unknowingly prescribing an excessive amount of opioid pain medication following surgical procedures. Previously, our study investigated the opioid prescribing knowledge and comfort of surgical interns following a 75-minute educational session during orientation week demonstrated improvements in objective knowledge and subjective comfort level with opiate prescribing. 15 The present study compares surgical interns’ comfort level with opioid prescribing and knowledge about opioids for treatment of acute pain after an opioid education session to their knowledge and comfort half way through their intern year.
Materials and Methods
As we previously reported, 15 an opioid education curriculum was designed by a multidisciplinary team of surgeons and anesthesiologists to teach incoming surgical interns basic pain management techniques and appropriate use of both opioid and nonopioid pain medications to achieve pain control in surgical patients while minimizing the risks of opioid misuse and abuse. 15 The curriculum was designed as a 75-minute didactic session which included several key components: a review of pain medications, dosing, indications and contraindications, identification of patients at high risk for uncontrolled pain and patients at risk for opioid misuse or abuse, patient monitoring and care plans, and state and federal legislation. In addition to the formal didactic teaching session surgical interns were given access to pocket reference cards and an online database available through the medical center’s network to use as a reference when prescribing opioids for patients following surgery. This online database provided the median and interquartile range of patient-reported opioid requirements following common surgical procedures. Users could add modifiers depending if the surgery was minimally invasive or open, if the patient was opioid naïve or has a history of opioid exposure, or abuse. Users were also able to select different opioid pain medications and the number of pills would be adjusted to reflect the appropriate morphine milligram equivalents to be prescribed.
To evaluate changes in knowledge all incoming surgical interns took an anonymous, de-identified, 11-question opioid knowledge assessment (Opioid Knowledge Self-Assessment, Patient Safety Authority; 2013) both before and after a 75-minute education session. 16 This knowledge assessment was designed by the Pennsylvania Patient Safety Authority and has previously been administered to prescribers, pharmacists, and nurses.17,18 In our prior study, both non-designated preliminary residents and categorical general surgery interns at two Accreditation Council for Graduate Medical Education (ACGME) accredited general surgery training programs were included in the education session and assessments as well as fourth year medical students who had already matched into general surgery or a surgical sub-specialties and would be completing a surgical intern year. 15
For the present study, 7 months following completion of the initial opioid education curriculum, the follow-up assessment was sent to all 16 intern residents at our academic medical center who had completed the initial study. All participation in the study was voluntary, and the study was approved under exempt status by the institutional review board at Beth Israel Deaconess Medical Center.
The assessment presents four clinical scenarios followed by questions about that clinical scenario, there are an additional three questions without a case scenario. The assessment questions aim to assess knowledge in one of three categories including general opioid medication and dosing knowledge, patient-specific characteristics that require alterations in dosing, and patient monitoring and treatment adjustments. The assessment also asks residents to rate their comfort with their knowledge and readiness to prescribe opioids on a scale of 1-10 where 1 indicated “very uncomfortable” and 10 indicated “very comfortable.” The assessment questions are presented in full in the Appendix.
Post-education assessment scores were compared to follow-up results using a paired student’s t-test. Statistical analysis was completed in STATA Version 15.1 (StataCorp, College Station, Texas).
Results
57 interns and fourth year students from our affiliated medical school (all beginning a surgical internship) were included as part of a series of intern education sessions for multiple hospitals from April to June. Seven months later, in January, the following year, a group of 16 interns at a single institution completed the same opioid knowledge assessment (Figure 1). Study participants flow chart.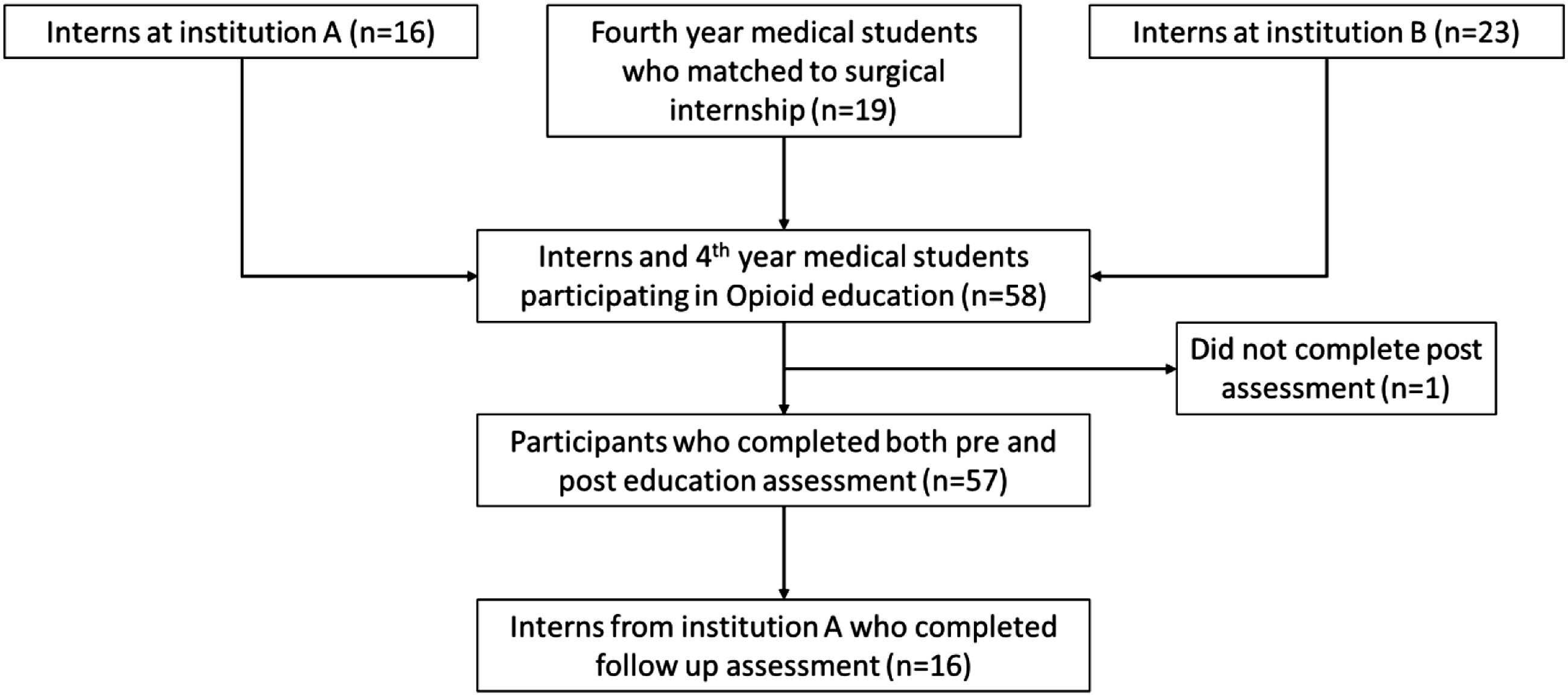
Pre-, Post-education, and 7 Month Follow-up Assessment Scores.
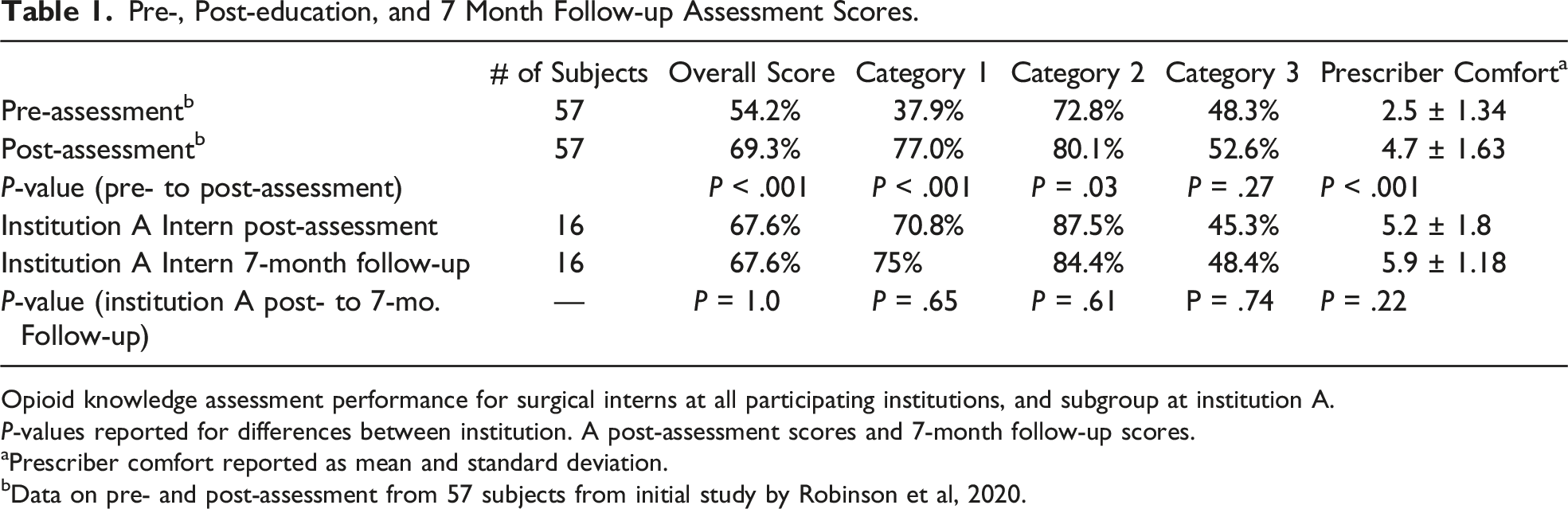
Opioid knowledge assessment performance for surgical interns at all participating institutions, and subgroup at institution A.
P-values reported for differences between institution. A post-assessment scores and 7-month follow-up scores.
aPrescriber comfort reported as mean and standard deviation.
bData on pre- and post-assessment from 57 subjects from initial study by Robinson et al, 2020.
Subjective scoring on questions regarding comfort with opioid prescribing averaged 5.2 out of 10 (range 2-8) on post-education session assessment. On 7-month follow-up, comfort with opioid prescribing increased to a mean of 5.9 (range 4-8). This difference was not statistically significant (P = .22) (Table 1).
Discussion
Incoming surgical interns have significant knowledge gaps when tested using a standardized opioid assessment tool. Further, they report feeling uncomfortable with prescribing opioids when starting their surgical residency. Our previous study demonstrated improvements in objective knowledge and subjective comfort level with opiate prescribing following a 75-minute educational session. 15 The current study demonstrates that residents maintain the knowledge obtained during these educational sessions, however based on sub-category assessment performance, they displayed similar knowledge gaps in opiate prescribing. Further, surgical interns continued to report feeling uncomfortable with their knowledge pertaining to pain control and opiate prescribing. These findings demonstrate that surgical residents continue to have knowledge deficits and discomfort with opioid prescribing and they are not effectively taught optimal opioid prescribing practices in their day-to-day clinical activities.
These results suggest that while targeted opioid education sessions demonstrate significant and lasting improvement in both opioid assessment scores and prescriber comfort, there remains room for improvement and surgical trainees may benefit from further opioid specific education to improve prescriber comfort and knowledge. There are multiple factors that may account for the continued knowledge and comfort gap in opioid prescribing observed at 7-month follow-up. It is possible that the patient examples covered in the education session were not sufficient in complexity compared to real life clinical scenarios that surgical residents encounter in practice. Further, the topics covered during the single education session may not have adequately addressed all of the issues that surgical interns encounter during day-to-day clinical practice which would result in continued discomfort and opioid prescribing. Surgical interns may benefit from additional didactic teaching sessions and more complex patient scenarios.
In a previous study, Freedman-Weiss et al. distributed an evidence-based reference card for postoperative analgesia to surgical residents. Their study demonstrated that 58% of residents utilized the card monthly, and 48% of junior residents reported using the card on a weekly basis. Further, 82% of surgical residents reported that utilization of the reference cards changed their prescribing practices. 19 In our study, interns were provided with a reference resource in the form of pocket reference cards and an online database available through the medical center’s network to reference when prescribing opioids for patients following surgery. Utilization of this resource by residents was not tracked in the current study, perhaps increased promotion of this resource would remind residents of the easily accessible references for residents to feel more comfortable in their day-to-day opioid prescribing.
A previous survey study of program directors in surgical residency demonstrated that 94.5% of surgical residency programs allow residents to prescribe outpatient opioids while only 20% of programs have mandatory opioid prescribing education. 10 However, multiple surgical residency training programs are starting to institute formal opioid education sessions for surgical residents. One study reported improved accuracy of opioid prescriptions following education sessions, but revealed that surgical residents prescribed more opioids following the education session compared to prior; there was no statistically significant improvement in subjective prescriber comfort with opioids following the education session. 20 Another study demonstrated a reduction in the number of opioids prescribed following common surgical procedures by 53% following formal opioid education at their institution. 21 While previous studies are able to demonstrate the short term effectiveness of formalized opioid education sessions on prescriber opioid knowledge and prescribing behavior, to our knowledge this is the first study investigating the retention of opioid prescribing knowledge in surgical interns following formal opioid education and months of clinical training on surgical services.
The current study is a follow-up assessment of opioid knowledge in surgical interns at a single institution 7 months following completion of an opioid education curriculum during intern orientation. In our study, we found that surgical interns continued to demonstrate knowledge gaps and reported feeling uncomfortable in their opioid prescribing knowledge. Given the small sample size of the follow-up group, the sample size for statistical analysis remains small and it is difficult to draw correlations between opioid assessment scores and provider comfort with prescribing on follow-up. Additionally, the 7-month follow-up assessment was conducted with residents at a single institution for this study and may not be generalizable other surgical training programs. In addition, testing conditions for the 7-month follow-up were different than for the initial study. The follow-up assessment was conducted in an unmonitored setting where residents were instructed to work independently and not look up answers while the pre- and post-education assessments were taken in a monitored and controlled setting.
As part of this study, we evaluated resident knowledge and comfort with opioid prescribing, but we did not evaluate prescribing practices of the study participants. Ongoing studies will evaluate the prescribing practices of surgical residents following participation in formal opioid education sessions to determine the effectiveness of opioid education on opioid prescribing. Our research and the findings of similar studies on opioid education continue to demonstrate the effectiveness of opioid education programs for surgical residents in improving prescriber comfort and encouraging appropriate prescribing habits for post-surgical analgesia. These results imply that there remains room for improvement and surgical trainees may benefit from further opioid specific education to improve prescriber comfort and knowledge beyond a single educational session.
Conclusions
Upon completion of medical school training, surgical interns have significant gaps in knowledge for optimal prescribing and management of opioid prescriptions. Participation in a targeted opioid education curriculum has demonstrated a significant improvement in opioid assessment scores and prescribing comfort. However, following 7 months of clinical experience, surgical interns did not demonstrate continued improvement in assessment scores or prescribing comfort for opioids. While a formalized opioid education curriculum demonstrated promising improvement in opioid prescribing knowledge, there remains room for improvement in preparing surgical interns for safe and effective opioid prescribing practices.
Footnotes
Author Contributions
Kevin Arndt MD, MS: Drafting and approval of the manuscript, statistical analysis, distribution and interpretation of the opioid knowledge assessments. Kortney Robinson MD, MPH: revision and approval of final paper, statistical analysis, education leader for opioid education sessions. Brian Yorkgitis DO: revision and approval of the final paper, study conception, and design. Gabriel Brat MD MPH: revision and approval of the final paper, study conception, and design.
Declaration of conflicts of interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.