
Abstract

Traumatic breast injuries can be severe and life-threatening and have a significant impact on a patient’s cosmetic appearance. Expanding breast hematomas may require operative interventions. Clinically significant breast hematomas requiring intervention occur more commonly in blunt force trauma in an older patient population. 1 Surgical interventions are not common but may be associated with severity and mechanism of trauma. Burns were shown to have a higher mortality rate and length of hospital stay compared to blunt or penetrating trauma. 2 Despite the morbidity of these injuries, the existing literature is lacking.
Louisiana has one of the highest rates of morbidity and mortality due to trauma in the nation. 3 However, breast trauma has not been well-studied in this region. The goal of this study was to characterize traumatic breast injuries in different crime risk areas within an urban community to develop prevention strategies.
Institutional Review Board approval and a waiver of consent were obtained prior to study initiation. A retrospective chart review was performed on adult female trauma patients presenting from August 2016 to August 2022 to an urban level 1 trauma center. Patients who suffered traumatic breast injuries were identified by ICD-10 codes. Zip codes of injury location were also collected.
For data analysis, patients were first stratified into two groups based on zip code of injury: high-risk group and a non–high-risk group. Division was performed by identifying the highest areas of crime mapped by NeighborhoodScout. 4 After stratification, both groups were compared. Univariate analysis was performed using the Mann-Whitney U test for continuous variables or Fisher’s exact test for categorical variables. Data was analyzed using IBM SPSS (version 27, Armonk, NY). A P-value equal to or less than .05 was considered statistically significant.
A total of 47 patients were included in the study with 18 patients (38.3%) in the high-risk zip code group. There was a higher percentage of younger patients (35 +/− 9.8 years vs 45.2 +/− 17.4 years; P = .03) in the high-risk group. There was a higher percentage of African American patients in the high-risk group compared to the non–high-risk group (n = 17/18, 94% vs n = 13/29, 45%; P = .0005). Penetrating mechanism made up a higher percentage of the high-risk zip group; however, the difference was not significantly different (P > .05). Bedside primary closure of the breast injury was more common in the high-risk group patients as well (n = 5/18, 28% vs n = 3/29, 10%, P = .04). There were no significant differences seen in insurance status, hospital admission, hospital length of stay, injury severity score, or follow-up requirements between the groups (P > .05) (Figure 1).
Breast trauma remains an understudied and underrecognized area of injury. This study showed that the most common race for this cohort of patients was African American females, and bedside procedures were used for treatment of their injuries. It was also found that traumatic breast injuries in high-crime risk communities were more often seen in younger patients. Similarly, a large nationwide study analyzing breast trauma demographics recognized that younger patients were linked to more penetrating breast injuries. 2 Patients with traumatic breast injuries may be linked to domestic violence trauma, especially penetrating breast injuries. In our study, 27% of penetrating breast injuries were documented due to domestic or partner violence. Identifying abuse in these patients is critical to offering the appropriate support and resources for victims.
The existing literature on breast trauma is lacking. Thus, there is no standard of care for the treatment and management. Most of the research on traumatic breast injuries is limited due to the failure to document and distinguish between breast trauma and chest trauma. 1 Limitations of this study include the retrospective nature, single center, and small sample size. Future prospective studies are needed to further characterize traumatic breast injuries to develop prevention strategies and appropriate management plans.
This study suggests that there are differences in demographics between traumatic breast injuries when comparing high-risk vs non–high-risk zip code group locations. These community locations can represent target areas for outreach in prevention. However, future studies are needed to better characterize this etiology. Comparison Between High-Risk vs Non–High-Risk Zip Code Groups of Traumatic Breast Injuries.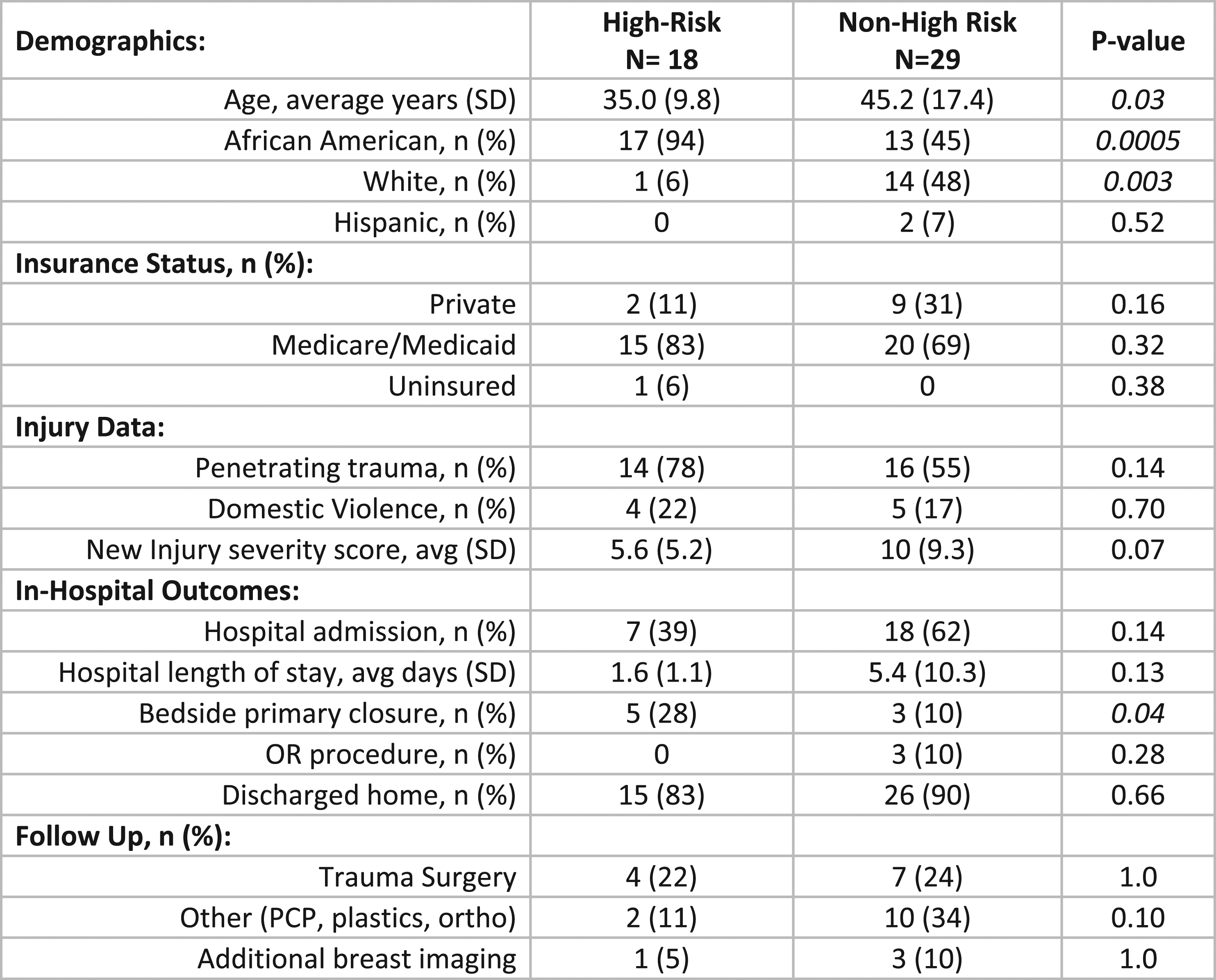
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.