
Abstract
Across the nation, patients with locally advanced gastric cancer (LAGC) are managed with modalities including upfront surgery (US) and perioperative chemotherapy (PCT). Preoperative therapies have demonstrated survival benefits over US and thus long-term outcomes are expected to vary between the options. However, as these 2 modalities continue to be regularly employed, we sought to perform a decision analysis comparing the costs and quality-of-life associated with the treatment of patients with LAGC to identify the most cost-effective option. We designed a decision tree model to investigate the survival and costs associated with the most commonly utilized management modalities for LAGC in the United States: US and PCT. The tree described costs and treatment strategies over a 6-month time horizon. Costs were derived from 2022 Medicare reimbursement rates using the third-party payer perspective for physicians and hospitals. Effectiveness was represented using quality-adjusted life-years (QALYs). One-way, two-way, and probabilistic sensitivity analyses were utilized to test the robustness of our findings. PCT was the most cost-effective treatment modality for patients with LAGC over US with a cost of $40,792.16 yielding 3.11 QALYs. US has a cost of $55,575.57 while yielding 3.15 QALYs; the incremental cost-effectiveness ratio (ICER) was $369,585.25. One-way and two-way sensitivity analyses favored PCT in all variations of variables across their standard deviations. Across 100,000 Monte Carlo simulations, 100% of trials favored PCT. In our model simulating patients with LAGC, the most cost-effective treatment strategy was PCT. While US demonstrated improved QALYs over PCT, the associated cost was too great to justify its use.
Introduction
Gastric cancer (GC) is the third leading cause of cancer deaths worldwide and is predicted to cause over 11,000 deaths in the United States in 2023.1,2 Gastric cancer is commonly diagnosed at advanced stages and thus carries a particularly poor prognosis.3,4 Gastrectomy remains requisite for the curative treatment of locally advanced GC (LAGC), defined as at least clinical T2 disease with or without nodal involvement. 5 The Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial published in 2006 was the first study to show a survival benefit with perioperative chemotherapy (PCT) in comparison to surgery alone. 6 This study spurred further research into identifying optimal chemotherapy regimens; in the current era upfront surgery (US) and PCT are both regularly utilized treatment modalities across the globe and in the United States.3,7,8
While the NCCN Guidelines recommend PCT for the treatment of LAGC with the highest level-of-evidence (LOE), across the nation patients with GC are managed with US at rates between 25% and 35%.7-9 US is usually succeeded by adjuvant therapy with adjuvant chemoradiation (CRT) or adjuvant chemotherapy both of which have been shown to reduce recurrence rates and increase survival.10,11 Literature reports physicians opt for surgery first in patients with poor performance status or in those with severe comorbidities.12,13 Access to tertiary centers in the community may also limit the number of patients for whom PCT is possible. Head-to-head randomized control trials comparing US (category 2A LOE) and PCT (category 1 LOE) have not been performed. It is in this setting that our study strives to utilize a cost-effectiveness lens and compare the most frequently used and best supported treatment strategies against each other. Herein, we performed a decision analysis comparing the costs and quality-of-life associated with the treatment of patients with LAGC to identify the most cost-effective option.
Methods
Decision Tree Design
We designed a decision tree model to investigate the survival and costs associated with both commonly utilized management modalities for LAGC in the United States: US and PCT (Figure 1). Neoadjuvant CRT, on the other hand, is growing in popularity but remains an understudied modality; thus, it was not included in the model due to the lack of comparable data available in the literature. The methodology used to build this model has been previously described by our group.14-18 The tree encapsulates costs accrued over 6 months to incorporate the complete treatment regimen. Due to this short time horizon, a decision model was used instead of a Markov model and discounts were not required. Our model represents potential outcomes for a theoretical cohort of patients. The probabilities of these outcomes occurring, and the survival associated with each of these outcomes, were derived from the published literature. First, the ideal patient cohort for this study was defined as patients with LAGC. It excluded patients with gastroesophageal cancer, unresectable LAGC, metastatic or recurrent GC, and those who received palliative therapy. Recent published studies that addressed outcomes for these included patients were then identified. Decision tree model used for analysis. Percentages included are best estimates derived from the literature.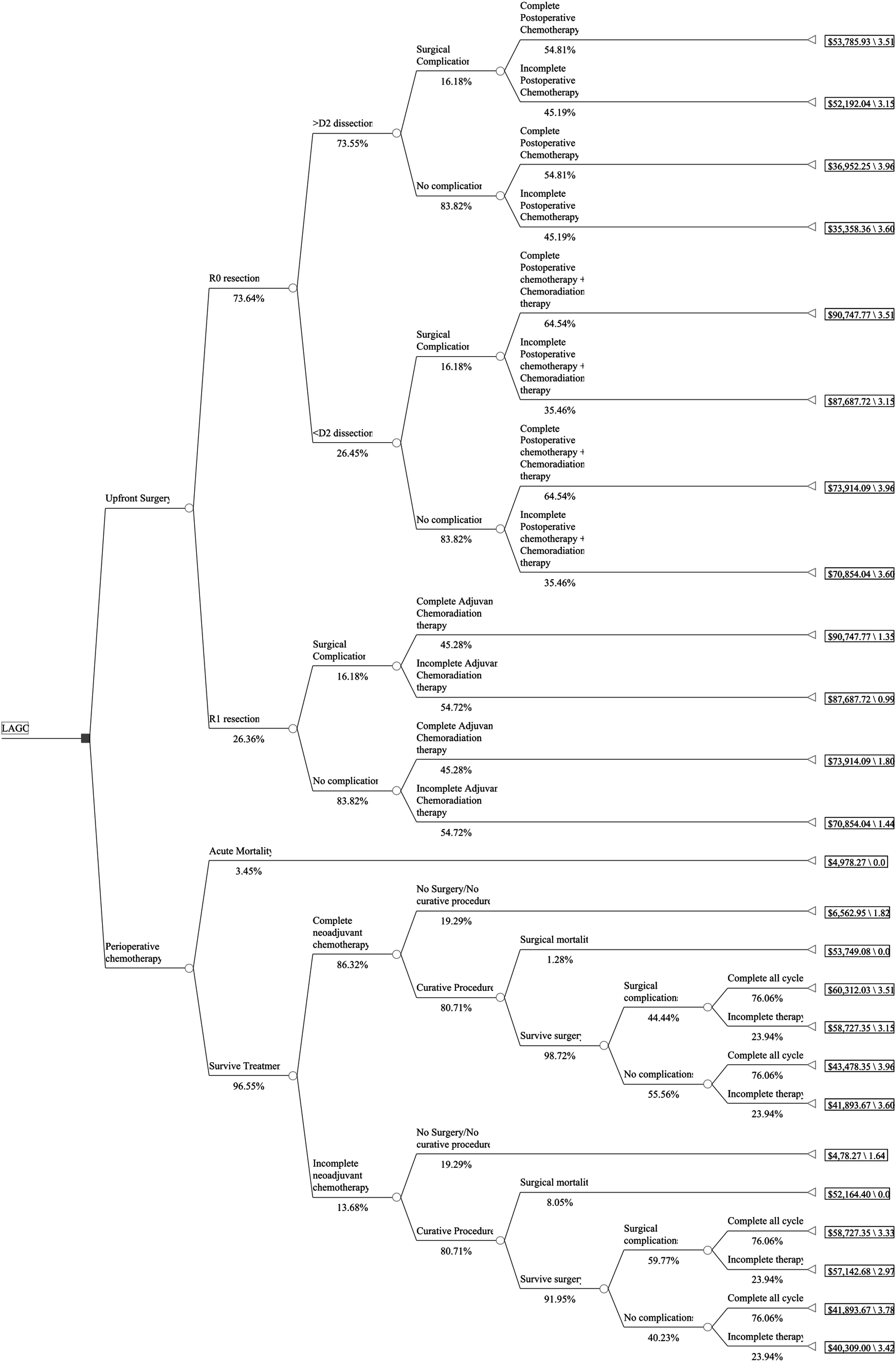
In our study, treatments were defined based on NCCN recommendations including chemotherapy and radiotherapy dosages and dosing schedules. 9 The diagnostic workup, such as diagnostic laparoscopy, was not included as our theoretical patients were assumed to have undergone this examination prior to treatment. Our study included perioperative fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) therapy in the PCT arm as it is the preferred regimen, carrying a category 1 LOE.9,19 Patients in the PCT arm were ascribed 4 cycles of neoadjuvant chemotherapy, gastrectomy with regional lymph node dissection, and 4 cycles of adjuvant chemotherapy.
After US in patients who had R0 resection and underwent a D2 or greater lymph node dissection, postoperative chemotherapy was recommended per the NCCN guidelines.11,20 Patients were assumed to receive 8 cycles of capecitabine and oxaliplatin cycled every 21 days as it as a preferred regimen carrying category 2A LOE.11,21 Patients who had R0 resections (no cancer at resection margin) but received less than a D2 lymph node dissection received postoperative chemotherapy and CRT. 10 Per NCCN Guidelines, they received 2 cycles of fluorouracil and leucovorin chemotherapy, followed by 5 weeks of fluorouracil chemoradiation, and finishing with 4 more cycles of fluorouracil and leucovorin chemotherapy. Finally, patients who had US but received R1 resection (microscopic residual disease) required adjuvant CRT.9,22 Adjuvant CRT also consisted of 6 cycles of fluorouracil and leucovorin chemotherapy and 5 weeks of fluorouracil-based CRT. 9
Some patients do not complete preoperative or postoperative therapy as planned. Incomplete therapy was defined as discontinuation prior to completion of the recommended number of cycles for reasons including adverse effects or disease progression. If preoperative chemotherapy was incomplete, patients were expected to progress to surgery and would be prescribed the regular number of adjuvant chemotherapy cycles, when possible. We additionally assumed patients who were unable to receive curative surgery received palliative care instead. 23
Data Selection
Decision Tree Probabilities.

Aggregate Decision Tree Costs.
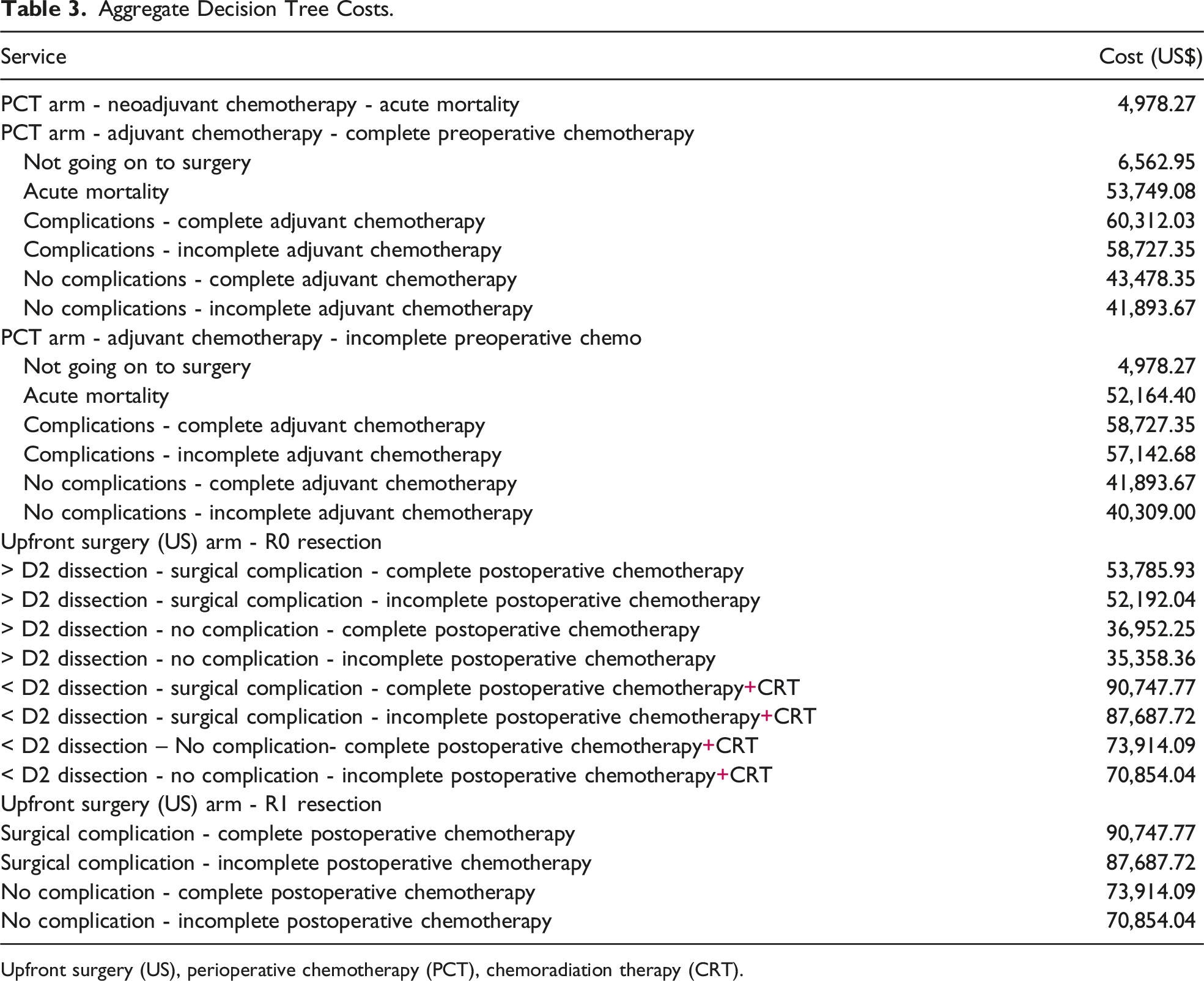
Upfront surgery (US), perioperative chemotherapy (PCT), chemoradiation therapy (CRT).
Decision Tree Costs.
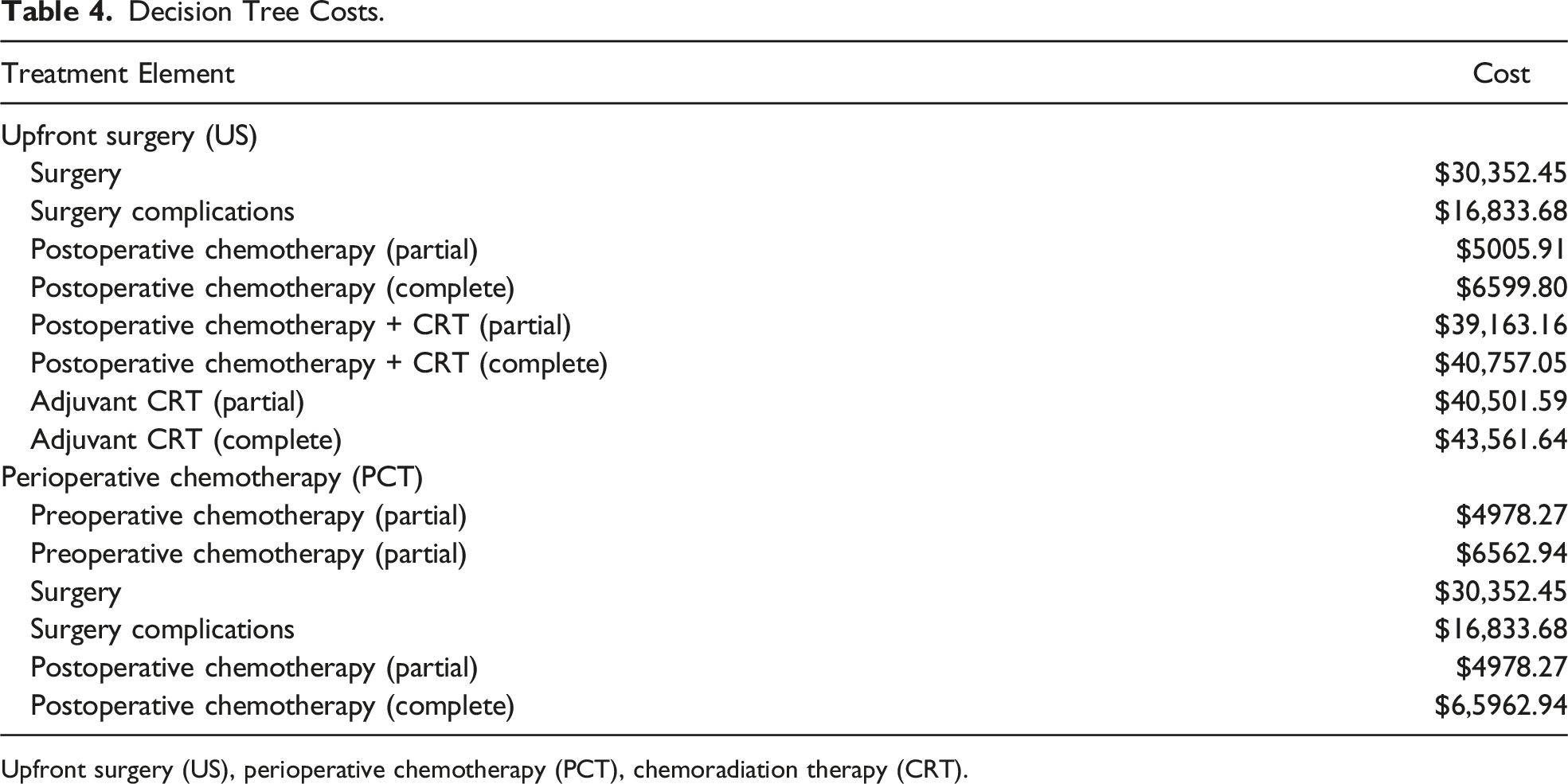
Upfront surgery (US), perioperative chemotherapy (PCT), chemoradiation therapy (CRT).
Costs were derived from 2022 Medicare reimbursement rates using the third-party payer perspective for physicians and hospitals. Data were obtained from the Medicare Inpatient and Outpatient Prospective Payment System, the Medicare Physician Fee Schedule, and the Medicare Part B Average Sales Price Drug Pricing File (FY2022) (Table 3-4). Costs secondary to gastrectomy and hospital stay, chemotherapy drug costs, medication administration, radiation therapy, and associated office visits were included in the analysis. A significant proportion of costs are associated with both fees surrounding postoperative inpatient length-of-stay and radiation therapy administration. As costs can vary widely across state lines, reimbursement rates were made to act as a proxy for hospital bills. We assume total reimbursement costs will allow for direct comparisons between treatment arms as total billed costs should vary directly with reimbursement rates.
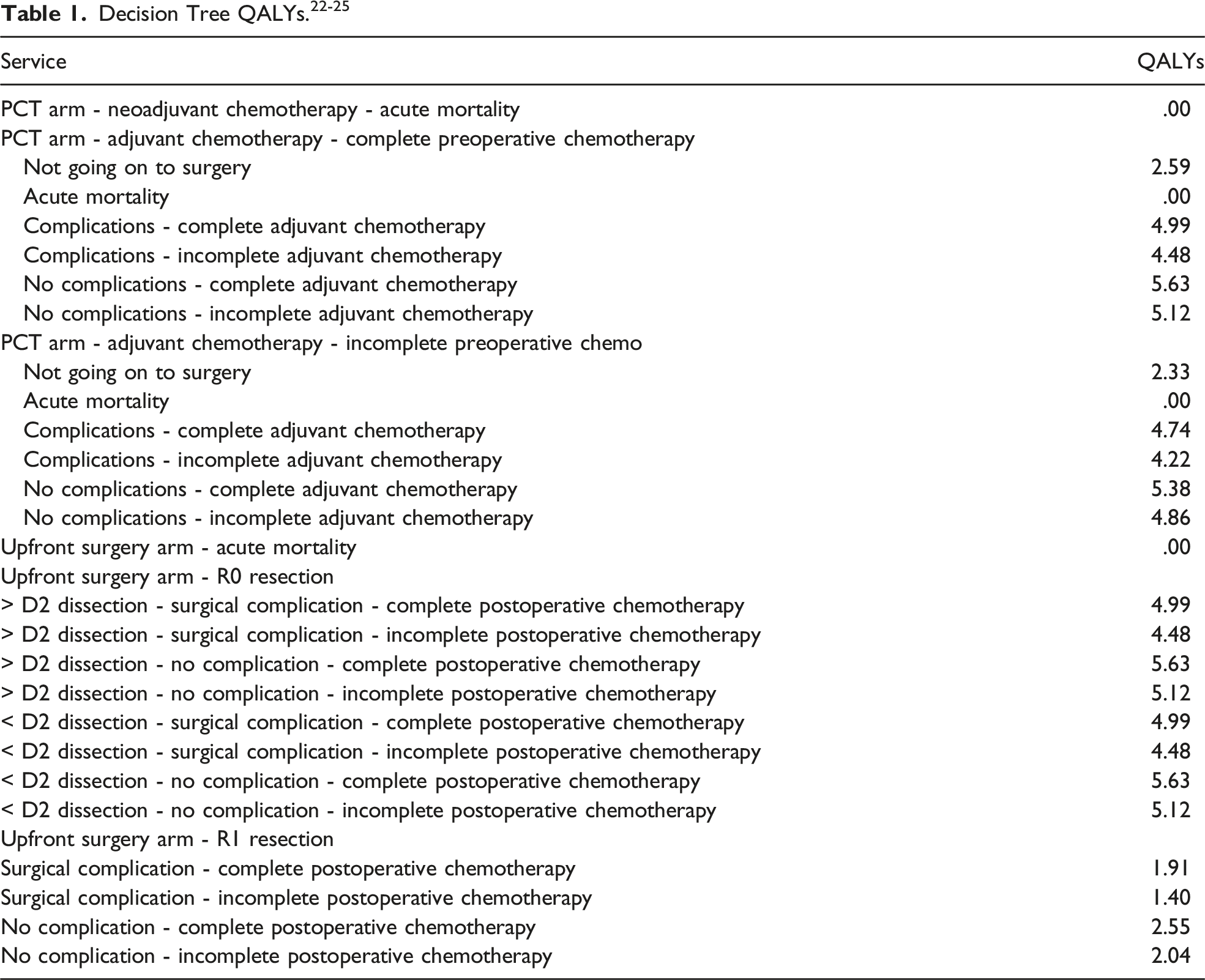
Effectiveness was represented using quality-adjusted life-years (QALYs). One QALY equates to a year of perfect health, while zero QALYs is equivalent to death. QALYs are tabulated in Table 1. Morbidity is calculated using a baseline utility for complete curative treatment with the subtraction of disutility values based on the severity of encountered complications. For all 3 arms, the base utility for a complication-free treatment was set to .88.22,24 Patients who had incomplete preoperative chemotherapy were assigned a disutility weight of −.04. We assumed incomplete adjuvant therapy yielded greater disutility than incomplete neoadjuvant therapy as these patients had undergone a procedure with notable morbidity.27,29,31 Thus, incomplete postoperative chemotherapy was assigned a disutility weight of −.08. In the PCT arm, those who did not undergo a surgical procedure and were moved to palliative care were assigned a utility weight of .404. 23 Across the tree, those who underwent non-curative procedures or had an R1 resection were assigned a utility weight of .399 due to the added morbidity of undergoing a surgical procedure. In both arms, acute mortality was assigned a utility weight of zero. Studies reporting on US identified no acute mortality; thus, this branch was removed from the tree.28,32 The absence of acute mortality in the US arm could be related to the lack of neoadjuvant therapies which may weaken patients before such a large procedure. 33
The American Cancer Society reported the average age of a patient diagnosed with GC was 68 years old. 34 As GC is known to more often affect male patients, Social Security Actuarial tables were used to identify the life expectancy for a 68-year-old male.1,35 This value was used in conjunction with 5-year survival rates also reported by the American Cancer Society and the declining exponential approximation of life expectancy (DEALE) method to arrive at a life expectancy of 4.5 years for the patients diagnosed with LAGC who are included in our study.34,36 Utilization of the DEALE method has been further explained in previous studies by our group.14,15,37
Comprehensive surgical complication data after completion of a preoperative FLOT regimen could not be identified in the literature for use in our PCT arm; data from the CRITICS trial,29,31 which utilized 3 preoperative cycles of epirubicin, cisplatin or oxaliplatin, and capecitabine (ECC/EOC), was chosen as the closest approximation as Classen et al stratified their data elements by completion or lack of completion of neoadjuvant therapy. While there were concerns about additional toxicity and complications associated with FLOT, recent literature found ECC and FLOT to have no significant differences in perioperative complications. 38 Data from the FLOT4 study by Al Batran et al was considered but ultimately excluded due to lack of stratification in this regard. 19
Statistical Analysis
Incremental cost-effectiveness ratio (ICER) was the primary outcome of our study. The a priori willingness-to-pay (WTP) for each QALY gained was $100,000, and marked the threshold for determining the most cost-effective treatment strategy. 39 Ineffective treatment strategies are represented by negative ICER values or ICER values computed above the threshold for determination. Cost-effectiveness analyses were performed in TreeAge (TreeAge Software, Williamstown, MA). The robustness of our conclusions was tested with one-way sensitivity analyses where each of the variables included in Table 2 were varied about ranges seen in the literature. Variables found to be significant in the one-way analyses were further analyzed in subsequent two-way analyses. Finally, we utilized 100,000 Monte Carlo simulations to perform a probabilistic sensitivity analysis with the triangle sampling method.
Results
Incremental Cost-Effectiveness Values for Base Case.

Across 100,000 Monte Carlo simulations, 100% of trials favored PCT. Perioperative chemotherapy costs ranged from $37,000 to $42,000 with QALYs between approximately 2.9 and 3.4. US, on the other hand, had costs ranging from 53,000 to 60,000 with QALYS between 2.8 and 3.3. Figure 2 shows 1000 samples from the aforementioned analysis for improved visualization. Finally, one-way and two-way sensitivity analyses did not identify any situations where an alternative treatment modality was preferred over PCT. Scatterplot of the first 1000 of 100,000 Monte Carlo probability simulations. Only the first 1000 simulations are shown for improved visualization.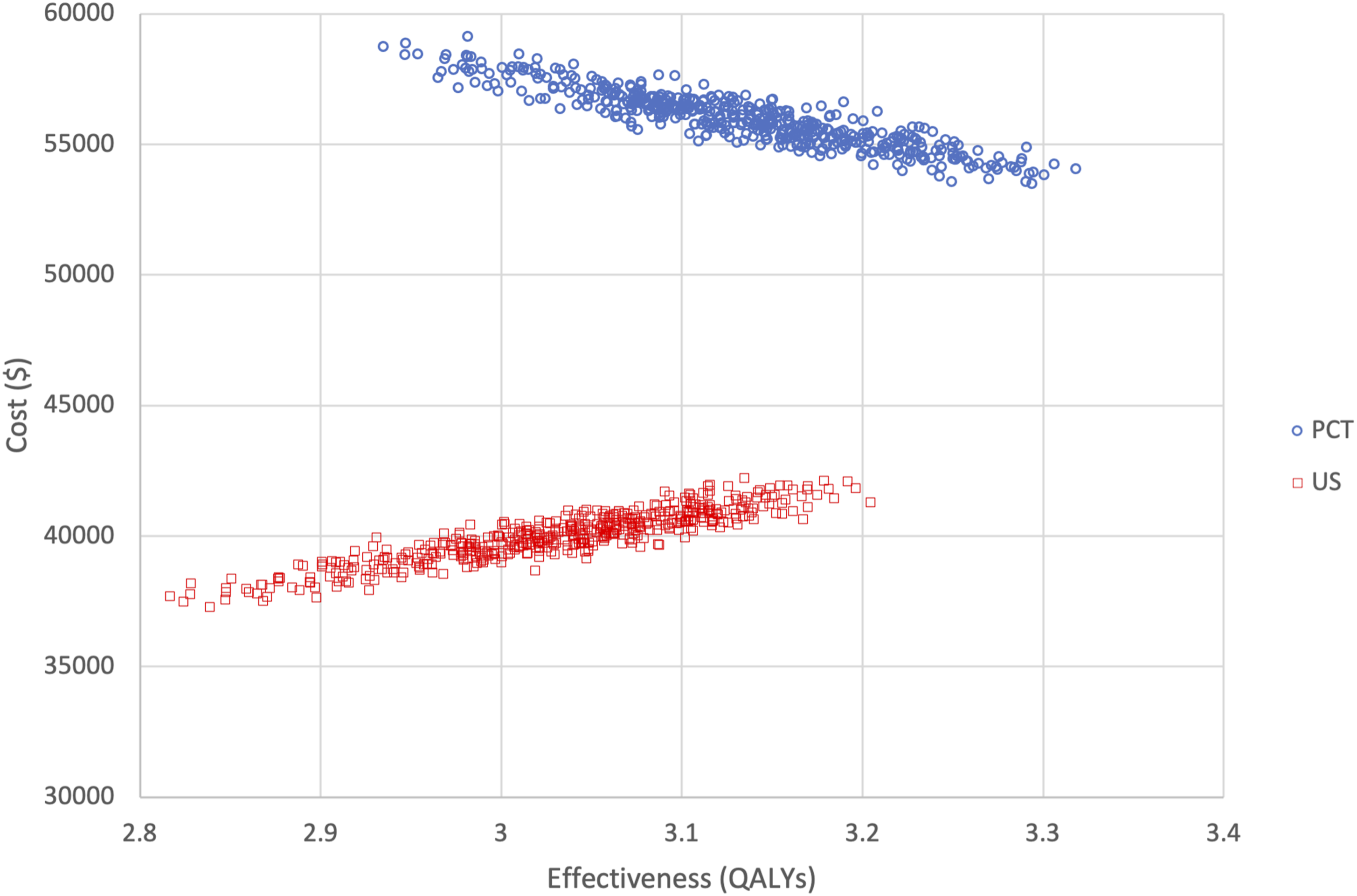
To identify situations where US may become cost-effective, secondary analyses outside of the preset confidence intervals obtained from the literature were utilized. US became more cost-effective than PCT when R1 resection rates approached 0%. Additionally, when acute mortality in PCT and surgical mortality after completing neoadjuvant chemotherapy increased beyond values established in the literature, we found US dropped below the preset WTP threshold making it a cost-effective treatment option.
Discussion
GC is a disease with high morbidity and mortality as it is often diagnosed at a late stage. Currently, NCCN Guidelines recommend treatment for LAGC with PCT or US, but these modalities have not been compared head-to-head in a clinical trial. 9 While PCT maintains category 1 evidence and US has category 2A evidence, recent studies by Anderson et al and others report both PCT and US are still regularly used across the country.7,8,40 Our study aimed to ascertain the difference in cost and effectiveness between PCT and US.
By using a decision tree model designed for patients with LAGC, our study showed PCT was the more cost-effective treatment strategy over US. With QALY values of 3.11 and 3.15 for PCT and US, respectively, cost was the factor ultimately responsible for determining the more cost-effective modality, depicted by the ICER of greater than $300,000. The sensitivity analyses and Monte Carlo simulations further supported this result and supported PCT over US in 100% of simulations. As such, our results concur with the NCCN guidelines in their recommendation to use PCT.9,41
With an increase in cost of nearly $15,000 per patient treated with US instead of PCT, we can estimate nearly $100 million of excess costs in the United States annually due to the continued usage of US as reported by Ikoma et al. 9 Furthermore, a systematic review for patients with LAGC reported disease-free survival rates ranged from 31% to 75% in US and from 59% to 80% in neoadjuvant chemotherapy. Without head-to-head Phase III studies, this systematic review alludes to some differences in survival we might expect to see between US and PCT. 42 As such, recent literature reports the usage of US has been declining over the last few years but updated studies are necessary to further describe this trend while improving access to PCT and preoperative treatment adherence for patients with LAGC in the community.7,8 Our study did not identify any subgroup of patients for whom US was more cost-effective, but data from future trials may aid in determining if such a group exists and can more accurately describe the overall survival and disease-free survival rates of the 2 groups. Even in the absence of this information, these population-based results should not discount the importance of risks or benefits associated with an individual patient’s case. Issues including reduced performance status and concerns about adherence with preoperative therapy should always be considered.
While cost-effectiveness studies have been utilized in the field of GC research for over a decade, prior studies have only investigated adjuvant therapy modalities.24,43 Our study is the first cost-effectiveness analysis directly comparing US and PCT. Both treatment branches contain surgical intervention as it remains a cornerstone in GC treatment; therefore, in this study we are primarily assessing the cost-effectiveness of neoadjuvant chemotherapy. Recent studies have consistently reported benefits of various PCT treatment regimens, 31 especially FLOT-based therapies which have been shown to improve overall survival. 19
Ultimately, cost prevented US from being the preferred treatment modality in our analysis. Several factors contribute to the significant price tag associated with US including potential adjuvant CRT administration and more specifically radiation therapy. Newer formats of radiation delivery including intensity modulated radiotherapy (IMRT) are currently used for GC treatment and are costlier than standard regimens.44,45
To ensure this study used the most recent and prevalent treatment modalities for GC, some assumptions had to be made while building the tree. We did not differentiate between partial, subtotal, and total gastric cancer surgery in our decision tree. Despite the elevated morbidity and mortality of total gastrectomy over subtotal gastrectomy, we determined separating between types of GC surgery was not possible in our analysis due to insufficient data from the literature. We also found most studies did not differentiate between adjuvant treatment outcomes after different levels of GC resection.6,10,11 As surgery was such a vital component of our analysis, we did not include advanced gastric cancers in our model because surgery is generally not an option for these patients who usually receive chemotherapy or CRT.
Our study assumed patients receiving radiation therapy were treated with IMRT which was reported to be standard practice for radiation therapy in the literature. 22 Our findings may not apply to patients who do not receive IMRT. As such, US may be more cost-effective in these patients due to a decrease in costs associated with non-IMRT radiation therapy. Likewise, our analysis assumed patients received FLOT perioperative chemotherapy while another NCCN guideline preferred option was 6 total cycles of fluoropyrimidine and oxaliplatin. 9 As this regimen required fewer cycles, fewer drugs, and thus fewer infusions, costs associated would be lower, which may further support PCT over US. However, literature suggests capecitabine is non-inferior when compared to 5-FU in terms of overall survival; thus, we assume at least QALYs would remain equivalent with either regimen. 46
Immunotherapy is another novel form of systemic therapy currently being assessed in GC. At this stage, the literature has reported on the efficacy and cost-effectiveness of immunotherapy in combination with chemotherapy in the treatment of advanced GC.47,48 While our study focused on LAGC, based on the published literature we can extrapolate that immunotherapy likely will not achieve cost-effectiveness in this subset of patients until costs of immunotherapy agents are dramatically reduced. 47 Furthermore, this assumption relies on the success of active clinical trials designed to demonstrate the efficacy of immunotherapy in patients with LAGC, which has yet to be established.49,50 Finally, immune checkpoint inhibitors are currently only recommended for the treatment of patients with microsatellite instability-high or mismatch repair-deficient tumors by the NCCN guidelines and further work is essential to assess the cost-effectiveness for these specific patients. 9
Our decision tree should not be generalized to each and every patient. Some patients with GC may be more radiosensitive than others. There have been studies demonstrating if radiosensitive patients receive adjuvant radiation therapy, they have a reduced rate of disease progression; US may be more cost-effective than PCT in these patients. 51 Our study compared only PCT and US as these modalities have the highest LOE per the NCCN Guidelines for treatment of LAGC and are most commonly utilized in the United States. Furthermore, due to the narrow difference in QALYs between both arms, minor differences in assumptions used to calculate utility weights could potentially change the outcome of this study. Current morbidity and mortality data on types of gastrectomies including partial, subtotal, and total gastrectomy as well as current data comparing D1 and D2 lymph node dissection would be essential in future analyses. If this data were available, it could aid in the stratification of patients for whom US may be more cost-effective than PCT especially when considering the stage and the location of the primary GC. Additionally, studies reporting on the usage of immunotherapy in LAGC are currently underway and results are pending. Publication of these clinical trials may also alter the therapeutic landscape.
Conclusion
In this decision analysis comparing cost-effectiveness of PCT vs US for patients with LAGC, PCT is the more cost-effective treatment strategy. US portends a nearly equivalent QALY value but at an increased cost above the WTP threshold. The publication of current and new studies reporting on US is essential to better compare these 2 management modalities.
Footnotes
Author Contributions
All authors contributed to the conception and design, acquisition of data, analysis and interpretation of data, editing, and final approval. VP, PLQ, and SA contributed to the drafting of the article. The critical revision of the article was performed by SL, JBO, OM, MJ, KH, and RJC.
Author’s Note
This work was accepted as an abstract at the 2023 ASCO Annual Meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.