
Abstract
Background
Current data on tranexamic acid (TXA) supports early administration for severe hemorrhagic shock. Administration by EMS has been facilitated by developing protocols and standing orders informed by these data. In this study, patterns of TXA use by EMS agencies serving a large level 1 trauma center were examined. We hypothesized that current widespread TXA use often includes administration outside of data-driven indications.
Methods
The trauma registry at a level 1 trauma center was queried for patients who received TXA. To determine the practice patterns and appropriateness of administration of TXA, patients’ physiologic state in the prehospital environment based on EMS records, physiologic state on arrival to hospital, and interventions performed in both settings were examined. Over 20 separately managed EMS systems that administer TXA transport patients to this trauma center, allowing for a broad survey of practices.
Results
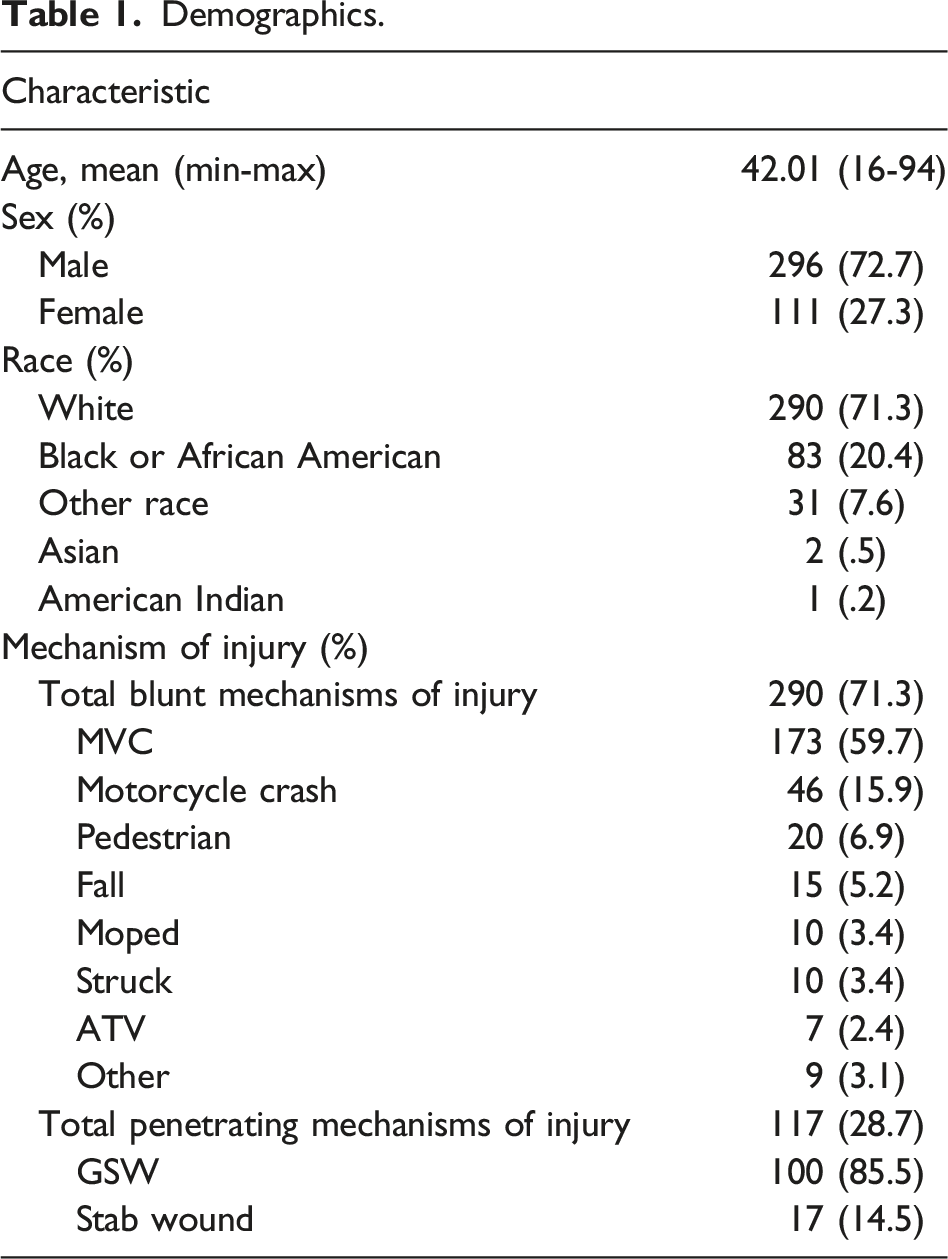
From 2016 to 2021 1089 patients received TXA, 406 (37.3%) having treatment initiated by EMS services. Of these, the average prehospital systolic blood pressure (SBP) was 108.2 mmHg and initial ED SBP was 107.8 mmHg. Only 58.4% of these patients received blood transfusion after arrival to this trauma center. Compliance with standard indications was low with only 14.6% of administrations meeting any data-driven SBP indication. Similar levels of compliance were seen across high volume EMS services.
Discussion
Tranexamic acid use has become common in trauma and has been adopted by many EMS systems. These results indicate TXA in the prehospital setting is over-used as administration is not being limited to indications that have shown benefit in prior data.
Key Takeaway
Tranexamic acid (TXA) is considered a relatively safe drug, but there are several potential risks associated with its use and only a subset of patients with low systolic blood pressure in the context of traumatic hemorrhage have shown benefit from TXA. In this study, EMS use of TXA was frequently beyond indications informed by data supporting benefit, likely due to vague protocols and limited education on TXA.
Introduction
The evolution of prehospital trauma care, facilitated by protocols and standard orders, has allowed earlier access to advanced interventions for injured patients. As many interventions for injured patients are time sensitive in their effects, there is potential for improved outcomes by making them available at first contact with the health care system. One example of such an intervention is early tranexamic acid (TXA) administration. Tranexamic acid is a synthetic lysine analogue that competitively binds the lysine receptor on plasminogen. This prevents plasmin(ogen) from binding fibrin, thus inhibiting the fibrinolysis pathway.1,2
Tranexamic acid has been shown to be valuable in several clinical scenarios. The CRASH-2 study showed that early administration enhanced the mortality benefit of TXA in traumatic hemorrhage, specifically, if given within 3 hours of injury. 3 The STAAMP trial attempted to recreate the findings of CRASH-2 but allowed for the administration of TXA within the prehospital setting. A mortality benefit of the TXA administration was seen in patients with systolic blood pressure (SBP) < 70 mmHg. 4 Similarly, subgroups that benefited from TXA in the CRASH-2 study were those with initial SBP ≤75 mmHg. 3
Although TXA has been shown to be valuable in several trials, concern exists regarding an increased risk of thrombotic complications and seizures.5,6 While often debated, several studies have identified increased thrombotic risks associated with the administration of TXA to injured patients, particularly with higher doses.7-12 Some data suggests the administration of TXA to patients with normal fibrinolysis may have a negative impact on mortality.13,14 Further, a meta-analysis conducted in 2016 found both a dose-dependent risk of seizures in cardiothoracic surgery patients who received TXA. 9 Additionally, the ideal dosage for TXA usage has not been clearly agreed upon in the literature and remains a topic of debate.5,6
As a general principle, interventions should be given to those patients for whom data support a possibility of benefit, and those unlikely to benefit should not be exposed to unnecessary risk. With the nuanced, limited, and sometimes conflicting data available for TXA, it is important that its use is guided by data. Several studies have previously identified a significant number of cases in which TXA has been administered without a clear clinical indication resulting in attempts to better standardize administration protocols at other facilities.15,16 This study, designed as a quality improvement project, examines practice, use, and compliance with data-supported indications of TXA administration within multiple EMS systems serving a large level 1 trauma center. We hypothesized that current widespread TXA use often includes administration outside of the physiologic parameters found to yield a mortality benefit within the previously published large multicenter trials. Thus, our objective was to evaluate if our current administration practices expose this medication to those who may not benefit from administration of TXA.
Methods
This is a retrospective review of the trauma registry at a state-designated and ACS-verified level 1 trauma center. This study was designed as a quality improvement project to identify appropriateness of TXA administration in the prehospital setting. This study was approved by the institutional review board (IRB# 00093599). The trauma registry was queried for patients who received TXA in the course of their initial resuscitation over a 5-year period from 2016 to 2021. To determine the practice patterns of administration of TXA, patient’s physiologic state in the prehospital environment based on EMS records (field vital signs including heart rate and blood pressure), physiologic state on arrival to hospital (first set of hospital vital signs including heart rate and blood pressure), and interventions performed in both settings (in particular, blood administration and tourniquet application) were examined. Thirty-seven separately managed EMS systems that administer TXA transport patients from the scene to our trauma center were included in this study. Systolic blood pressure (SBP) at or below 90, 75, and 70 mmHg were used as metrics to evaluate TXA administration based on CRASH-2 inclusion criteria, patients that had a mortality benefit in the STAAMP trial, and patients that had a mortality benefit in the CRASH-2 trial respectively. These SBP metrics were chosen based on previously reported inclusion criteria or mortality benefit in the aforementioned large multicenter trials. Additionally, a broad survey of protocols for TXA administration from multiple EMS systems was evaluated to identify areas for improvement. Normally distributed data is presented as mean ± SEM while non-normally distributed data is presented as median and interquartile range.
Results
Demographics.
Compliance by SBP Indication Standards.

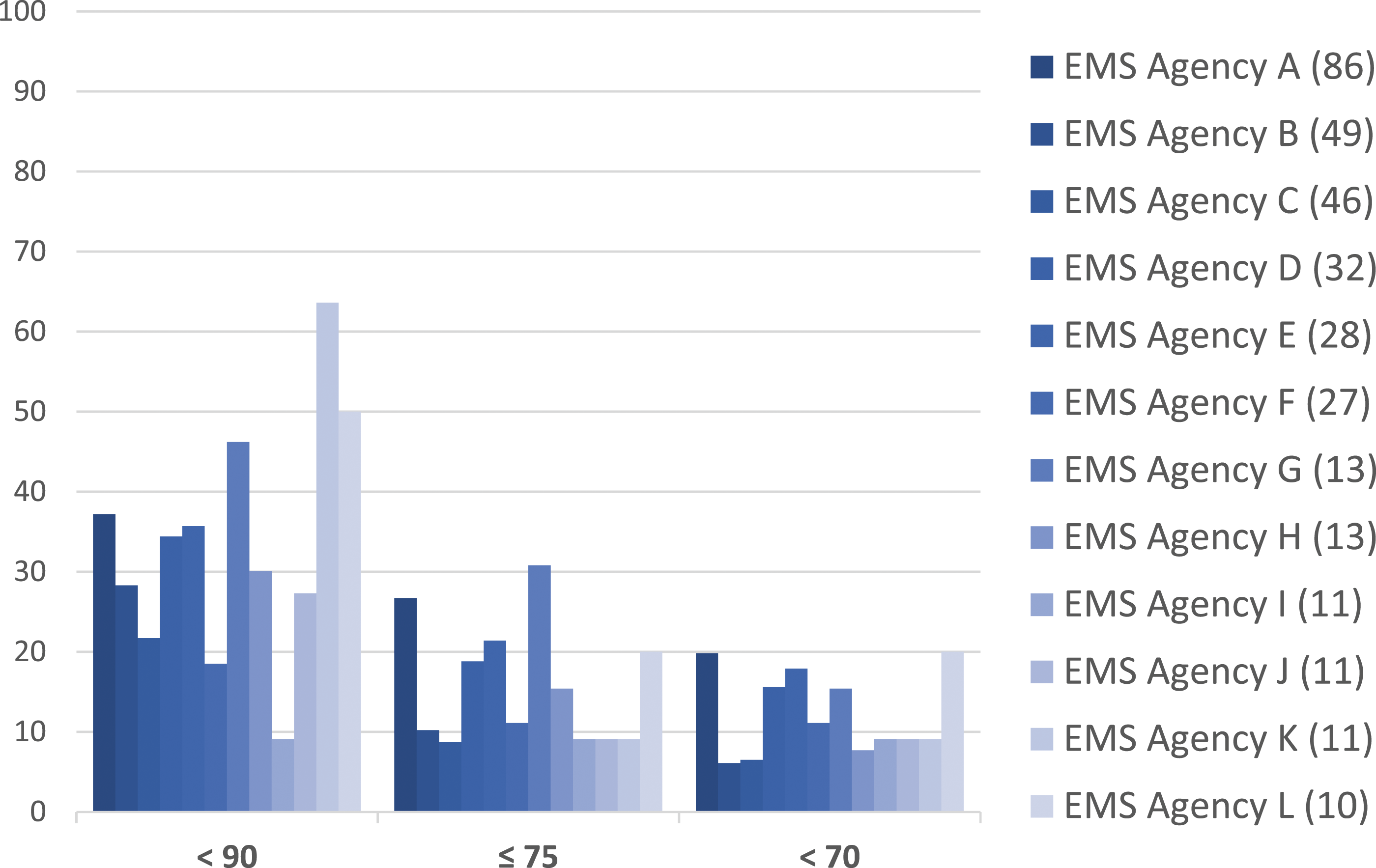
Percent compliance by individual de-identified agencies (total n).
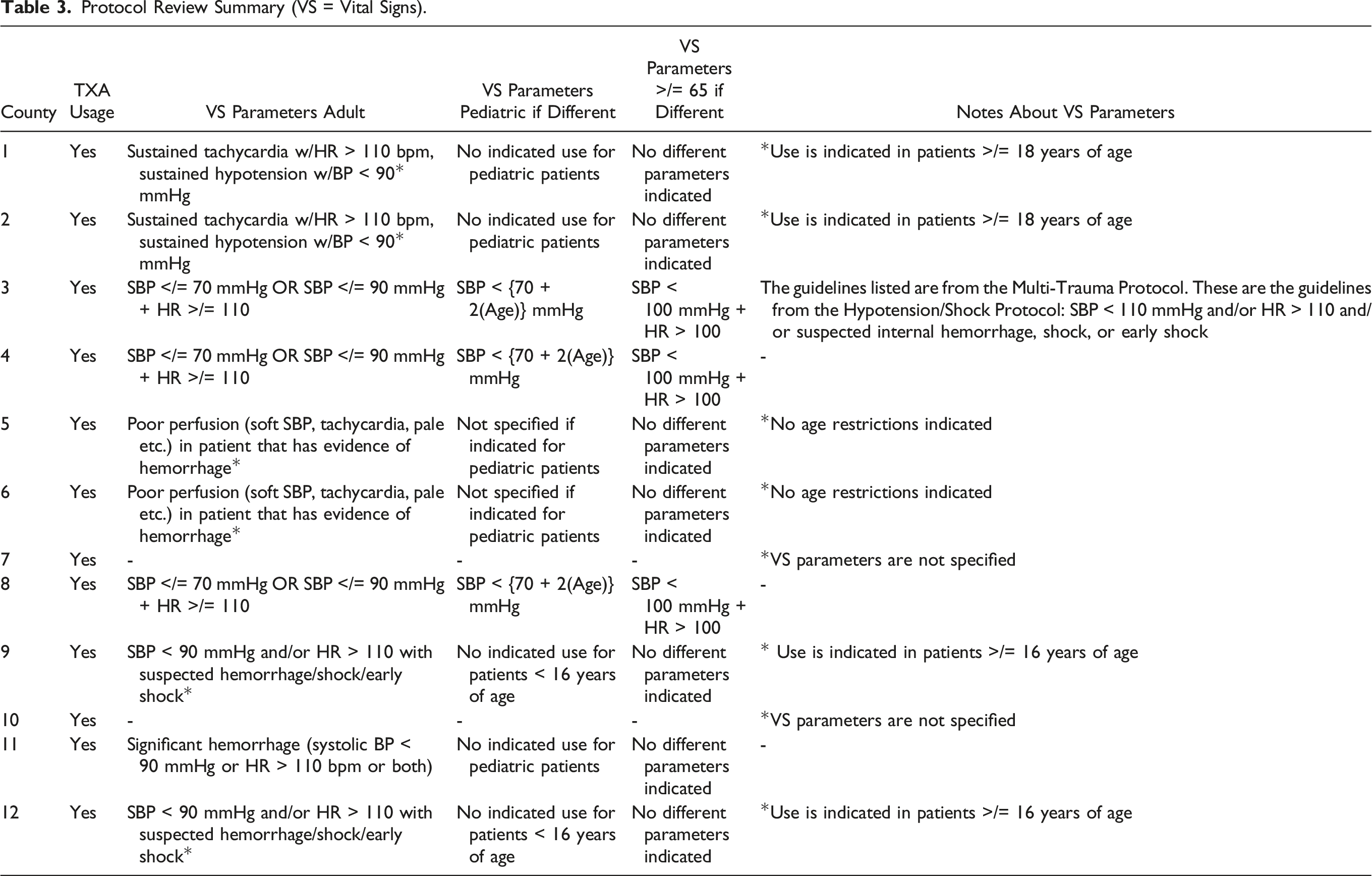
Protocol Review Summary (VS = Vital Signs).
Discussion
This study shows that TXA administration to patients that have physiologic parameters that meet data-driven mortality or study inclusion metrics is low. Less than 15% of patients receiving TXA had an SBP below the highest cutoff showing mortality benefit (≤75 mmHg in CRASH-2). We also identified a large amount of variability in TXA administration protocols between EMS agencies. The guidance of these protocols provides a framework for practice patterns. However, we suspect that a large driver toward the low compliance with TXA administration based on SBP metrics is based on differences in both interagency as well as state protocols regarding the use of TXA for the severely injured patient.
Several studies have found evidence that early administration of TXA is associated with improved mortality. The CRASH-2 study showed that TXA administration within 3 hours of injury improved mortality in patients with traumatic hemorrhage, with the greatest benefit seen when given as early as possible. After 3 hours, TXA administration was associated with increased mortality. 3 An exploratory analysis of the CRASH-2 trial showed that this effect of time of administration was not explained by differences in SBP, injury type, or GCS of patients. 17 The CRASH-3 study, which evaluated effects of TXA administration in patients with traumatic brain injury, showed improvement in head injury-related death with TXA administration. This study also identified the greatest benefit in patients who were administered TXA at an early time point. 18 The STAAMP study evaluated the potential benefits of administering TXA in the prehospital setting. Although the STAAMP trial did not find an overall improvement in mortality with TXA administration, it did show improved mortality in a subgroup of patients who received TXA within 1 hour of injury. 4 While these studies have revealed the value of TXA in the injured patient, several other studies have underscored the potential complications or risks associated with the use of TXA.7-11,13,14 Making TXA available to EMS allows for administration at the earliest point of contact of a patient with the medical system. However, as scope of EMS expands to provide earlier and more advanced care, it is vital to ensure that their protocols reflect administering interventions to patients who will truly benefit from it and avoid administration in situations it may cause harm.
Much of the research surrounding TXA has focused on the timing of administration. Unfortunately, our study was not able to elucidate the timeliness of administration as another possible point of improvement. However, given that a significant number of patients had TXA administered by EMS in the prehospital setting, it can be inferred that most of these patients were administered TXA within the appropriate time frame. The relationship between blood pressure and the benefits of TXA administration has been examined in several large studies including CRASH-2 and STAAMP.3,4 Subgroup analyses showed benefit in patients with SBP ≤ 75°mmHg and <70 mmHg, respectively.3,4 SBP of less than 90 mmHg is used as a physiologic inclusion criterion of hypotension in both the CRASH-2 and STAAMP trials.3,4 Although SBP of less than 90 mmHg is widely accepted as identifying shock in the injured patient, this cutoff has no evidence of benefit in the context of TXA administration. We found that over 70% of patients that received TXA in the prehospital setting had SBP > 90 mmHg (Table 2). Further, if we use SBP of ≤75 mmHg or <70 mmHg as metrics to identify patients that should have a mortality benefit to TXA administration, we found that TXA is administered more than 85% of the time to patient’s who, based on CRASH-2 and STAAMP data, would not benefit.3,4 This finding is prevalent among all EMS agencies we evaluated (Figure 1). A review of the highest volume EMS agency protocols further revealed that the most common SBP parameter to administer TXA was <90 mmHg (Table 3). Many of these agencies also indicate a heart rate parameter to initiate TXA administration. However, no data has shown that there is a benefit of TXA administration based on HR. Tachycardia (HR > 110) was used as an inclusion criterion for both CRASH-2 and STAAMP, but the effects of TXA on mortality in patients with isolated tachycardia were not actually evaluated in CRASH-2 and patients with isolated tachycardia were shown to have no mortality benefit from TXA in STAAMP.3,4 Our findings are consistent with a study evaluating utilization of TXA in an aeromedical transport system. 15 This study revealed that 43% of patients that received TXA by the aeromedical transport service that serviced a busy level 1 trauma center had no evidence of hemorrhage upon arrival to the hospital, indicating that TXA administration was likely over utilized in their patient population. 15 Further, a review of TXA usage in the prehospital settings revealed at least 30% of patients may have received TXA but had no clear clinical indication for the administration of the medication. 16 In the uncontrolled environment of the prehospital system, application of protocols is generally pragmatic rather than perfect, which could contribute to some inclusion of patients with SBP just above given cutoffs. However, enhancing this inclusion creep with variable or unclear protocols can expose patients to therapy that may not add benefit based on their physiology.
Another issue identified in this quality improvement project was in the identification of several cases TXA was administered in the setting of isolated extremity injury, sometimes when a tourniquet was in place. Of the patients that had a tourniquet applied in the prehospital setting, 68% of patients also received TXA. After their value was proven in military settings, 19 tourniquet use has been adopted in civilian EMS systems and is currently considered an important part of standard of care for extremity hemorrhage. Combining TXA and tourniquet use in trauma has not been well studied, although TXA has been shown to decrease intraoperative blood loss in the case of extremity trauma. 20 This combination has been examined in elective orthopedic surgery where the addition of TXA to tourniquet use has been shown to decrease blood loss. 21 However, in these cases TXA is given prior to tourniquet application and as such, reaches the site of incision to act locally. In prehospital management of extremity trauma, it is contrary to basic ATLS principles to delay tourniquet placement if indicated to administer medication. As such, TXA does not reach the injury site until after the tourniquet is removed. During this time not only is TXA being metabolized, decreasing the circulating amount the medication is in contact with the injury site, but the patient is also exposed to all potential risks without benefits. There is evidence that TXA also has anti-inflammatory activity, 22 which could be beneficial systemically while a tourniquet is in place. However, the significance of any anti-inflammatory effect in the setting of isolated extremity trauma with a tourniquet in place before TXA has been administered has not been examined.
As all systems fall under the same state protocol outline, the lack of specific guidance used to create agency protocols leaves more room for individual interpretation of available data and leads to variation in agency practice patterns. As a result of this inquiry, the state protocols are now being revised to include strict data-driven vital signs and mechanistic indications for TXA administration. Although this is a geographically limited study, we suspect that our findings would be replicated at other institutions and an examination of local EMS protocols in other geographic areas may help standardize protocols for TXA administration to target giving this medication to the patients that will benefit the most.
Limitations of This Study
This study has several limitations. There are inherent limitations given the retrospective nature of the study. Similarly, there are limitations based on the inclusion of EMS systems serving only a single level 1 trauma center. Although there are many separate EMS systems examined, there are certainly regional, cultural, and educational elements that are shared between these agencies. Further, data is only as accurate as documentation and inclusion within the trauma registry and details of EMS care such as timing of TXA administration, and specific indications for tourniquet use were not available. Many of the EMS protocols allow for administration based on concern for hemorrhage and not necessarily strict physiologic criteria. It is not possible, based on documentation, to identify the specific indication used to administer TXA for each individual patient.
Conclusions
Tranexamic acid use has become common in trauma management and has been adopted by many EMS agencies. However, these results indicate that TXA in the prehospital setting may be over-used as administration is not being limited to metrics that have shown significant clinical benefits. As a result of this quality improvement inquiry, the state protocol, which acts as a template for all regional protocols, is in the process of being re-written with a plan for the regional protocols to follow. Further studies should be aimed at evaluating compliance following initiation of new protocols, effects on clinical outcomes and complications, and cost associated with change in protocol.
Footnotes
Author Contributions
AMPB contributed to study design, data acquisition and analysis, interpretation of data, manuscript writing, and edits. MF contributed to data acquisition and analysis, manuscript writing, and edits. GRS contributed to study design, interpretation of data, and manuscript edits. JW contributed to data acquisition and analysis, interpretation of data, and manuscript edits. RSM contributed to study design, data analysis, interpretation of data, and manuscript edits.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentations
This paper was presented at EAST Annual Scientific Assembly 2023 as a podium presentation.