
Abstract
Background
Surgical specialties represent the most competitive residency positions to obtain, and applicants for these spots may apply to increasingly more programs in an attempt to match. We describe trends in residency applications across all surgical specialties from 2017 to 2021 application cycles.
Materials and Methods
This review of the 2017, 2018, 2019, 2020, and 2021 surgical residency application cycles used the American Association of Medical Colleges’ Electronic Residency Application Service (ERAS) databases. Data from a total of 72,171 applicants to United States surgical residencies during the study’s time period were included. The 2021 ERAS fee schedule was used to calculate the cost of applications.
Results
The number of applicants across the study interval remains unchanged. Trends suggest more women and underrepresented minorities in medicine are applying to surgical residencies today compared to 5 years ago. The mean number of applications per applicant increased 32.0% from 39.3 in 2017 to 51.8 in 2021, resulting in an increased application fee cost of $329 per applicant. Mean total cost for application fees alone in 2021 were $1211 per applicant. In 2021, the cost of applying to surgical residency for all applicants was over $26 million, a nearly $8 million increase from 2017.
Conclusions
There has been an increase in the number of applications per applicant in the past 5 residency application cycles. Increased applications create barriers and burdens for applicants, and residency program personnel. These rapid increases are unsustainable and require intervention, although a viable solution has yet to be elucidated.
Key Takeaways
• The number of applications submitted per applicant has greatly increased recently. • Enhanced volume of applications is detrimental to applicants and program personnel. • Financial cost of applications is notable, particularly when accounting for loans. • Signaling in otolaryngology did not decrease applications per applicant.
Introduction
Applying to residency, in many ways, represents the pinnacle of medical school. 1 Medical students synthesize hours spent studying a myriad of information from biochemistry to physical examination skills in order to determine which specialty training they would like to pursue. 2 After years of education, applying to residency remains a stress-inducing and anxiety-provoking process for many students.1,3,4 This is caused, in part, by a highly competitive applicant cohort seeking a limited number of residency spots.5–7 This foundational principle of scarcity and the allocation of limited resources is crucial to understand residency applicant behavior. 7
Reports in individual specialties have lamented rising numbers of residency applications being submitted annually.8–18 Surges in application number have multifold effects. 19 These include raising the quantity of administrative screening of applications for residency programs and introducing added incremental costs for residency applicants. Various approaches have been proposed to mitigate or reduce this year-over-year increase though clear solutions to the problem have yet to be elucidated.7,8,15,19–21 Surgical specialties as some of the most competitive application processes within medicine have been impacted by these trends.10–12,22
The objective of this manuscript is to longitudinally compare the number of residency applications submitted across the surgical subspecialties. Secondarily, the cost associated with these applications will be estimated. We hypothesize an increase in the number of applications submitted and an increase in cost of applications.
Methods
The American Association of Medical Colleges (AAMC) and Electronic Residency Application Service (ERAS) websites were used to obtain application information.23,24 Data from these websites were collected for the 2017, 2018, 2019, 2020, and 2021 United States (US) residency application cycles. Information collected included number of applicants, average number of applications per applicant, sex, and race/ethnicity. Applicants to the residency programs in general surgery (preliminary and categorical), neurological surgery, obstetrics and gynecology, orthopedic surgery, otolaryngology, plastic surgery (integrated), thoracic surgery (integrated), urology, and vascular surgery (integrated) were included. In total, 72,171 applicants’ information was reviewed. This study was performed using publicly available information, did not include human subjects, and as such was Institutional Review Board exempt.
Costs were calculated using the ERAS 2021 fee schedule for number of applications paired with the number of applicants and the average number of applications per applicant. 23 Costs were adjusted to understand true burden through the implementation of a 4.3% fixed interest rate, the current best interest rate for federal loans, across application costs over a 10-year payback period. Descriptive statistics were run as appropriate using Microsoft Excel (Microsoft Corp.; Redmond, WA).
Results
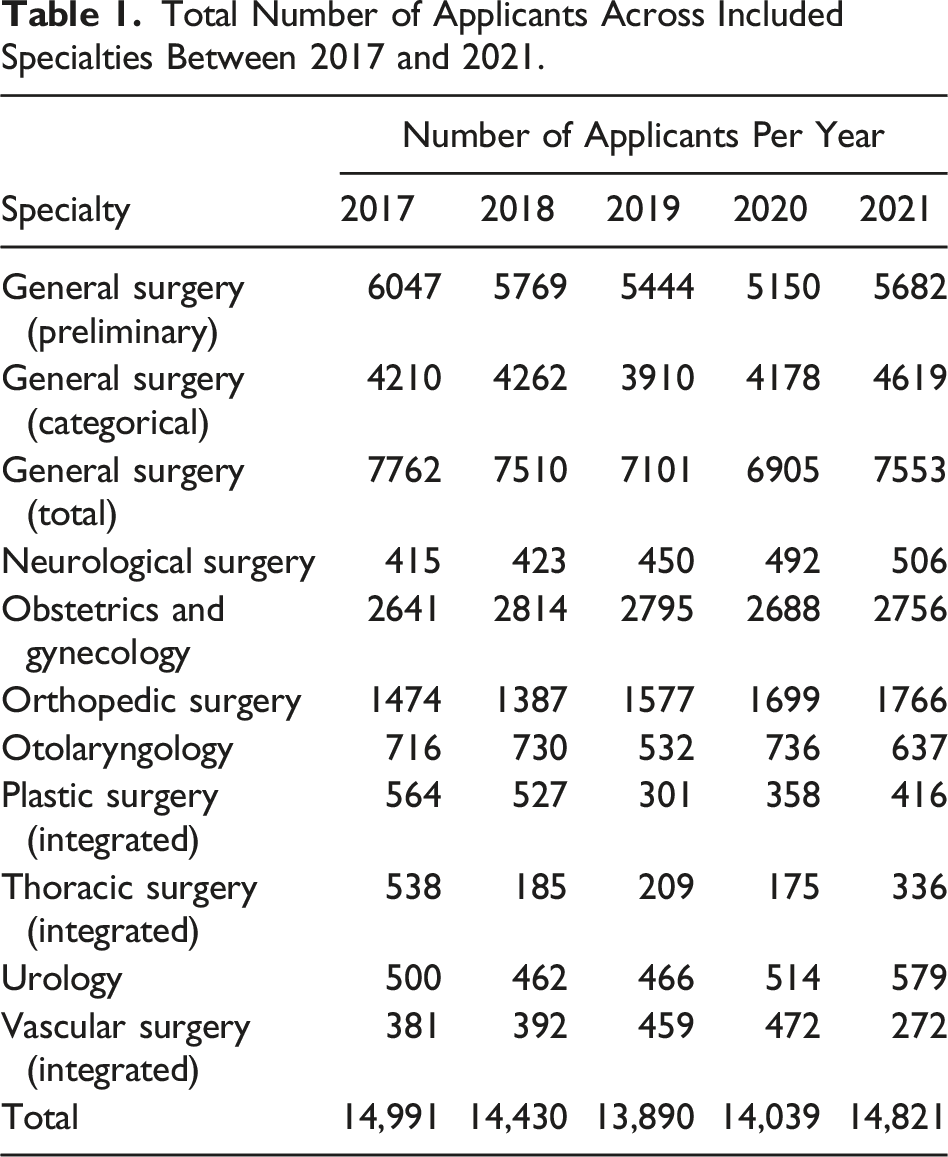
Total Number of Applicants Across Included Specialties Between 2017 and 2021.
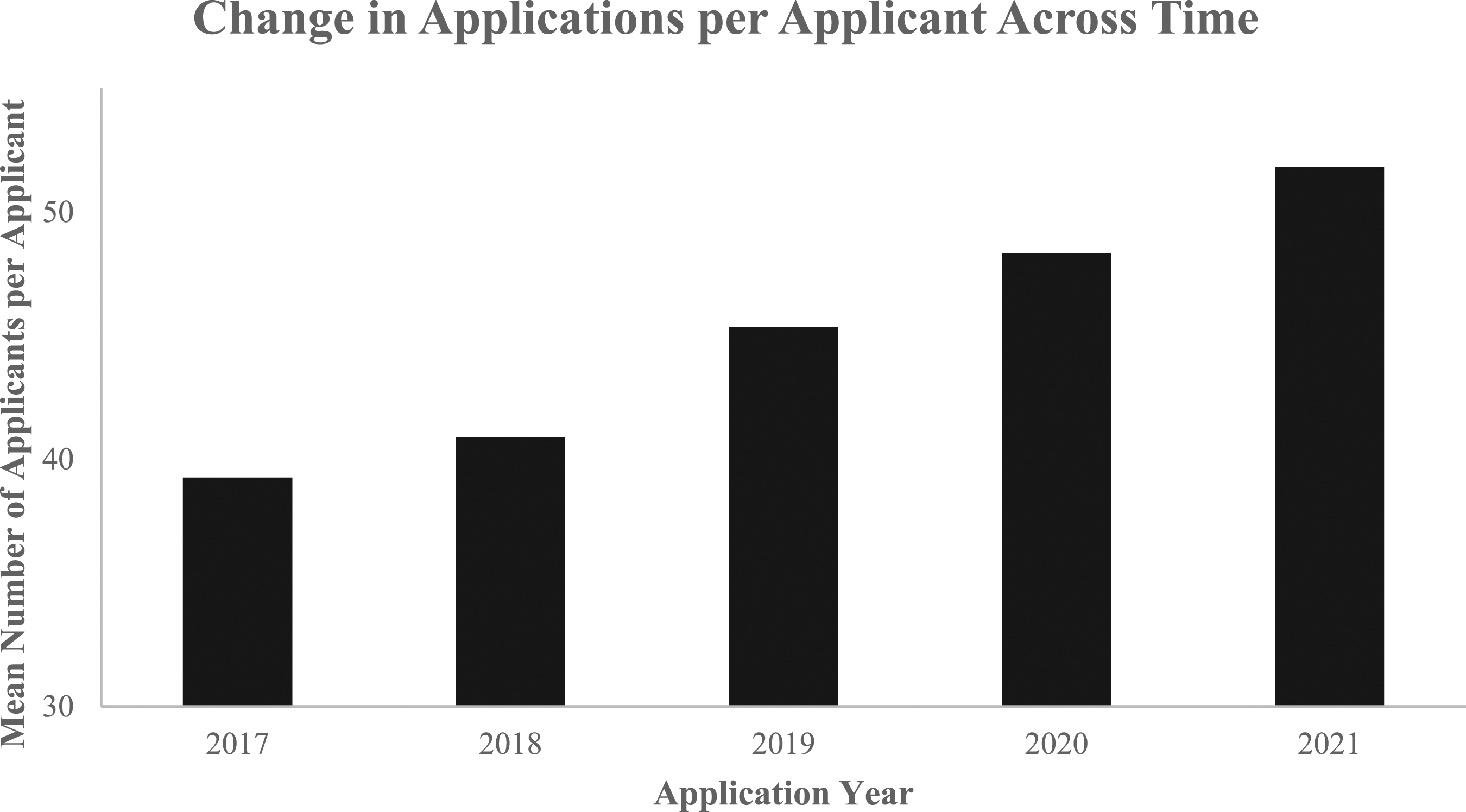
Change in number of applications per applicant across included specialties from 2017 to 2021.
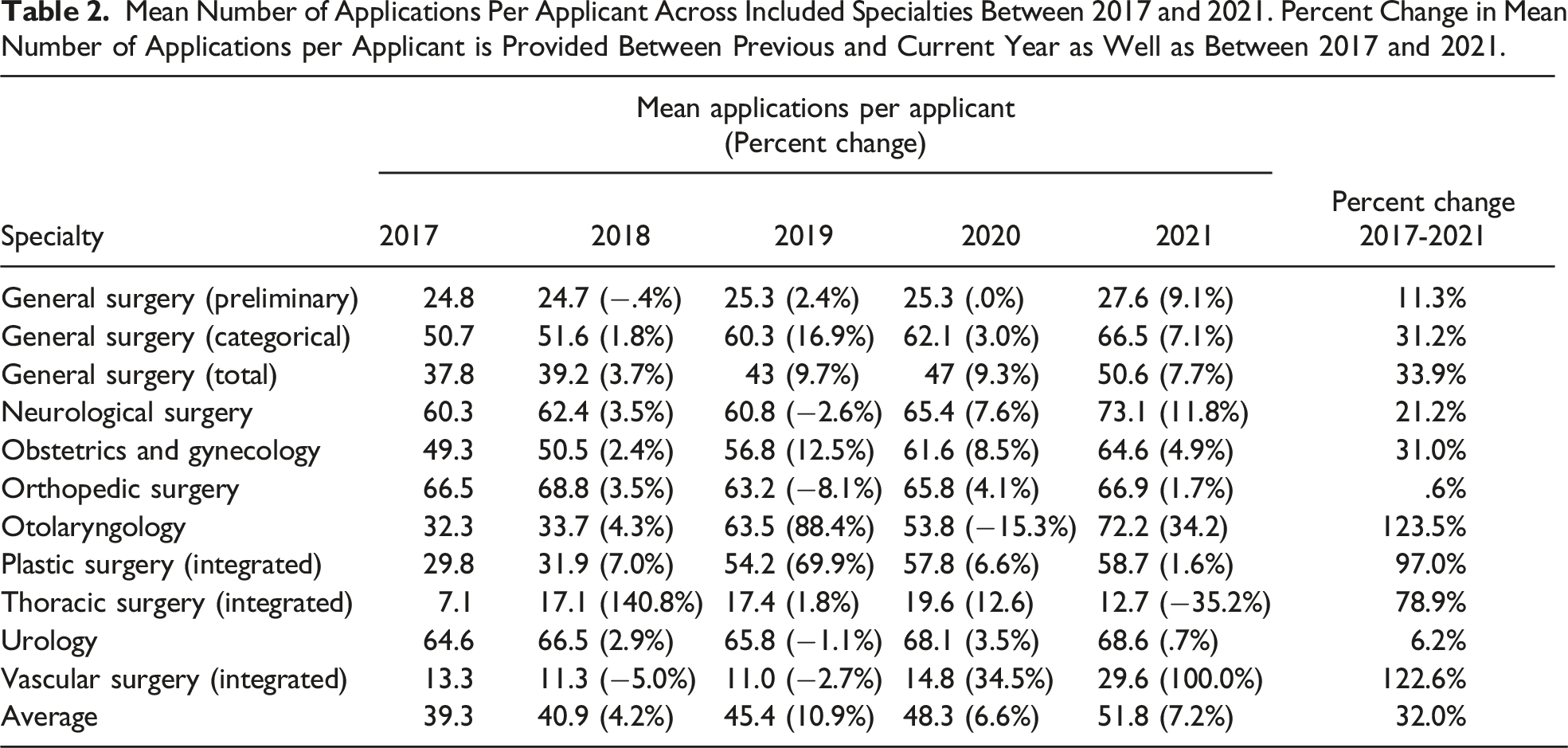
Mean Number of Applications Per Applicant Across Included Specialties Between 2017 and 2021. Percent Change in Mean Number of Applications per Applicant is Provided Between Previous and Current Year as Well as Between 2017 and 2021.
Men represented the majority (58-62%) of surgical residency applicants from 2017 to 2021. Throughout the study interval, the number of women applicants rose by 12% and the number of men applying decreased by 8%, increasing women’s collective representation from 38% to 43%. Across the 5-year cohort, large increases in number of women applicants were noted in general surgery (categorical) (30%), neurological surgery (58%), orthopedic surgery (36%), urology (22%), and vascular surgery (integrated) (780%).
In 8 of the 11 included specialties, mean applications per applicant appeared similar between men and women. Women applied to more programs on average in obstetrics and gynecology (13 additional applications), orthopedic surgery (3 additional applications), and plastic surgery (5 additional applications) when compared to men.
From 2017 to 2021 there was an increase in the number of applicants who self-identified as Black or African American (19%) Hispanic, Latino or of Spanish Origin (22%), and White (5%) and a decrease in those who self-identified as Asian (−3%) and Other (American Indian, Native Hawaiian, other race, and unknown race) (−17%).
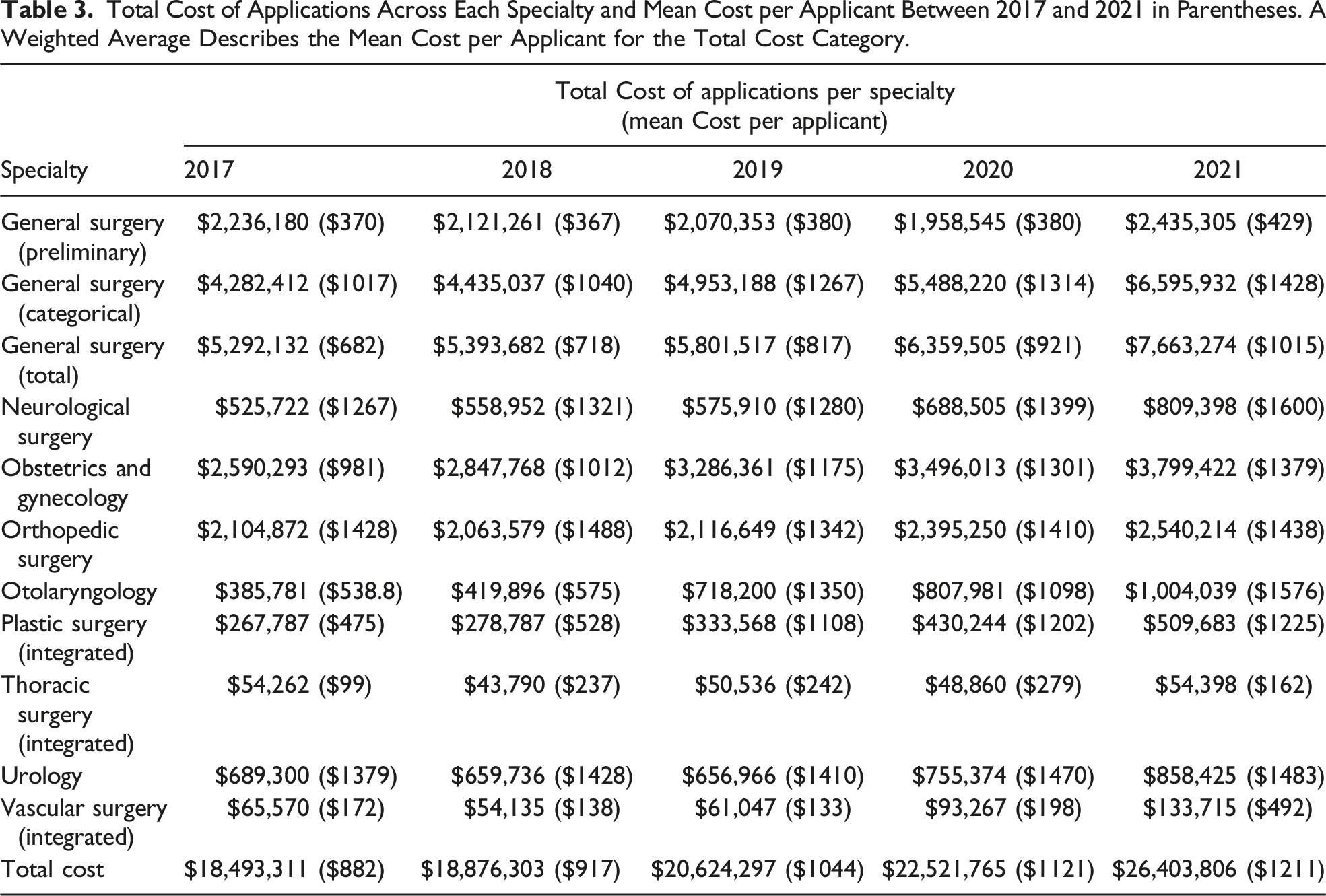
Total Cost of Applications Across Each Specialty and Mean Cost per Applicant Between 2017 and 2021 in Parentheses. A Weighted Average Describes the Mean Cost per Applicant for the Total Cost Category.
Discussion
Analysis of ERAS application data from surgical subspecialties reveals a general high increase in residency applications over the past 5 years. This increase demands additional administrative application review by programs while introducing substantial increases in cost to applying medical students. 26 Given how invested various stakeholders are in improving the residency application process, the results of this study beckon several important considerations.
When calculating the cost estimates for medical students who by in large rely on loans to fund their education, it is naïve and inappropriate to simply look at the cost of applications today.27,28 Instead, we must consider the future value of the costs associated with applying to residency. In an attempt to avoid overestimating the true cost of applying to surgical residencies, we chose the most conservative metrics possible for our calculations. We assumed a 4.3% fixed interest rate (current federal rate) paid back in full by year 10. 28 It is important to note that some medical students may not have loans and others may have loans forgiven through the public service loan forgiveness system. Still, based on these assumptions, application fees alone have increased by 42.7% from ERAS 2017 to ERAS 2021. The future value of costs for applicant fees to surgical residencies totals over $40 million. Applying to surgical residency is a multi-million-dollar industry. Medical students, programs, and governing bodies must be made aware of this high cost.29–33 All parties have a responsibility to work collaboratively to reduce this economic burden bestowed upon medical students.
Increases in applications in the ERAS 2020 and ERAS 2021 application cycles are difficult to attribute to a singular cause. The coronavirus disease 2019 (COVID-19) pandemic thrust instability and uncertainty into the traditional residency application structure.34,35 Critical elements of prior residency application process including audition rotations and in-person interviews were suddenly taken away given social distancing protocols and safety priorities.36–38 In response to uncertainty, some propose that humans are biased toward actions that either enable them to mitigate the effects of uncertainty or gain additional control over the ambiguity. 39 It is possible that given decreased overall travel and lodging expenditures associated with the absence of audition rotations and in the wake of virtual interviews, surgery applicants may have been willing to spend more money on additional applications. A 2021 review of the integrated plastic surgery application process found that on average, applicants spent $6690 on total application cost. 33 The highest cost in our analysis was for neurological surgery in 2021, with an average application cost of $1600. The reduced cost of travel likely greatly outweighs the increased cost of applications. By applying to more programs, applicants may have sought to limit the effects of uncertain circumstances introduced by the COVID-19 pandemic and increase their likelihood of obtaining a residency interview. Receiving an interview invitation, however, is a non-random event largely confounded by the merit of the individual’s application. Interview hoarding was another well-described phenomenon across numerous specialties in the ERAS 2020 application cycle, in which applicants who received a large number of interview invites, held onto and attended more interviews than they would have traditionally in an in-person setting.4,16,18 Hoarding behavior by higher tiered applicants resulted in fewer interview invitations for certain students.18,40–42 Both anecdotal tales of this phenomenon from disgruntled ERAS 2020 applicants in addition to literature reports may have influenced the higher number of applications submitted by ERAS 2021 students.
Another development that occurred in response to the COVID-19 pandemic was a selection bias for home students occurring at higher rates than previous application cycles.43,44 This phenomenon created such stir amongst the plastic surgery community that six manuscripts have already been written and published on the topic in the past year.44–49 These trends are contextualized by recent literature discussing the importance of applicant familiarity for determining appropriate applicant fit within a program.38,50,51 Seeing the effects of home program bias in the ERAS 2020 application cycle, many students may have responded by applying to more programs. Of note, “home-field advantage” is extremely detrimental to applicants who may not have a home program in the given surgical specialty they are applying to including international medical graduates. 43
Applicant preference signaling has been proposed as a solution to residency application inefficiencies.52–54 Signaling is an approach for programs to identify applicants who are highly interested and seriously considering their program, and as such applicants signal a select number of programs to express their genuine interest. A recent report from the otolaryngology experience describes widespread enthusiasm with results achieved through preference signaling and suggest its alleviating effects on over application and interview hoarding. 52 Data from the AAMC, however, reveals that otolaryngology saw a 34.2% increase in the number of applications from the first year of signaling (2021 Match) to the second year of signaling (2022 Match). This observed rise in the number of applications costs increased the application fees by nearly $500 per applicant, leading to a total increase in cost of over $300,000 today and over $460,000 when extrapolated to its future value. As discussed elsewhere, it is impossible to distill an observation to one causal effect given the multifactorial nature of applying to residency coupled with the effects of the COVID-19 pandemic. At this point, the effect of signaling remains unclear and further assessment is required to determine potential benefits of preference signaling. 52
Close examination of the trends observed in the orthopedic surgery application cycle are warranted given that the field maintained the lowest fluctuation in the number of applications per cycle. From 2017 to 2021, orthopedics observed only a .6% increase in the mean number of applications per applicant. Other surgical fields in the same timeline saw increases in applications per applicant range from 6.2% to 123.5%. The stability of application numbers in the orthopedics may be explained by several possibilities. Orthopedics has demonstrated a well-correlated growth between new residency positions and the number of applicants in contrast to other fields which document a growing discrepancy.16,55 Furthermore, reports in the orthopedic surgery literature document that applying to more programs is not associated with greater success in the Match. 10 Further analysis is warranted to illuminate potential factors contributing to the stability seen in the orthopedic application cycle.
The data suggests that there are more women applying for surgical residencies today than 5 years ago. This trend was particularly noticeable in several surgical subspecialties including neurosurgery, orthopedic surgery, urology, and vascular surgery. More female medical student interest and applicants to surgical residencies is the first step in increasing female representation in surgery.56–59 The mean number of applications per applicant between men and women were similar in the majority of specialties. In the three specialties where women on average applied to more programs per applicant, the significance of these differences in not able to be readily explained by the data itself. Further examination of these differences, however, is warranted to ensure applicants are not being discriminated against in the application process or being required to spend additional money on application fees to be competitive based on their sex.
The United States Medical Licensing Examination (USMLE) Step 1 transitioning from numeric scoring to pass/fail reporting may further increase application volume. This may be due to the loss of this historically objective metric for which applicants could determine their competitiveness with, thus increasing the uncertainty around their application. Surgical specialties and associated national governing bodies should act preemptively to curtail the impact of this change on medical student application behavior.60–69
There are several limitations to this analysis. This analysis is limited by the observational nature and reliance on data as reported by the AAMC. Elucidation of causal relationships remains impossible given the multifaceted complexities of residency applications. Due to the mechanism of reporting of race/ethnicity by the AAMC in 8 different categories and year to year variations, we were unable to elucidate detailed trends regarding application number per applicant with this demographic factor. However, further classification of this variable by race/ethnicity is important to ensure an equitable application process for all applicants. It is possible that socioeconomic factors which are unavailable in the AAMC’s dataset may confound these trends. Still, more underrepresented in medicine groups appear to be applying to surgical specialties which is critical for addressing their representation in surgical specialties.70–74 Match statistic data from the NRMP does not stratify according to sex or race/ethnicity and a targeted match analysis focused on these applicant characteristics was unable to be performed. In addition, despite an increase in the cost of applying to surgical residencies, applicants in the virtual application cycles have likely faced less total cost associated with applications due to reduced travel cost. Residencies for integrated thoracic surgery and integrated vascular surgery are in the early stages of national adoption, thus trends from these emerging residencies programs may not provide an adequate interval of equilibrium for comparative assessment. Due to nature of this study’s data, statistical analysis was not able to be performed.
Conclusions
Across all surgical specialties, the number of applications per applicant has increased by significant margins since the 2017 residency application cycle. It is possible that the COVID-19 pandemic accelerated this process, however increased in application numbers were seen before the onset of the pandemic. These changes come at significant costs, with increased financial burden to applicants, increased work by residency program personnel, and a potential deduction in the holistic review of applications. Novel signaling efforts conducted by otolaryngology did not reduce the number of applications per applicant. Orthopedic surgery is the only specialty which did not face large scale change during this time period, and further examination of the orthopedic surgery application process may aid future application cycles.
Footnotes
Author Contributions
N. Singh: Writing, data collection, data analysis, and approval of the final version for submission. C. Boyd: C. Boyd: Writing, editing, study design, idea generation, and approval of the final version for submission
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.