
Abstract
Introduction
Ground level falls in the elderly often lead to complications due to use of anticoagulants (ACs). Intracranial hemorrhage (ICH), immediate or delayed, is a feared consequence of such falls. The rate of delayed ICH (dICH) in patients taking anticoagulants or antiplatelet (AP) agents ranges from .6% to 6%. Patients on warfarin have a persistent rate of dICH, leading to implementation of routine repeat head CTs at our institution. This policy was extended to direct oral anticoagulants (DOACs). This study aims to determine institutional incidence of DOAC-associated dICH.
Methods
With IRB waiver approval, we conducted a retrospective review of trauma evaluations for falls on DOACs from 2016 to 2018. We reviewed records for neurologic status, DOAC use, and results of initial and delayed head CTs. Exclusion criteria included initial GCS ≤14, new neurologic deficits, traumatic findings on initial CT, concurrent use of additional AC/AP, or absence of repeat head CT.
Results
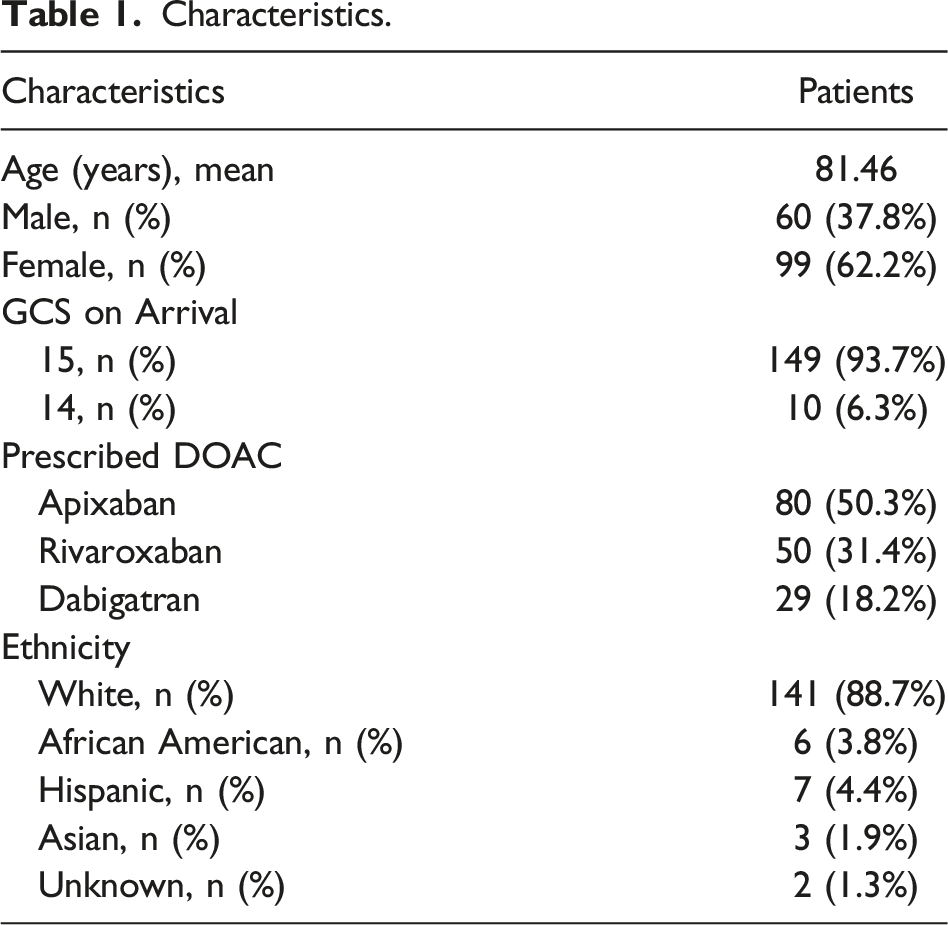
Among 632 patients evaluated for falls on AC/AP therapy, 159 (25%) of patients were included in the review. The age range was 19-98 years old, with 99 females and 60 males. Half of the patients were on apixaban, with the rest on dabigatran or rivaroxaban. Ten patients presented with GCS of 14. No delayed hemorrhages were detected in this population.
Conclusion
The necessity of a repeat head CT in patients taking DOACs is debated in the literature. Our analysis failed to demonstrate any delayed hemorrhage in neurologically intact patients after head strike on DOAC, suggesting no indication for follow-up imaging in this group.
Background
Older adults represent an increasing proportion of trauma patients. Falls are a significant source of morbidity for elderly patients, affecting 1/3 of people over the age of 65 every year. 1 Of special interest are elderly patients who sustain blunt head trauma while on oral anticoagulation. Patients taking anticoagulants or antiplatelet medications are twice as likely to suffer an intracranial injury compared to control patients. 2 A prospective study by Ganetsky et al 3 quoted a rate of intracranial hemorrhage of 3.5% in patients taking either anticoagulants or antiplatelet agents who sustained head trauma after a ground level fall at an urban Level I Trauma Center. There is also a risk of delayed intracranial hemorrhage (dICH) of up to 6% 4 amongst this patient population, which represents a potentially devastating complication. Much of this data is specifically associated with warfarin or antiplatelet agents. Collins et al 5 noted that patients taking warfarin had a 40% increased risk of intracranial hemorrhage when compared to those who were not anticoagulated. Our previously presented data regarding patients taking warfarin showed that risk of dICH increases with INR over 2, which led us to perform interval head CT scans in any patient on warfarin with whose INR met that threshold. 6 Given that the number of patients taking direct oral anticoagulants (DOACs), such as apixaban, rivaroxaban, and dabigatran has increased—now accounting for close to 80% of patients taking oral anticoagulation for atrial fibrillation 7 —more work is necessary to determine the ideal method of detection for dICH in this subset of patients.
A consensus has not been established in the literature regarding how best to screen for dICH in patients taking DOACs. Institutional protocols, including ours, are often derived from the warfarin data and vary from a period of observation of differing lengths to mandatory repeat head CTs at a number of different time intervals. Our study seeks to determine the rate of dICH in this population at our institution and to add to the growing body of literature regarding routine repeat head CTs in patients medicated with DOACs. We hypothesize that the rate of dICH will be lower in patients on DOACs than on warfarin therapy, and that there will be no clinically significant instances of dICH in this population.
Methods
A waiver was obtained from the Institutional Review Board at our institution, an American College of Surgeons Verified Level II Trauma Center in a small city. This was a single institution retrospective observational study. The institutional trauma database was queried for all patients evaluated by the trauma service at our center for ground level falls on anticoagulation from January 2016 to December 2018 (Figure 1). It is institutional policy that any patient on anticoagulation with head trauma is evaluated by the trauma service at the time of arrival. Data collected included age, gender, ethnicity, prescribed anticoagulant, initial Glasgow Coma Scale (GCS), presence of new neurologic deficits on arrival as documented in the trauma history and physical, results of initial head CT and results of repeat head CT, as well need for reversal agents and neurosurgical intervention. Patients were excluded if their GCS on arrival was less than 14, if they presented with new neurologic deficits, if there was evidence of traumatic intracranial pathology on initial head CT, if they were taking antiplatelet agents or other anticoagulants in addition to DOACs, or if a repeat head CT was not performed. However, patients presenting to the emergency department greater than 6 h after their fall and having only one head CT performed were included. Our primary objective was to determine the rate of dICH in patients sustaining head trauma in the setting of ground level falls on DOACs. Patient selection.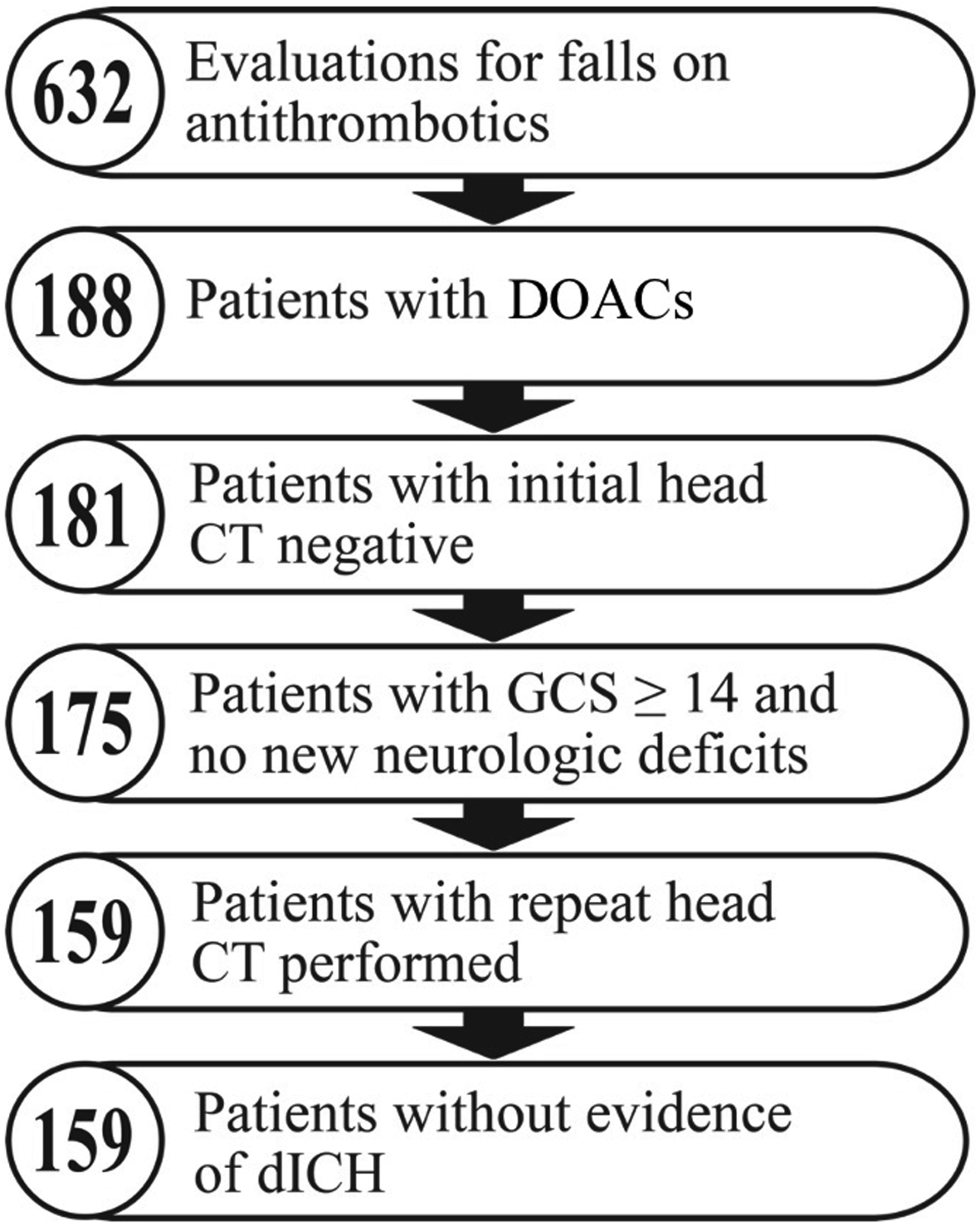
Results
Characteristics.
Discussion
Our data show that patients who sustain head trauma from ground level falls while taking DOACs have no risk of developing dICH. This differed significantly from our institutional experience with warfarin, where we had multiple instances of dICH, some of which led to neurosurgical intervention and all of which occurred in patients with INR greater than 2. This is consistent with published literature which demonstrates that the DOACs have a more favorable safety profile than warfarin, specifically in relation to intracranial hemorrhage.8,9 Additionally, there is a trend in our data with increasing use of DOACs toward the end of the study period compared with the beginning, also consistent with the national prescribing patterns. 7
We have since changed our institutional policy regarding the management of head trauma in patients on DOACs. Previously, all of our patients were admitted for a repeat head CT 6 h after their fall, although most patients remained in the hospital for 24 h or longer. This allowed for continued neurological assessment. During the study period, there were no patients who had a change in their neurologic exam after their interval scan. This indicates that any dICH that may have developed after the delayed CT scan was not clinically significant. With our new protocol, if the initial head CT is negative, and there are no neurological deficits on presentation, the patient is kept in the emergency department for 4 h of observation, after which time a member of the trauma team reevaluates the patient. If the patient remains neurologically intact, they are discharged home without repeat imaging. To date, we have had no patients who have required repeat head CT or admission for altered mental status. Changing this policy has led to a decrease in admissions to the trauma service, fewer unnecessary imaging studies, and decreased costs for the patients and our health care system.
There are limitations to our study. This was a retrospective, single institution study with a relatively small sample size. The results of our study should be taken in the context of a growing body of evidence suggesting that DOACs have a lower incidence of dICH than warfarin, and that routine repeat head CT is not necessary in this population. Even though we did not identify any instances of dICH in our population, we do believe there is a non-zero risk of this phenomenon in patients on DOACs. Despite this, ours is one of many studies that supports that routine screening for dICH in neurologically intact patients on DOACs may not be warranted. Future areas of study address patients on both anticoagulants and antiplatelet agents or patients on DOACs who present with altered mental status or loss of consciousness but have negative initial head CT, similar to the population studied by Livingston et al, to identify whether these populations are at higher risk for dICH and thus would benefit from more rigorous screening. 10
Footnotes
Author Contributions
M.B. performed literature review, M.B. and K.D. designed study, M.B. and G.T. performed data collection and analysis, and M.B. and K.D. contributed to the writing and critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.