
Abstract
Introduction
Non-iatrogenic aerodigestive injuries are infrequent but potentially fatal. We hypothesize that advances in management and adoption of innovative therapies resulted in improved survival.
Methods
Trauma registry review at a university Level 1 center from 2000 to 2020 that identified adults with aerodigestive injuries requiring operative or endoluminal intervention. Demographics, injuries, operations, and outcomes were abstracted. Univariate analysis was performed, P < .05 was statistically significant.
Results
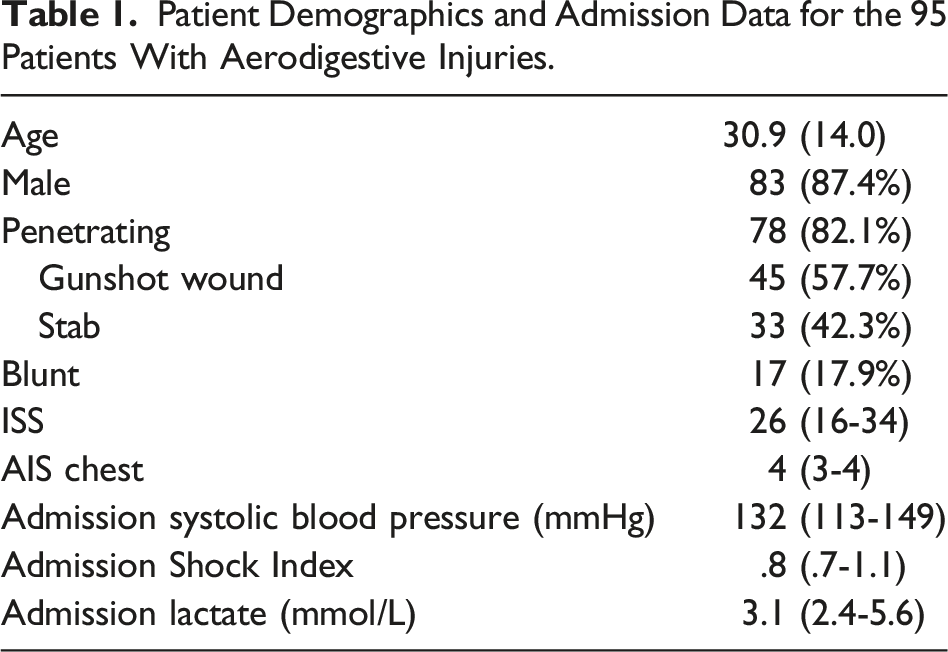
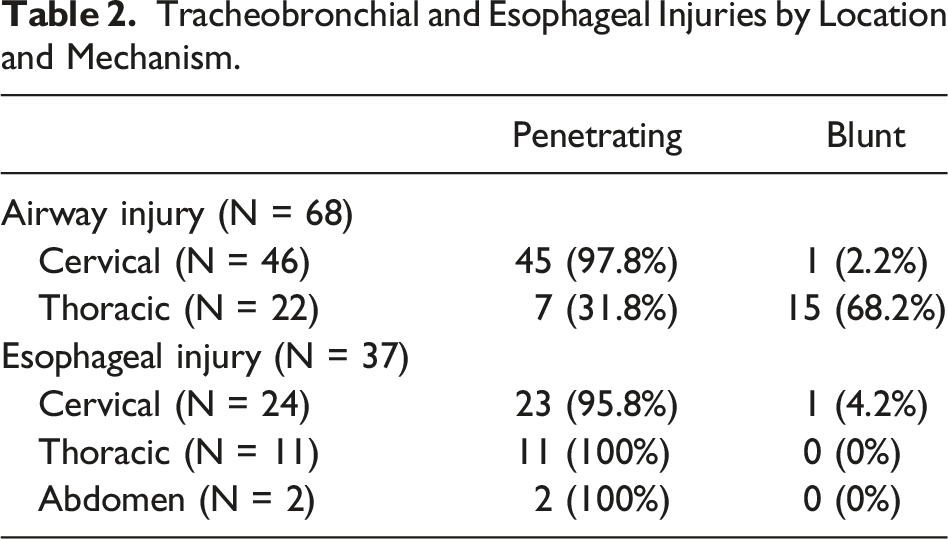
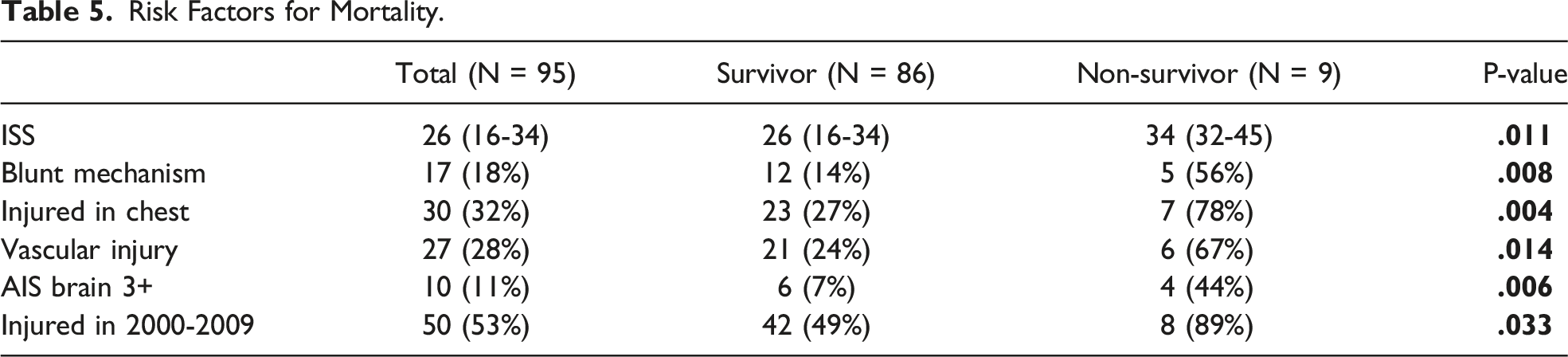
95 patients had 105 injuries: 68 tracheal and 37 esophageal (including 10 combined). Mean age 30.9 (± 14), 87.4% male, 82.1% penetrating, and 28.4% with vascular injuries. Median ISS, chest AIS, admission BP, Shock Index, and lactate were 26 (16-34), 4 (3-4), 132 (113-149) mmHg, .8 (.7-1.1), and 3.1 (2.4-5.6) mmol/L, respectively. There were 46 cervical and 22 thoracic airway injuries; 5 patients in extremis required preoperative ECMO. 66 airway injuries were surgically repaired and 2 definitively managed with endobronchial stents. There were 24 cervical, 11 thoracic, 2 abdominal esophageal injuries—all repaired surgically. Combined tracheoesophageal injuries were individually managed and buttressed. 4 airway complications were successfully managed, and 11 esophageal complications managed conservatively, stented, or resected. Mortality was 9.6%, half from intraoperative hemorrhage. Specific mortality: tracheobronchial 8.8%, esophageal 10.8%, and combined 20%. Mortality was significantly associated with higher ISS (P = .01), vascular injury (P = .007), blunt mechanism (P = .01), bronchial injury (P = .01), and years 2000-2010 (P = .03), but not combined tracheobronchial injury.
Conclusion
Mortality is associated with several variables, including vascular trauma and years 2000-2010. The use of ECMO and endoluminal stents in highly selected patients and institutional experience may account for 97.8% survival over the past decade.
Key Takeaways
• Tracheobronchial and esophageal injuries are infrequent, often have associated vascular trauma, and are potentially fatal. • 30% of patients were emergently explored for shock, an obvious vascular injury or serious airway disruption. Only hemodynamically stable patients had a CTA. ECMO and endoluminal stents were used selectively. • Mortality was significantly associated with higher ISS, blunt mechanism, thoracic location, vascular injury, and years 2000-2010 but not combined airway and esophageal injury.
Introduction
Tracheobronchial and esophageal injuries are infrequent, often have associated injuries, and are potentially fatal. Mechanism and injury location influences the presentation, diagnosis, operative approach and outcome.
The precise incidence of non-iatrogenic traumatic tracheobronchial injury is unknown since many patients die prior to hospital arrival.1,2 The cervical trachea is vulnerable to blunt and penetrating mechanisms, but penetrating injuries predominate.3-5 The majority of thoracic airway injuries occur within 2.5 cm of the carina and are overwhelmingly from blunt injury.2,4 Mortality ranges from 4.5% to 20% and is higher with blunt trauma, thoracic location, and associated injuries.3,6-8
Esophageal injuries are rare, almost entirely the result of penetrating trauma, and have serious complications and a high mortality.9-12 Mortality and morbidity are associated with a thoracic location, combined injures and, in some studies, delay to definitive repair.9,11-14 Previous studies demonstrated a higher mortality with combined tracheoesophageal injuries than isolated injuries.15-17
This is a review of the management and outcome of aerodigestive injuries requiring operative or endoluminal intervention over two decades at a high-volume urban trauma center. The hypothesis was that advances in trauma care including novel modalities, such as extracorporeal membrane oxygenation (ECMO) and endoluminal stenting, have contributed to decreased mortality over time.
Methods
This study was approved by the Institutional Review Board of the University of Maryland School of Medicine. The R Adams Cowley Shock Trauma Center registry was queried from 2000 to 2020 for patients 16 years of age or older with non-iatrogenic traumatic injuries of the trachea, bronchus, or esophagus requiring operative repair or an endoluminal procedure. Demographics, Injury Severity Score (ISS), Abbreviated Injury Scale (AIS), and admission physiologic and laboratory data were collected. Data regarding mechanism and location of injury, presentation, preoperative evaluation, operative details, complications, and mortality were abstracted. Airway injuries were classified as cervical or thoracic, and esophageal as cervical, thoracic or abdominal.
Descriptive statistics were utilized. Continuous parametric data were analyzed using paired t-tests, and nonparametric continuous data were analyzed using the Wilcoxon rank-sum test. Chi-squared or Fisher exact tests were used as indicated for the analysis of categorical data. All tests were two-tailed, and a P-value <.05 was considered statistically significant. Data are reported as mean with standard deviation (SD) or median with interquartile range [IQR].
Results
Patient Demographics and Admission Data for the 95 Patients With Aerodigestive Injuries.
Tracheobronchial and Esophageal Injuries by Location and Mechanism.
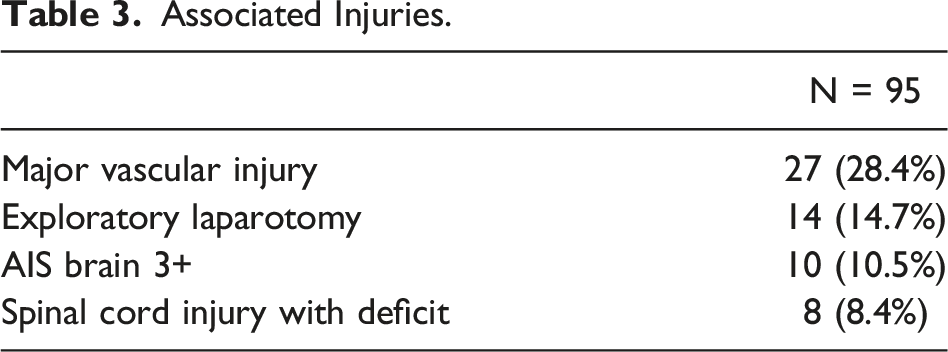
Associated Injuries.
Presentation and Evaluation
There were 29 (30.5%) patients emergently explored for shock, an obvious airway injury, or hard signs of a vascular injury. Overall, 92.6% had preoperative chest radiography. Additional preoperative studies were only performed in the 66 hemodynamically stable patients including computed tomography angiography (CTA) in 69.5%, bronchoscopy in 51.6%, surgeon-performed upper gastrointestinal endoscopy in 30.5%, and esophagram in three (3.2%). Of the 37 esophageal injuries, 73% were identified preoperatively and the remainder diagnosed intra-operatively with no missed esophageal injuries.
In the 68 patients with airway injuries, 54.4% were evident or suspected on admission including 54.1% with air escaping from the wound, 43.2% with massive subcutaneous emphysema, and 24.3% with a large continuous air leak. A definitive airway was established in 52 (76%) patients either prior to or on arrival, including 5 surgical airways. A bronchoscopy was performed by the surgeon in all suspected airway injuries. One small cervical injury was missed at the index operation and repaired within 12 hours. There were no missed injuries to the thoracic airway.
Operative Management
Operative repair was performed in 93 (97.9%) patients, and two bronchial injuries were stented. The operative approach for the cervical airway was a left neck or collar incision, with 3 extended to a partial sternotomy. Over 75% of thoracic airway injuries were managed through a right posterolateral thoracotomy on single lung ventilation. The remainder had a median sternotomy to facilitate repair of a concomitant vascular injury. Devitalized tissue was debrided, and a primary repair performed with a single layer of interrupted absorbable monofilament sutures. Ten (14.7%) tracheostomies were performed at the index operation.
Five (7.4%) patients with airway injuries were profoundly acidotic, hypercapnic, and hypoxemic refractory to conventional ventilator management. Percutaneous cannulation for veno-venous extracorporeal membrane oxygenation (VV ECMO) was performed on arrival, and the injury was repaired on ECMO.
Endobronchial stents were placed in two patients with bronchus intermedius injuries and concomitant TBI requiring intracranial pressure monitoring. The risk of hypotension, hypoxia, hypercarbia, and intracranial hypertension during operative repair made stenting a prudent option. Although initially placed as a temporary procedure, both patients had protracted courses. After interval bronchoscopies demonstrated healing, the stents were removed at 22 and 78 days, thus obviating surgery.
Of the 37 patients with esophageal injuries, a cervical incision was used in 24, a right thoracotomy in 11, and laparotomy in 2. A two-layer closure was performed over a nasogastric tube or esophageal dilator, with a running absorbable suture for the mucosa and interrupted non-absorbable sutures for the muscular layer. All repairs were widely drained, and distal feeding access was established.
Combined tracheoesophageal injuries were managed with separate repairs, and muscle was interposed between the suture lines. Also, a buttress was frequently used for isolated thoracic esophageal repairs. Sternocleidomastoid and intercostal muscle were the overwhelming choice with mediastinal pleura and fundoplication used infrequently. Vascular injuries were managed by ligation, primary repair, or interposition graft as indicated. Vascular suture lines were also buttressed.
Post-Operative Management
The use of a post-operative esophageal contrast study varied by provider and injury location. For isolated cervical repairs, oral intake was started between the third and fifth post-operative days without a contrast study with drain removal if the output did not increase. Twenty-seven (73%) esophageal repairs, including all thoracic repairs, had a contrast study on post-operative day 12 (±12.3). Oral intake was started if there was no leak. Controlled leaks were managed by continuing both NPO and enteral feedings via distal access. Drains were removed when a subsequent contrast study demonstrated resolution.
Weaning from ECMO followed guidelines for a lung protective ventilation strategy and decreasing the ECMO sweep while maintaining normal pCO2, pH, and oxygen saturation. The median duration on ECMO was 5 days (range 3-7).
Outcomes
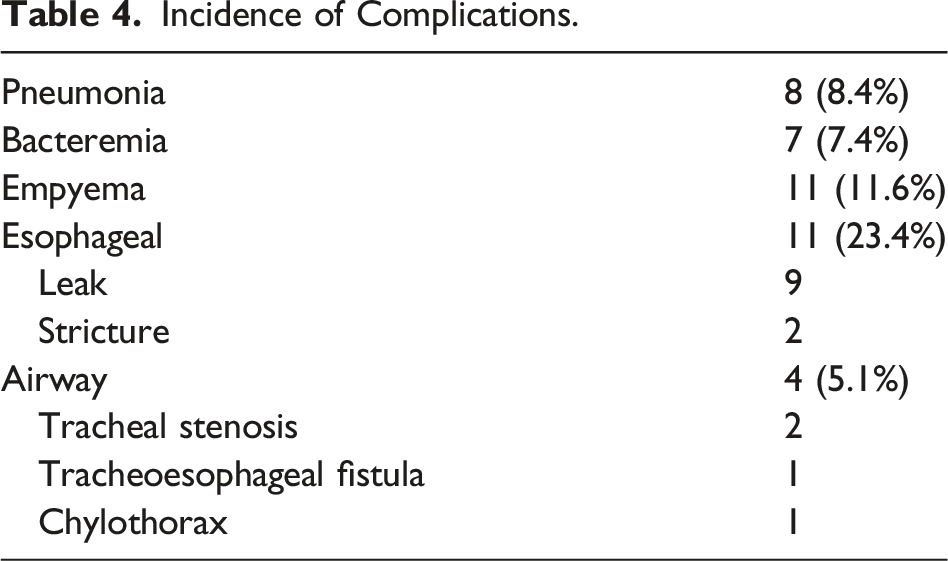
Incidence of Complications.
Hospital and intensive care lengths of stay were 19 (±22) and 12.5 (±17.2) days, respectively. Seventy (81.4%) patients were discharged home and the remainder to a short-term facility. Sixty-seven patients were followed for 11.2 (±18.3) months; the one late complication was the tracheal stenosis requiring resection.
There were nine deaths (9.5%) including five from intraoperative hemorrhage. There were four late deaths, three from multisystem organ failure, and one stroke in a TBI patient. Injury-specific mortality was 8.8% in tracheobronchial, 10.8% in esophageal, and 20% in combined injuries. Survival to discharge for ECMO patients was 80%. When comparing the decades, there were no significant differences in ISS, AIS, SI, mechanism, associated vascular injury, lactate, or blood pressure. Additionally, there were no differences in severe traumatic brain injury, thoracic injury location, or bronchial injuries. However, more ECMO and stents were used in the second decade. Mortality was significantly lower in the second decade compared to the first, 2.2% vs 16% (P = .03).
Risk Factors for Mortality.
Discussion
Of interest, 29 (30.5%) patients in this series were emergently explored for shock, an obvious vascular injury or serious airway disruption, and over 25% of esophageal injures were diagnosed at that time. This illustrates the severity of aerodigestive injuries and the importance of recognizing associated injuries. Furthermore, it reinforces that additional imaging is only appropriate in patients without hemodynamic or pulmonary decompensation. Associated vascular injuries are common and adversely impact mortality.3,4,6,8 Dyspnea, change in phonation, or subcutaneous emphysema suggest a cervical airway injury. Air escaping from the wound is diagnostic. A pneumomediastinum, large continuous air leak, or a persistent pneumothorax despite a chest tube may indicate a thoracic airway injury. A multi-slice helical CTA is an excellent screening test for airway and vascular injuries.18,19 A tracheal wall defect confirms the diagnosis. Bronchoscopy is essential to define the precise location of the injury since it determines the operative approach.
Initial airway management is of paramount importance. Direct or video-assisted laryngoscopy, bronchoscopy, or placement of the endotracheal tube through the cervical tracheal injury are all acceptable techniques. Whichever method is chosen, it is imperative to avoid converting a partial to a complete tracheal disruption. Airway management for intrathoracic injuries is more nuanced. Lung isolation enhances surgical exposure and can be achieved with selective mainstem intubation, a bronchial blocker, or a double lumen endotracheal tube, which is our preference.
Like other reports, we found cervical injuries accounted for over two-thirds of airway injuries, with 90% from a penetrating mechanism.3,4,6,7,20 A collar incision, with extension along the anterior border of the sternocleidomastoid muscle as needed, is ideal to explore the cervical trachea. Thoracic inlet injuries can be problematic since a collar incision may be inadequate and the injury is too proximal to approach by a thoracotomy. Although rarely necessary, extending the collar incision as a partial sternotomy provides excellent exposure. Comparable to other studies, a juxta-carinal thoracic location accounted for most airway injuries in our series.2-4,6,8,20
This review had a high percentage of penetrating injuries to the thoracic airway, which may reflect the population seen at a busy urban trauma center. Intrathoracic injuries were repaired through a right posterolateral thoracotomy utilizing single lung ventilation. Tracheostomy at the initial operation is a topic of debate, with some studies favoring it.20,21 However, we agree with others who recommend early extubation and, if possible, avoiding tracheostomy at the index operation.3,6,7
Endobronchial stents are commonly used for benign and malignant conditions but rarely in trauma, and only as a temporizing technique. 22 Although stents were initially placed in two patients as a bridge to surgery, the protracted clinical courses prevented timely operative repair. Since the airway healed without complication or need for surgery, endobronchial stents may be considered as definitive treatment in highly selected trauma patients.
The 8.8% mortality for tracheal injuries is similar to the 6% reported by Rossbach and colleagues 4 and 9% by Kiser and associates 6 and lower than the 13% to 23% described in other reports.3,6,8,20,21 Similar to these reports, mortality in this current review was significantly higher with a thoracic location and a blunt mechanism.
We utilized VV ECMO, without systemic anticoagulation, as a damage control strategy in patients with airway injuries and profound respiratory failure refractory to conventional ventilation. Correcting hypercarbia, hypoxemia, and acidosis allows for a safe, controlled operative repair on ECMO. Survival to discharge was 80%, consistent with our prior experience with ECMO in trauma patients. 23
Non-iatrogenic esophageal injuries are rare, almost exclusively from penetrating trauma, and more common in the neck.9-12 Similar to other reports, over 25% of esophageal injuries in this study were diagnosed during emergency exploration for an airway or vascular injury.9,11,14 We utilized CTA as the primary screening study for patients not explored emergently.11,18 An intact esophageal wall and the absence of mediastinal air or fluid effectively excludes an esophageal injury. Esophagoscopy is performed if findings suggest an injury.
The esophagus was repaired in two layers over a nasogastric tube or esophageal dilator to mitigate the risk of post-operative stricture. An esophageal myotomy is occasionally required to expose the extent of the mucosal injury, and failure to do so may increase the risk of leak. Although there is general agreement to interpose a muscle buttress between aerodigestive suture lines, there is no consensus for isolated esophageal repair.9,12,18 Because of the consequences of mediastinitis, thoracic esophageal repairs are reinforced with intercostal muscle or mediastinal pleura. Fundoplication for the distal esophagus.
Similar to other studies, associated cervicothoracic injuries were common including 28.4% with a major vascular injury. Additionally, 27% of patients with esophageal trauma had a concomitant airway injury. The 29.7% complication rate for esophageal injuries in this review compares favorability with the 29% to 53.5% in the literature.10-12,14 Similar to other studies, esophageal leak was the most common complication. Despite this, 75% resolved with non-operative management. While esophageal stents are infrequently used in the management of traumatic esophageal injuries, the two persistent leaks in this series were successfully managed with stents, which were removed prior to discharge. 24
The mortality for esophageal trauma ranges from 0 to 23%.9,10,14 In the large multicenter study by Asensio et al, the mortality was 19%. 11 Mortality is higher with a delay to definite repair, need for resection, extent of esophageal injury, thoracic location, gunshot wounds, and associated injuries.9-12 The mortality of 10.8% in this review is consistent with others.10,14 Since over 25% of patients with esophageal injuries were transferred to our facility, the time from injury to surgical repair could not be precisely determined. Consistent with other series, we found that associated injuries were common and adversely impacted mortality.9-11,14
The study limitations are those inherent to any retrospective report over two decades, as is our inability to accurately determine the impact of time to esophageal repair, which is an important variable. This report provides a comprehensive review of a large contemporary series of aerodigestive injuries managed at a mature trauma center, utilizing innovative therapeutic modalities in selected patients.
Non-iatrogenic aerodigestive injuries are infrequent even at a busy urban trauma center. Securing the airway and precisely locating the site of the injury are of paramount importance. Associated injuries, especially major vascular, are common. Almost one-third of patients are emergently explored, and only stable patients have additional imaging. Early complications, while frequent, are generally managed non-operatively, and late complications are rare. Mortality was significantly associated with higher ISS, blunt mechanism, thoracic location, vascular injury, and years 2000-2010 but not combined airway and esophageal injury. Institutional experience, precise operative repair, and selected use of innovative therapies, such as ECMO and endoluminal stents, may account for the improved survival over the past decade.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.