
Abstract

Choledocholithiasis is increasing in incidence in the pediatric population. 1 The management of choledocholithiasis in this population can be challenging due to the lack of clear consensus regarding the optimal therapeutic approach, the relatively low incidence of biliary disease, and available resources for the pediatric population. 1 Many institutions lack pediatric gastroenterologists, and the majority of therapeutic endoscopic procedures rely on adult gastroenterologists. This may limit timely intervention for the pediatric population. 2 Currently, the predominant treatment for choledocholithiasis involves a two-stage intervention, consisting of endoscopic retrograde cholangiopancreatography (ERCP) followed by laparoscopic cholecystectomy (LC). An alternative single-stage pathway has been described and practiced since the 1990s, which consists of LC with intraoperative cholangiogram (IOC) and laparoscopic common bile duct exploration (LCBDE). 3 The success of LCBDE has been well-documented in the adult population, with randomized controlled trials demonstrating comparable stone clearance rates and acceptable safety profiles.1,4 Adopting a single-stage, surgery-first approach could reduce the number of interventions and anesthetic events and lead to shorter inpatient stays.3,4 We aimed to identify missed opportunities for single-stage intervention by retrospectively examining the endoscopic findings of those who underwent an ERCP-first approach. We hypothesized that most patients undergoing preoperative ERCP had biliary obstructions that could have been cleared by basic LCBDE maneuvers, specifically, those patients presenting with sludge, small or medium stones, and even patients with a negative ERCP. We predicted that only a small portion of patients would have large stones or findings that would require more advanced LCBDE techniques.
This study was approved by the Institutional Review Board at our institution. We screened 26 children who underwent preoperative ERCP from 2018 to 2022. Inclusion criteria included age ≤18 years old and suspected diagnosis of biliary obstruction with performance of preoperative ERCP prior to LC by pediatric surgery. Exclusion criteria included failed ERCP and diagnosis of cholangitis. One patient was excluded due to failed ERCP and requiring an additional ERCP intra-operatively at the time of LC. In total, 25 patients were included. The diagnosis of suspected choledocholithiasis was based on biochemical markers, clinical presentation, and imaging findings concerning biliary obstruction. A retrospective chart review was conducted for baseline characteristics, hospital course, laboratory tests, and endoscopic findings as reported on ERCP. Stone size was classified according to the American Society for Gastroenterology: small (0-4 mm), medium (5-7 mm), and large (≥8 mm). In cases of multiple stones, the largest stone size was used for classification. Two patients were excluded from length of stay (LOS) calculation as they had outpatient ERCPs. Baseline characteristics and experimental data were summarized using median and IQR for continuous variables and percentages for summarizing categorical variables.
Baseline characteristics of patients included 19 females and 6 males with a median (IQR) age of 16 (14-16.8) years old and body mass index (BMI) of 28.74 (22.4-31) kg/m2. The median (IQR) length of stay was 89.3 (74.1-138) hours and the median (IQR) time from admission to ERCP was 23.4 (16.1-34.0) hours. Two patients were not included in the LOS and time from admission calculation as the ERCPs were performed outpatient. Seventy-six percent (n = 19) of patients had choledocholithiasis without cholecystitis. Gallstone pancreatitis was noted in 16% (n = 4) of patients, and choledocholithiasis with cholecystitis in 8% (n = 2) of patients. For imaging, 96% of patients underwent US (n = 24), 12% underwent computed tomography (CT) (n = 3), and 24% (n = 6) MRCP. Seven patients underwent multiple imaging modalities.
Endoscopic Findings.
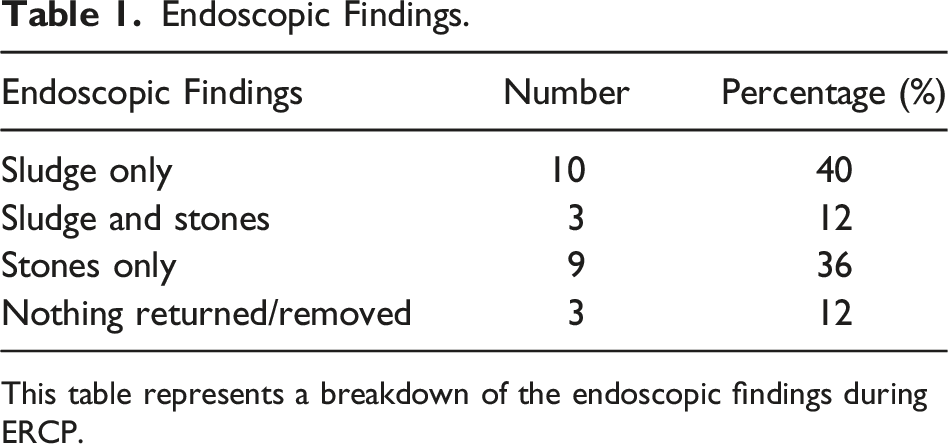
This table represents a breakdown of the endoscopic findings during ERCP.
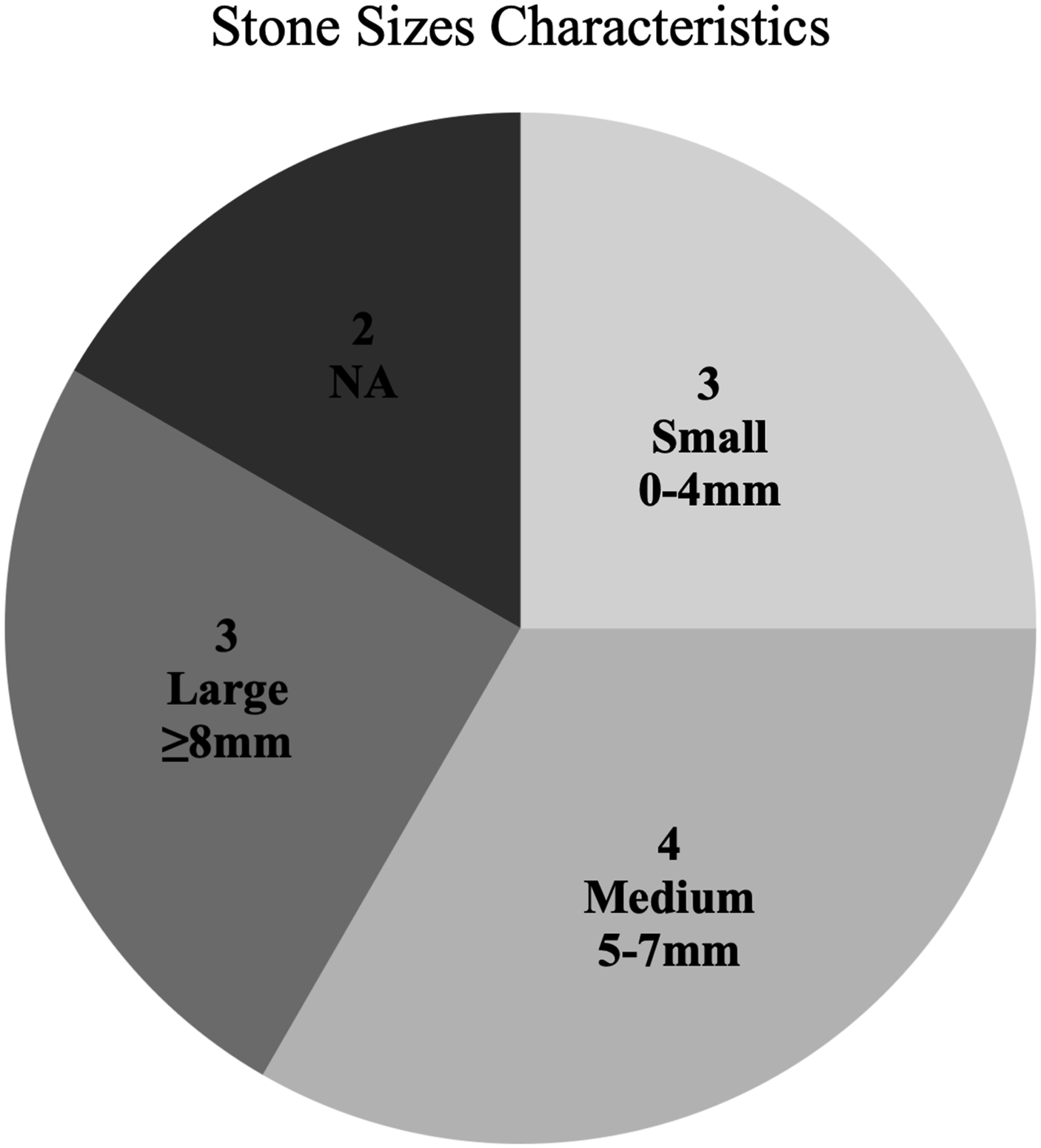
Stone size distribution based on stone findings. NA corresponds to stones that are unable to be characterized.
Our study suggests that the majority of pediatric patients undergoing preoperative ERCP in the management of choledocholithiasis have endoscopic findings that can be treated with LCBDE as the preferred treatment modality. Specifically, 80% of children had findings of small- or medium-sized stones, sludge, or no stones. Within this group, almost 70% of patients had findings that were likely to resolve with LC + IOC with power flushing or glucagon. Although 20% of patients had larger stones that may require more advanced LCBDE approaches such as transductal or lithotripsy, this represents a small portion of the pediatric patients in this study.
The optimal management strategy of choledocholithiasis remains a controversial topic, especially in the pediatric population.1,2 The chosen treatment pathway can vary based on health care providers, medical systems, expertise, and comfort in endoscopic or laparoscopic techniques, as well as general recommendations and referral patterns.1,2 When performed as a single-stage procedure, LCBDE is not only associated with fewer interventions but also with shorter LOS and lower costs. 1 Consistent with these studies, the median LOS in our study was 89.3 hours. The difference in LOS between single-stage and two-stage interventions is likely related to the inherent latency between multiple anesthetic events required for the diagnosis and treatment of those pediatric patients who undergo the two-stage pathway. LCBDE offers the advantage of being a diagnostic and therapeutic procedure that can minimize unnecessary radiologic and laboratory tests in this patient population.
The stone sizes successfully cleared in the LCBDE literature are variable. The majority of patients in our study had stones smaller than 8 mm, supporting our hypothesis that most patients undergoing ERCP had findings that can be cleared via basic transcystic LCBDE maneuvers. This highlights the importance of characterizing CBD stone sizes to determine the effectiveness of LCBDE and identify those who will likely have successful ductal clearance via the single-stage approach. In this study, 70% of the patients undergoing preoperative ERCP fell into the category of minimal interventions, where LC + IOC alone, along with adjuncts including power flushing or glucagon administration, may be sufficient treatment. This reinforces the concept that a surgery-first approach can help avoid unnecessary procedures and should be considered as a suitable first-line approach. This study has several limitations. First, this is a retrospective study with a relatively small sample size. Factors such as ductal tortuosity, ductal diameter related to the child’s age, and stone number are not specifically evaluated in this study. Future studies will include a multi-center analysis of pediatric patients with choledocholithiasis.
Our findings suggest that most children who received preoperative ERCP for suspected choledocholithiasis had findings amenable to simple LCBDE techniques. These findings included small stones, medium stones, sludge, or negative ERCP. Therefore, implementing a surgery-first approach for suspected choledocholithiasis can offer an efficient alternative to more common practices. Ultimately, the adoption of this approach has the potential to reduce health care costs and improve patient care.
Footnotes
Authors’ Note
Presented at SESC 2023, Savannah, Georgia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.