
Abstract
Background
The use of laparoscopy in the repair of duodenal atresia has been increasing. However, there is no consensus regarding which surgical approach has better outcomes. We aimed to compare the different surgical approaches and types of anastomoses for duodenal atresia repair.
Methods
Patients who underwent duodenal atresia repair at a single pediatric center were identified between January 2006 and June 2022. Those with concomitant gastrointestinal anomalies or who required other simultaneous operations were excluded. The primary outcome was rate of complications, defined as rate of leak, stricture, and re-operation by surgical approach and technique of anastomosis.
Results
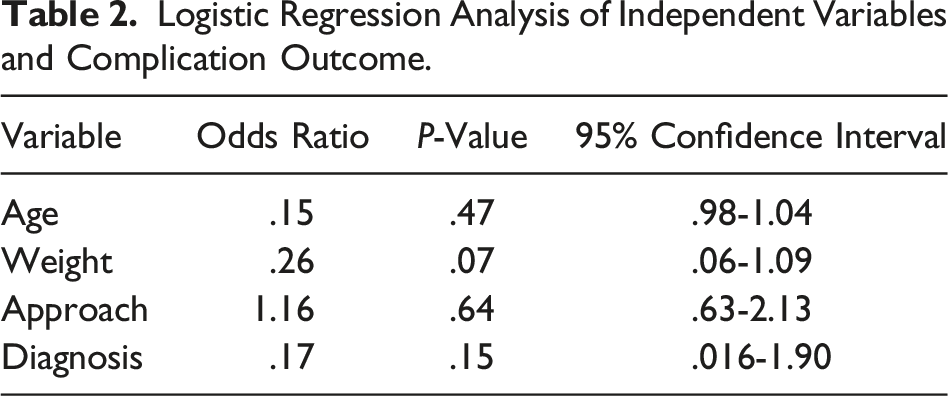
A total of 78 patients were included. The majority were female (51.3%, n = 40), with a median age of 4 days (IQR 3.0,8.0) and a median weight of 2.7 kg (IQR 2.2,3.3) at repair. The re-operation rate was 7.7% (n = 6), of which two were anastomotic leaks, and four were anastomotic strictures. The leak rate was 5.6% (n = 1/18) for the open handsewn and 4.8% (n = 1/21) for the laparoscopic handsewn technique. The stricture rate was 12.5% (n = 1/8) for the laparoscopic-assisted handsewn, 9.1% (n = 2/22) for the laparoscopic U-clip, 4.8% (n = 1/21) for the laparoscopic handsewn, and none with laparoscopic stapled and laparoscopic converted to open handsewn techniques. No differences were found in complication rate when controlling for surgical approach.
Conclusion
The method of surgical approach did not affect the outcomes or complications in the repair of duodenal atresia.
Key Takeaways
• There has been controversy regarding the benefits of laparoscopic vs open surgery for duodenal atresia. • A comparison of the different surgical approaches and anastomosis techniques in the repair of duodenal atresia resulted in similar outcomes.
Introduction
Duodenal atresia is a rare congenital anomaly characterized by a partial or complete obstruction of the duodenum occurring in approximately 1 in 5000-10,000 live births.1,2 Surgery is the mainstay of treatment to relieve the obstruction and restore intestinal continuity.
There are several surgical techniques available for repairing duodenal atresia, the most commonly used being a duodenoduodenostomy which can be performed as an open or laparoscopic procedure. 3 While the choice of surgical technique depends on the type and location of the duodenal obstruction, as well as the surgeon’s experience and preference, advances in minimally invasive surgery have allowed the transition from open to laparoscopic duodenal atresia repair. 2 Despite the introduction of laparoscopic repair in the 2000s, there is no consensus regarding the safety and efficacy of laparoscopic duodenostomy when compared to traditional open repair.2,4
There have been multiple recent studies comparing outcomes between laparoscopic and open duodenal atresia repair.1,2,4-6 These studies have shown that laparoscopic duodenostomy is feasible and safe. 1 However, there has been controversy regarding the benefits of laparoscopic vs open surgery for duodenal atresia. Some studies have demonstrated longer operative times for laparoscopic surgery,4,6 with the advantage of shorter time to initial oral feeding, shorter mean time to full oral feeding, and shorter length of hospital stay.2,4
In addition, there are multiple techniques to complete the anastomosis including handsewn, U-clip, and stapled approaches. U-clips were used before they were discontinued from the market with good results.5,7 Mini staplers (<6 mm) are now available in the market and have also been shown to be a safe and feasible technique for laparoscopic repair of duodenal atresia. 8
Most available studies have small sample sizes and offer comparisons between open and laparoscopic surgical outcomes. Studies comparing all surgical modalities including the technique of anastomosis creation are scarce. Our aim was to compare the outcome between all the different surgical and anastomotic approaches for the repair of duodenal atresia. We hypothesized that there is no difference in outcomes when considering the approach and type of anastomosis performed.
Materials and Methods
Institutional Review Board approval was obtained for this study. Patients who underwent duodenal atresia repair at a single pediatric center were identified between January 2006 and June 2022. Those with concomitant gastrointestinal anomalies, those who required other simultaneous operations at the time of duodenal atresia repair, and those who underwent surgery at an outside hospital or had incomplete medical records were excluded. The surgical approach and anastomosis type were chosen by the attending board-certified pediatric surgeon performing the case based on their preference and experience. We categorized surgery type as laparoscopic, open, laparoscopic converted to open, and laparoscopic assisted. In the laparoscopic-assisted technique, the surgeon exteriorized the duodenum to perform the anastomosis in an extracorporeal fashion with all other aspects of the surgery performed laparoscopically. In the laparoscopic converted to open case, the surgeon extended the laparoscopic incision and performed the case in an open fashion.
Our electronic medical record transitioned to new software in 2007 and therefore some records before that date were incomplete. A retrospective chart review was performed to obtain data such as demographics, surgical details, hospital admissions, time of feedings, imaging results, and postoperative complications. The primary outcome was rate of complications, defined as the rate of anastomotic leak, stricture, and re-operation by surgical approach and technique of anastomosis. Secondary outcomes included operative duration and time to first and full feedings.
Anastomotic leak was defined as evidence of contrast extravasation on an upper gastrointestinal study performed postoperatively. Stricture was defined as a narrowing of the anastomosis that was causing signs of obstruction such as abdominal distention, nausea, and vomiting. Operative duration was measured from skin incision time to end of surgery. The first feeding time was defined as the first time the patient was provided enteral nutrition either by nasogastric/orogastric tube or orally. Full feeding time was defined as the first time the goal feeding rate or quantity was provided, as established by the primary team or nutrition services. Data are presented as medians with interquartile ranges, and frequencies with percentages, where applicable. Logistic regression was used to analyze the relationship between weight, surgical approach, diagnosis, and complication probability. Linear regression was performed to evaluate if the surgical approach and anastomosis type influenced operative duration, time to first feeding, and time to full feeding. Significance was defined as a P < .05. Stata (StataCorp 2017. Stata Statistical Software: Release 15. College Station, Tx: StataCorp LLC) was used for all statistical analyses.
Results
Cohort Baseline Characteristics.
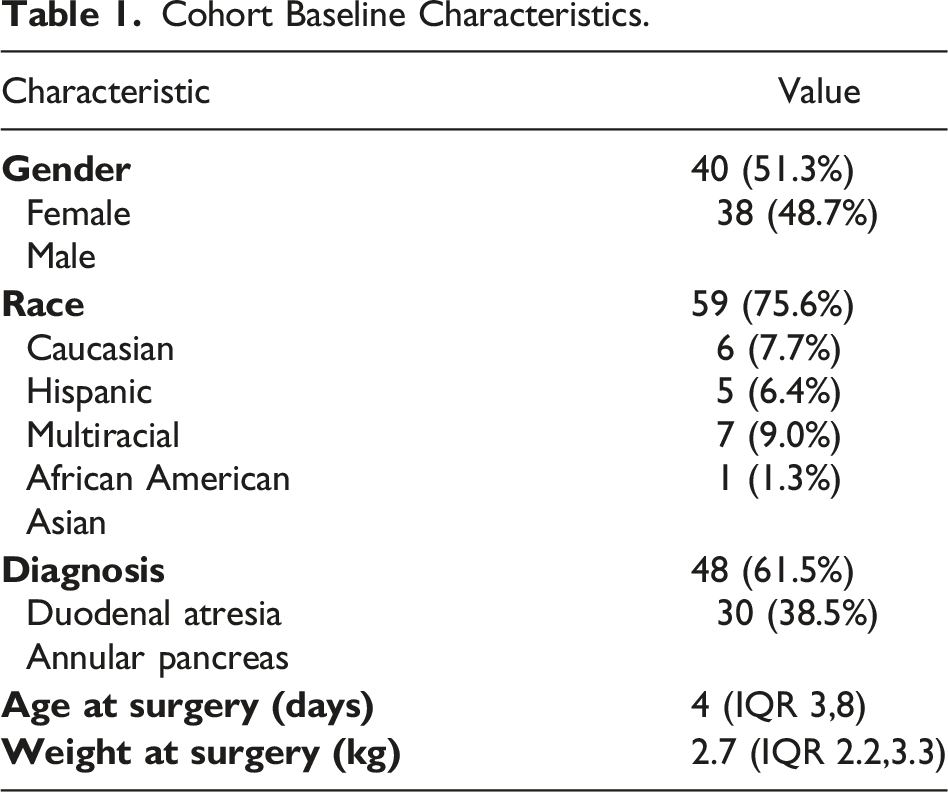
The predominant surgical approach was laparoscopic (L) (64.1%, n = 50), followed by open (O) (23.1%, n = 18), laparoscopic assisted (LA) (10.3%, n = 8), and laparoscopic converted to open (LCO) (2.6%, n = 2). Most anastomoses were handsewn (HS) (62.8%, n = 49), followed by U-clip (UC) (28.2%, n = 22) and stapled (S) (9.0%, n = 7).
Logistic Regression Analysis of Independent Variables and Complication Outcome.
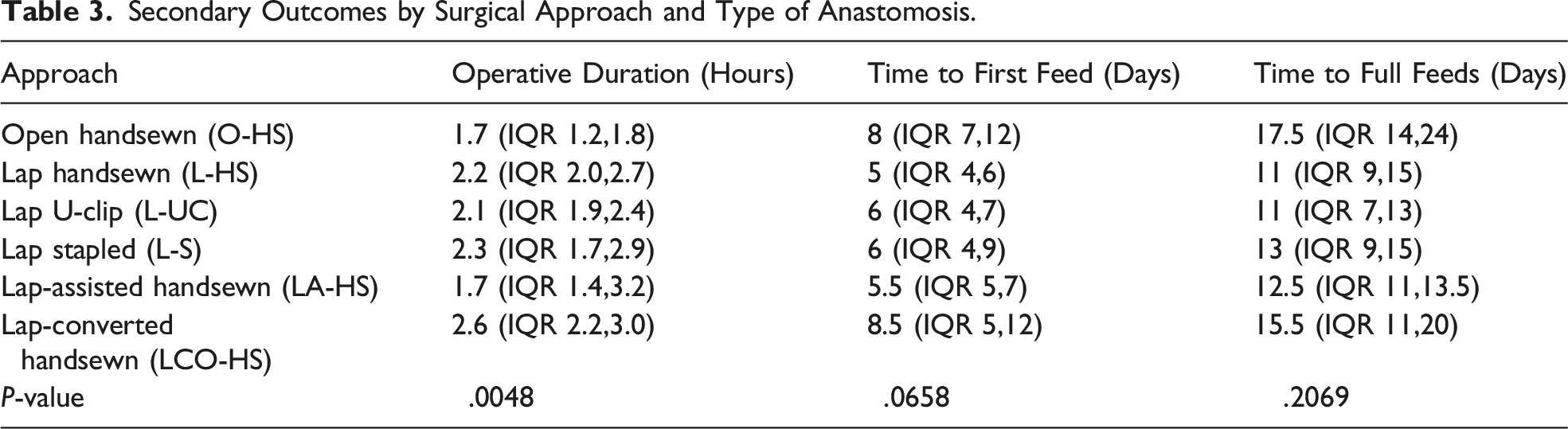
Secondary Outcomes by Surgical Approach and Type of Anastomosis.
Discussion
A comparison of the different surgical approaches and anastomosis techniques in the repair of duodenal atresia resulted in similar outcomes. Open and laparoscopic-assisted handsewn anastomoses result in a significantly shorter operative duration.
In our institution, laparoscopic duodenal atresia repair was the predominant surgical approach and handsewn was the most commonly used anastomosis type. Laparoscopic duodenal atresia repair was introduced in the 2000s with the first reports showing high rates of leak with handsewn anastomosis. A 2011 single-center retrospective review reported 22 cases of laparoscopic duodenal repair from 2000 to 2005 of which 22.7% had a postoperative anastomotic leak. 9 However, there were no reported incidents of anastomotic leaks in patients undergoing laparoscopic duodenal repair from 2008 to 2010. 9 As surgeon experience and technical abilities with laparoscopic duodenal repair improved, the rate of complications decreased and outcomes with open surgery were comparable to laparoscopy.1,2,4-6 This is reflected in our institution as the predominant surgical technique after 2005 was laparoscopy.
After high rates of leak were reported with the laparoscopic handsewn technique, our institution started using U-clips to create the anastomosis with favorable results. Results of our experience with this technique have been previously published and account for this technique being the second most common in our cohort. 7 We recognized no anastomotic leaks and only had one case of stricture requiring re-operation with this type of anastomosis.
Previous reports have demonstrated a shorter time to initial and full feedings with the laparoscopic technique.4,10 However, when comparing each surgical approach paired with the anastomosis type we did not find any differences. First feeding time ranged from 5 to 8 days after surgery in our cohort. In our institution, patients undergo a postoperative upper gastrointestinal study around the fifth postoperative day before introducing feeds. This postoperative imaging protocol may explain the absence of a difference in time to first feed because most patients, regardless of surgical approach, had approximately five days of nothing per os before imaging. Additionally, there were other factors influencing the time of feedings in patients with cardiac issues that required cardiothoracic surgery or other procedures. Time to full feedings was also influenced by these factors, regardless of the surgical approach.
There were no relationships identified between surgical approach and rate of complications. In our cohort, anastomotic leak was observed with handsewn anastomoses in open and laparoscopic approaches. The working space in a neonate is small, and perhaps the posterior aspect of the anastomosis is the most challenging aspect of this surgery, especially for the handsewn technique. Strictures were observed with laparoscopic U-clip and laparoscopic and laparoscopic-assisted handsewn. Laparoscopic-assisted surgeries might be the result of a difficult case that required additional extracorporeal exposure to complete the anastomosis, along with potential complications. Open and laparoscopic-assisted handsewn approaches had the shortest operative duration in our cohort. Previous studies have reported mixed results with some showing longer operative times with laparoscopy than those of open duodenal repair. 5 Holler et al 8 reported shorter operative times with the laparoscopic-stapled technique than the laparoscopic handsewn approach. We did not observe this difference in our cohort. It’s reasonable that a laparoscopic-assisted approach would have similar surgery time to an open technique since it allows to complete the anastomosis faster in an assisted manner without the space constraints or the limited visibility of a purely laparoscopic technique.
Limitations of this study include its retrospective nature, small sample size, and that it is a single-institution review which impacts the generalizability of the results. The time to first feeding and full feedings could be influenced by other factors that are not related to the surgical approach or postoperative complications, such as our pre-feeding imaging protocol as previously discussed. Additionally, not all surgeries were performed by the same pediatric surgeon and this can add variability to the results as each surgeon has different surgical skills and years of experience. Despite these limitations, this study highlights the safety and feasibility of laparoscopic duodenal atresia repair. As surgeons have become more experienced with this technique and with the availability of additional devices to create intracorporeal anastomoses, outcomes of this procedure have improved over time and will likely continue to progress satisfactorily.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.