
Abstract
Background
Decompression of the intestine with a long tube or nasogastric tube is the first-choice treatment for adhesive small bowel obstruction (ASBO). Scheduling surgery while weighing the risks of surgery against conservative care is a crucial factor in clinical decision-making. Whenever feasible, unnecessary surgeries should be avoided, and it is essential to provide clinical markers for this. This study aimed to obtain evidence regarding the optimal timing of ASBO and when conservative treatment options are not successful.
Methods
The data of patients diagnosed with ASBO and receiving long tube insertion for more than 7 days were reviewed. We investigated transit ileal drainage volume and recurrence. The primary outcomes were the change in the drainage volume from the long tube over time and the percentage of patients who required surgery. We evaluated some cutoff values to determine the indication for surgery based on the insertion duration and volume of long tube drainage.
Results
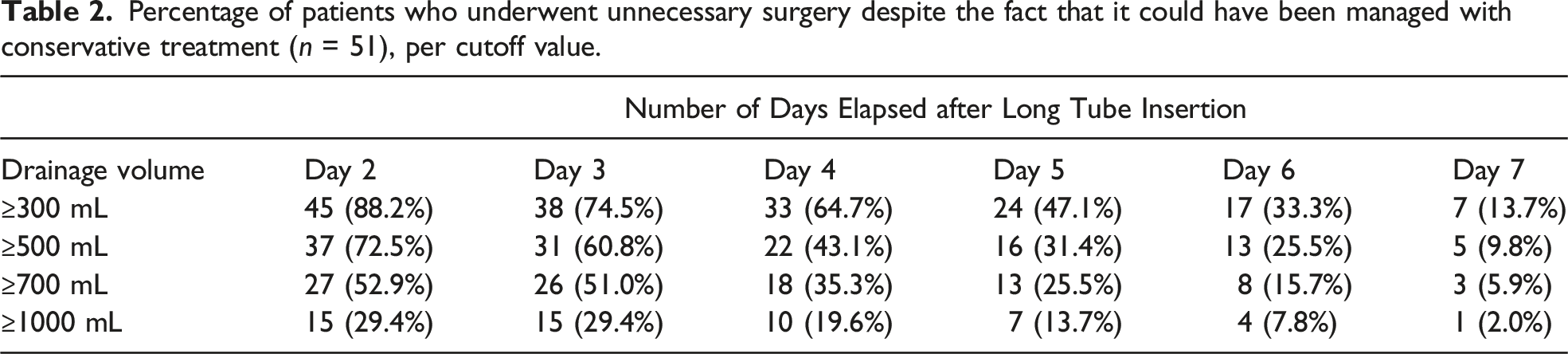
Ninety-nine patients were enrolled in this study. Fifty-one patients showed improvement with conservative treatment, whereas 48 ultimately required surgery. When a daily drainage volume of ≥500 mL was considered an indication for surgery, 13-37 cases (25%-72%) would be judged unnecessary within 6 days of long tube insertion, while 5 cases (9.8%) would be judged unnecessary on day 7.
Discussion
Unnecessary surgical interventions for ASBO might be avoided by assessing the drainage volume on day 7 after inserting a long tube.
Key Takeaways
• Our findings demonstrate the percentage of successful conservative therapy at each drainage volume cutoff point up to 7 days following long tube insertion. • Unnecessary surgical interventions for adhesive small bowel obstruction might be avoided by assessing the drainage volume on day 7 after inserting a long tube. • With these findings in mind, surgeons may be able to spare high-risk ASBO patients from needless surgical interventions.
Introduction
The first-choice treatment for adhesive small bowel obstruction (ASBO) is decompression of the intestine via the insertion of a long tube or nasogastric tube. 1 The evidence-based guidelines from the World Society of Emergency Surgery ASBO working group recommend this nonoperative treatment, which has an efficacy of 70%-90%. Some studies have proven the safety of nonoperative management within 72 h; 2 however, the evidence or consensus is absent in cases with a persistently high volume output from a decompression tube. In clinical practice, it is likely that conservative treatment is often continued for approximately 1 week for patients with stable conditions.
An important issue in clinical decision-making is determining the timing of surgery while considering the risks of surgery vs conservative treatment. In general practice, surgeons consider the relationship between the duration of long tube insertion and fluid drainage volume to determine the indication for surgery; however, no exact index value has been identified. Some studies have suggested that surgery should be considered if the drainage volume is ≥ 500 mL on the third or fourth day after long tube insertion.3,4 On the other hand, Onda et al reported that 40% of patients could avoid surgery, even on days 7-14 after long tube insertion. 5 Although prolonged non-surgical treatment with decompression may lead to dehydration, renal failure, malnutrition, and deterioration of patients’ conditions, surgical intervention with laparotomy for ASBO may cause further adhesions. It is important to avoid unnecessary surgeries whenever possible, and it is crucial to develop clinical indicators for this.
Decompression with a long tube is often used in the treatment for ASBO and is effective. However, the long-term placement of an ileus tube causes a patient physical and emotional distress. We conducted this retrospective study to investigate whether the indication for surgery could be determined earlier based on the relationship between the amount of drainage and the insertion duration in patients who had a long tube inserted for >7 days. The results of this study may serve as a useful clinical marker for surgeons in determining the indications for surgical treatment for ASBO.
Methods
Study Design and Patients
This study was conducted in accordance with the principles of the Declaration of Helsinki and all applicable local laws and regulations. The study protocol was reviewed and approved by the institutional review board of Southern Tohoku General Hospital (approval number: 553). All study participants provided informed consent.
A single-arm, retrospective, and observational design was adopted for this study. Between January 2012 and December 2020, data on consecutive patients diagnosed with ASBO and who had a long tube inserted were selected from the hospital database. Of these patients, those with the long tube in place for ≥8 days were selected for the analysis. In addition to patient demographics, a detailed medical history was obtained, including a history of abdominal operations and ASBO. We excluded patients with malignant diseases (including primary, metastatic, or recurrent disease), suspected bowel obstruction due to inflammatory bowel disease, or signs of strangulation at the moment of diagnosis based on imaging and other laboratory findings.
Treatment Strategy and Surgical Indication
A long tube (single lumen tube) was inserted in our hospital for ASBO, and intermittent suctioning was performed. The tube was removed when the drainage volume decreased to 500 mL or less. If the patient had abdominal distention symptoms or did not exhibit flatulence, we performed a clamp test or gastrointestinal series test. Moreover, we ensured there was no passage obstruction before removing the tube.
Surgery is considered if the long tube drainage volume is > 500 mL after ≥7 days of insertion. Surgery was performed either via laparotomy or laparoscopy. Although adhesiolysis is the basic technique, intestinal resection was performed at the surgeon’s discretion.
Outcome Measurement and Statistics
We examined when and how much drainage volume would indicate that a conservative treatment had failed, that is, whether surgery could be indicated early. The main outcome was the percentage of patients for whom unnecessary surgery was avoided based on each cutoff value of fluid volume drained from the long tube. Specifically, if the cutoff values for drainage volume were set at 300, 500, 700, and 1000 mL from day 2 to day 7 after insertion, we calculated the proportion of patients who could have shown improvement with conservative treatment. We defined successful conservative treatment as patients who could be discharged without surgery during hospitalization and did not require surgical treatment for ASBO during the minimum 1-year observation period after discharge.
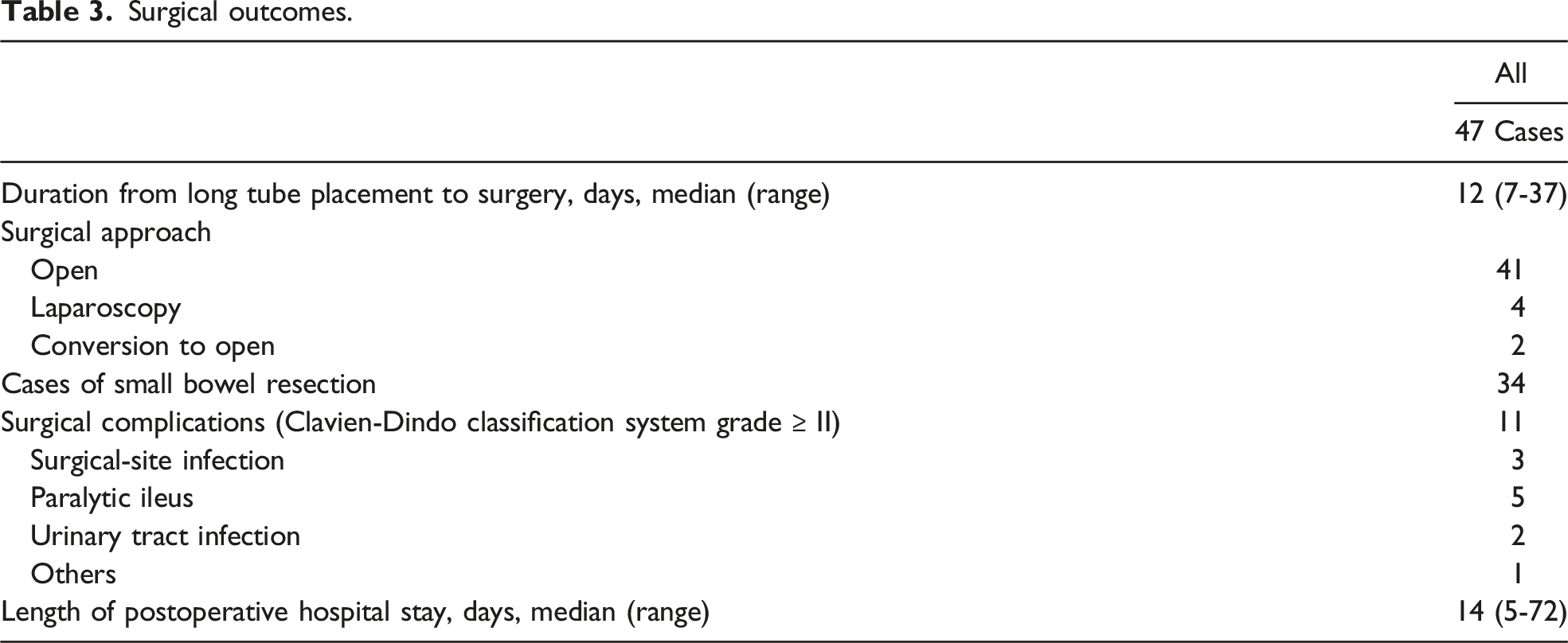
As secondary outcomes, we also evaluated the procedure, length of postoperative hospital stay, and postoperative complications in patients who underwent surgery after ≥8 days of long tube insertion.
Results
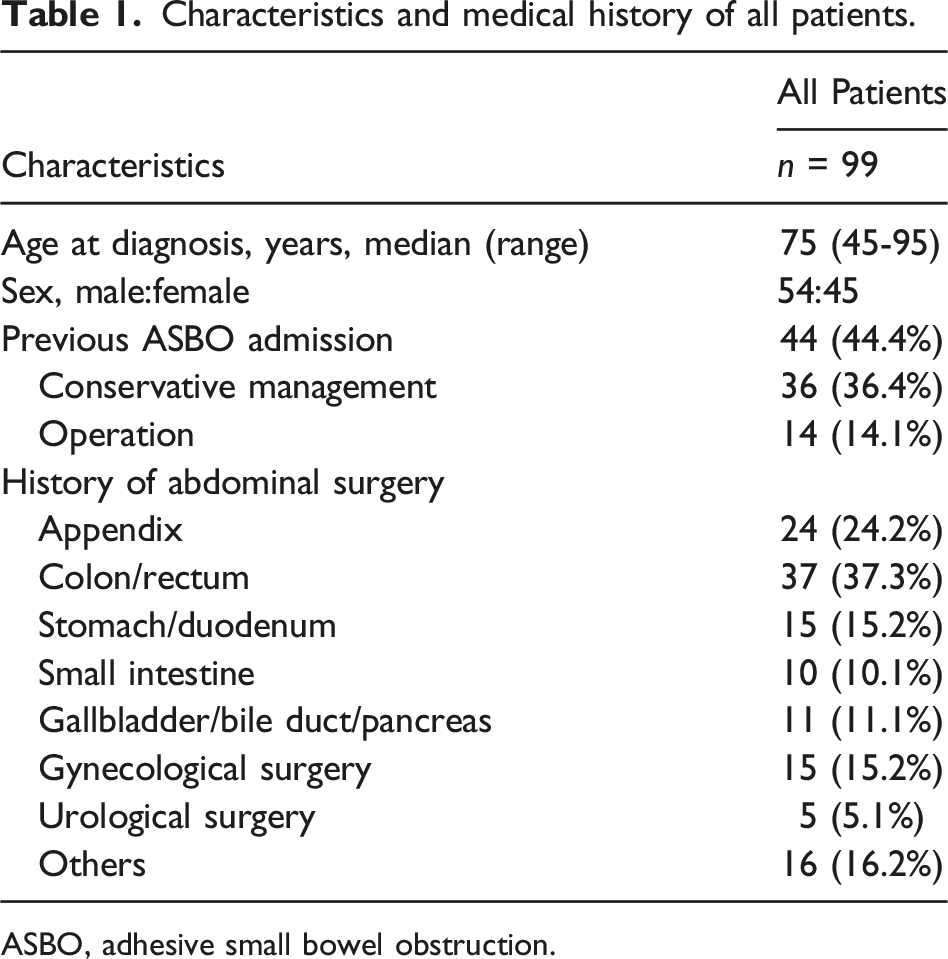
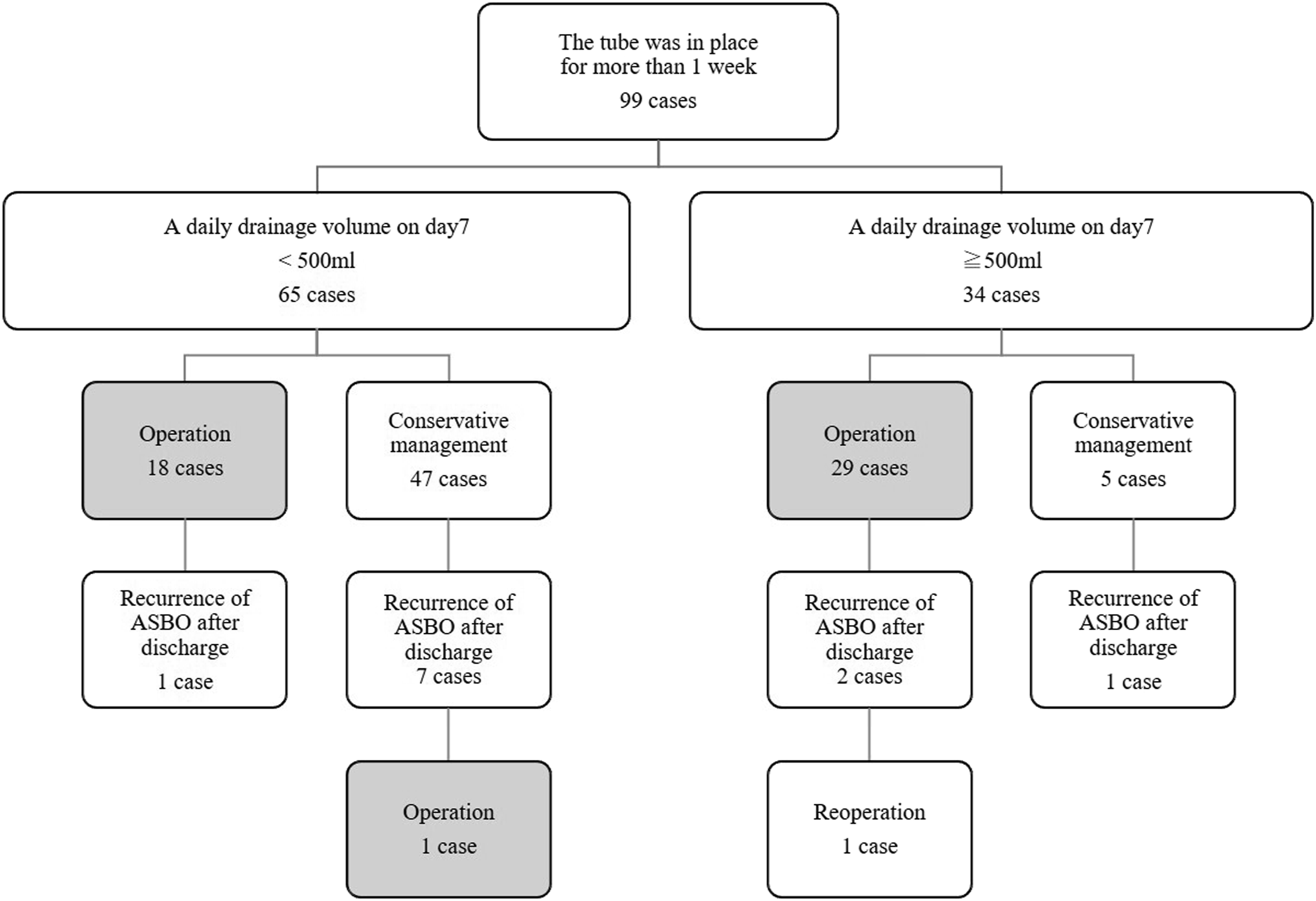
The clinical course of all patients is shown in Figure 1. A long tube was inserted in 332 patients during the study period, and in 99 patients, the tube was in place for >1 week. Patient characteristics and medical history are shown in Table 1. Previous surgeries involved surgeries for various diseases in the gastrointestinal tract, hepatobiliary and pancreatic regions, and gynecological and urological regions. Forty-four patients (44.4%) were hospitalized for ASBO, and 14 (14.1%) had previously undergone surgery for ASBO. The median observation period was 24 (12-105) months. Fifty-one (51.5%) patients showed improvement with conservative treatment, and 48 (48.5%) ultimately required surgery (Figure 2). The patients’ drainage volumes of <500 mL on day 7, for which surgery was performed, were due to repeated hospitalizations, discharges for ASBO within a year, and the patient’s strong desire for surgery. On the other hand, the reason why the patients with drainage volumes >500 mL on day 7 did not undergo surgery was their strong refusal to undergo surgery and their intolerance or general condition. The median duration from long tube insertion to surgery was 12 (7-37) days. Patient enrollment. In 99 of 332 patients, a long tube was inserted for >1 week. Characteristics and medical history of all patients. ASBO, adhesive small bowel obstruction. Clinical course of all 99 patients. Fifty-one patients showed improvement with conservative treatment, whereas 48 patients ultimately required surgery.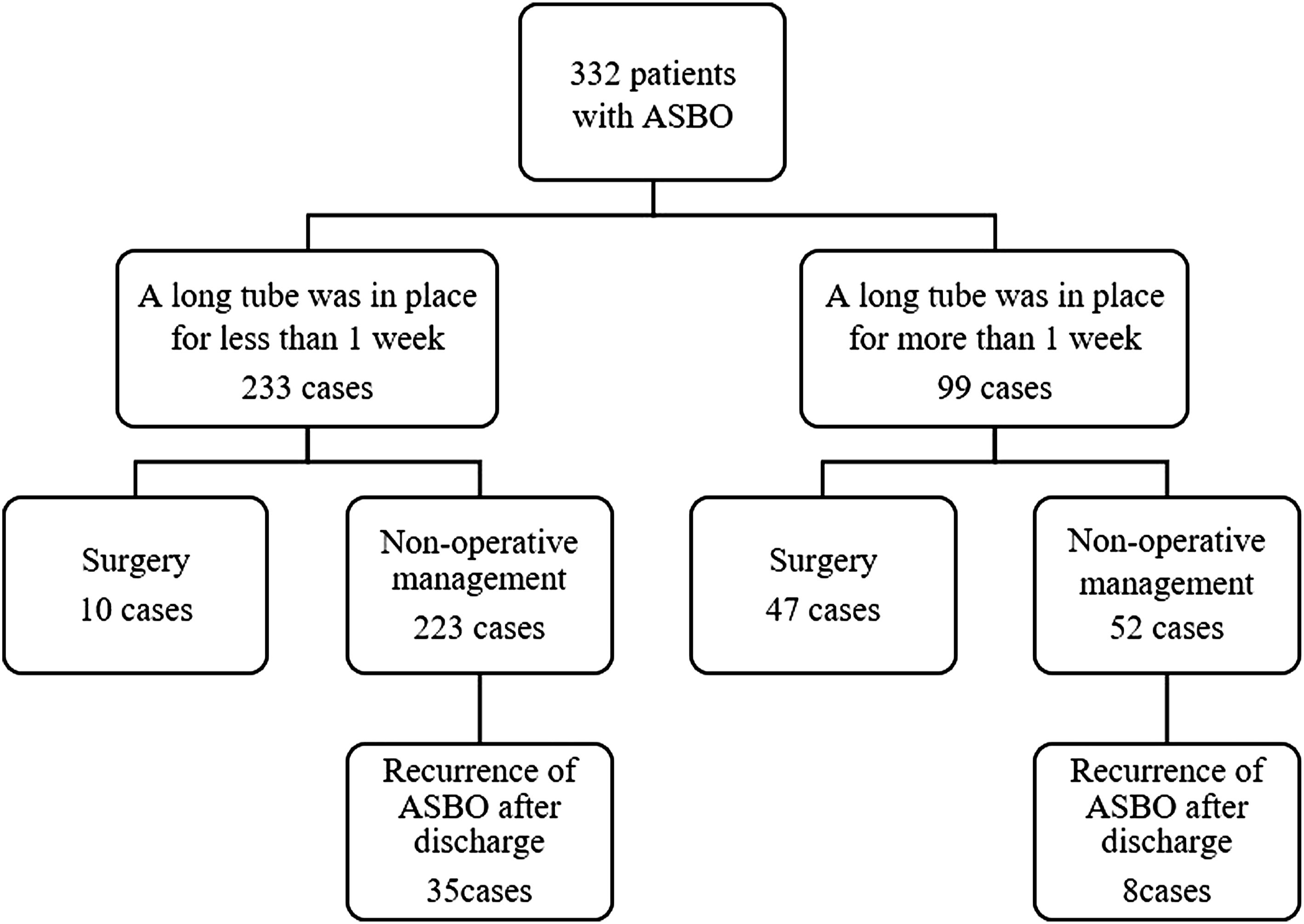
Dot plots and box-and-whisker plots show the drainage volume per day from day 3 to day 7 after long tube insertion in patients who underwent surgery (n = 48) and those who improved with conservative treatment (n = 51). In the former, the median daily drainage volume showed little change over time, while the latter showed a decrease in daily drainage volume over time (Figure 3). Dot plots and box-and-whisker plots of the drainage volume per day from day 3 to day 7 after long tube insertion in patients who underwent surgery and those who improved with conservative treatment.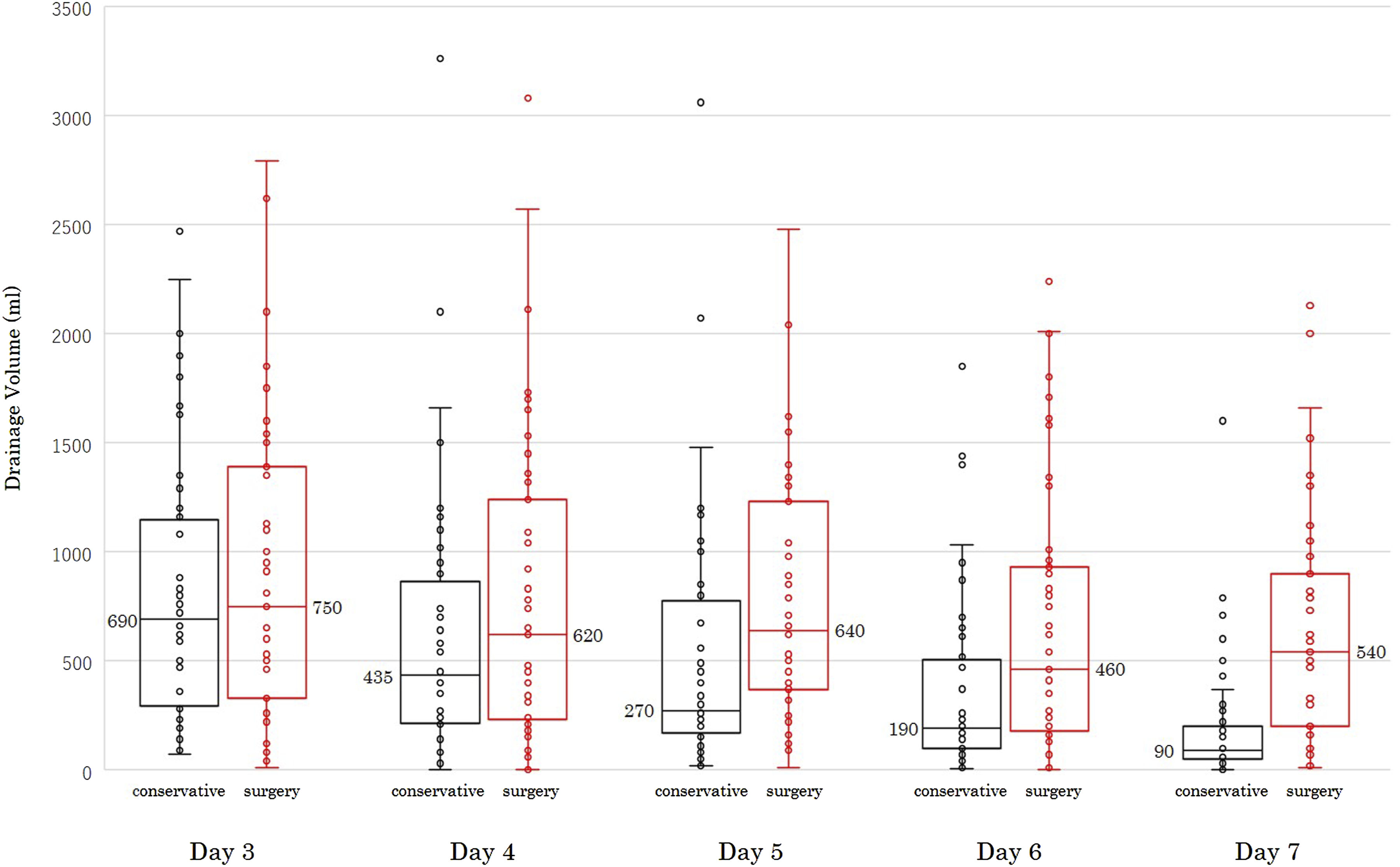
Percentage of patients who underwent unnecessary surgery despite the fact that it could have been managed with conservative treatment (n = 51), per cutoff value.
Surgical outcomes.
Discussion
Two clinically important findings emerged from this study. First, 1 potential criterion to reduce unnecessary surgery for ASBO to less than 10% would be a drainage volume of less than 500 mL on the seventh day or less than 1000 mL on the sixth day after tube insertion. Unfortunately, it was difficult to predict the probability of successful conservative treatment based on drainage volume prior to the fifth day after tube insertion. Second, grade ≥ III postoperative complications were 2.1%, even in patients with long tubes inserted for more than 7 days.
Matsumura et al 6 reported that between 1959 and 1968, 74.1% of patients diagnosed with ASBO required surgery. In 1975, the percentage of patients indicated for surgery dropped to 52.1% and decreased to 16.9% in 2000 with advances in decompression therapy and systemic management.5,7 In this study, 17.2% of patients with ASBO underwent surgery, similar to that reported in a previous study. Undoubtedly, the first choice for ASBO is decompression of the intestinal tract with a gastric tube or long tube, bowel rest, and intravenous fluid hydration, but the problem lies in the timing of the surgical decision.
Sakakibara et al and Higaki et al focused on the drainage volume of the long tube and stated that surgery was indicated when the drainage volume was ≥500 mL 3 days after implantation.3,8 Furthermore, in Europe and the United States, the Bologna Guidelines 9 issued by the World Society of Emergency Surgery in 2017 recommend 3 days. Similar to these references, recent reports have emphasized the advantages of reducing the number of days of conservative treatment and making early treatment decisions. However, most of the reports that provided evidence for the above conclusions were based on the trend of cases operated at each institution as the standard for surgical indication, and conclusions were drawn by comparing cases operated on and those treated conservatively, which is hardly an appropriate indication for surgery. In fact, the Bologna Guidelines also have an evidence level of 2b and a recommendation level of C, which is not a strong recommendation. In our result, even among the 51 cases that were ultimately successfully treated conservatively, approximately 25% (13/51) had a daily drainage volume of 500 mL or more on the sixth day after long tube insertion.
Notably, when the indication for surgery was defined as a drainage of ≥500 mL on day 7, the proportion of patients who underwent unnecessary surgery decreased. Based on these results, there is a certain validity to the indicator that surgery is indicated when a daily drainage volume is ≥ 500 mL on day 7 after the insertion of a long tube. Shih et al reported that when surgery is indicated for patients who do not improve after 5 days of conservative treatment, unnecessary surgery is performed in approximately 60% of cases; 10 therefore, evaluation on day 7 was considered an important time point to avoid unnecessary surgery. Of course, in clinical practice, inserting a long tube for a week is painful for the patient and leads to a longer hospital stay, so there is no denying that early surgery can be performed if the patient desires it.
In this study, surgery was performed at a median of 12 days after long tube insertion. Postoperative complications were comparable to those reported in previous studies, and longer waiting times did not appear to increase surgical risk. Additionally, previous reports have shown that prolonged conservative treatment does not increase complications.11,12 However, there are reports that postoperative complications increase when the waiting time exceeds 3 days.13,14 Therefore, in cases of long tube insertion, the results of this study can be used as a reference to educate patients and decide whether to perform surgical intervention at an early stage, considering the patient’s condition and wishes.
A limitation of this study was that the indication for surgery was determined based solely on drainage volume. In clinical practice, we should consider the number of previous ASBO admissions and the recurrence rate after conservative treatment when deciding the indication for surgery.
In conclusion, our results show the percentage of successful conservative treatment at each cutoff value of drainage volume up to 7 days after long tube insertion. Considering these results, surgeons may be able to avoid unnecessary surgical intervention in high-risk patients with ASBO.
Footnotes
Acknowledgments
We would like to express our gratitude to Seria Sato, Kaori Ouchi, and Eriko Yamaguchi for their help with data collection.
Authors’ Contributions
Substantial contributions to conception and design, acquisition of data: Michitaka Honda, Teppei Miyakawa, Yukitoshi Todate, and Yoshinao Takano Study conception and design: Eiichi Nakao and Michitaka Honda Acquisition of data: Michitaka Honda, Teppei Miyakawa, Yukitoshi Todate, and Yoshinao Takano Analysis and interpretation of data: Eiichi Nakao and Michitaka Honda Drafting of manuscript: Yukitoshi Todate, Eiichi Nakao, and Shinichi Konno Critical revision: Satoshi Toshiyama, Nobuyasu Suzuki, and Ryuya Yamamoto.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.