
Abstract
Fragility hip fractures result from low energy mechanisms and are associated with morbidity and mortality, especially in the elderly. We examined outcomes 2 years before and after implementation of a fragility fracture program. The pathway involves emergency department clearance and admission by a medical service with orthopedic consultation. Demographics include age, gender, fracture location, injury severity score (ISS), and ASA. Outcomes include DVT/PE, mortality, disposition, non-operative rate, ICU admission, time to surgery (TTS), length of stay (LOS), and admission service. 777 patients were included (383 PRE/394 POS). POS patients were slightly younger. Trauma admission decreased and LOS and TTS increased. There were no other demographic or outcome differences. Although TTS increased, it remained under 48 hours. Length of stay increase was possibly a reflection of COVID-19. Decreased trauma admission demonstrates pathway adherence. Further studies need to be conducted to verify that quality care can be maintained after initiation of a hip fragility pathway.
Fragility fractures are the result of a fall from standing height or lower, occur most often in the elderly, and are associated with significant mortality, morbidity, and reduced health-related quality of life. 1 Hip fractures are among the most severe of these fragility fractures and are associated with a high treatment cost and decline in health-related quality of life. The absolute mortality in the first year following a hip fragility fracture is 21.5% in females (age 66+) and 32.3% in males (age 66+). 2 As the population ages, it is expected that the number of patients with fragility fractures will increase to total 500 000-840 000 hip fractures in the United States by 2040. 3
Due to the medical complexity and multidisciplinary nature of these patients’ injuries and comorbidities, some programs have developed specific approaches that aim to improve quality and efficiency. There is evidence that specialized clinical pathways for fragility hip fractures can improve health-related quality of life and physical function in short and long term when compared to usual care. 1 Multiple models are utilized in the United States in treatment of fragility hip fractures. The traditional approach involves patient arrival to the ED, admission, surgical clearance by a medical physician, and operation and postoperative instructions and management from the orthopedic surgeon. It has been shown that multiple strategies and variations of this decrease time to surgery and improve clinical metrics. 4
In the academic level 1 trauma center in this study, a fragility pathway (Figure 1) for patients with hip fractures was implemented in July 2021 with an aim to provide more efficient and effective treatment with hospitalist managed care. In this pathway, patients arriving with fragility fractures are evaluated by trauma surgery and if other injuries are found, the patient is admitted with orthopedics consultation if needed. If no other injuries are found, the patient is admitted to hospitalist services and trauma is available if needed. For the elderly and those with multiple comorbidities, hospitalists will evaluate the patient prior to surgery. If young or with few comorbidities, orthopedics will directly admit, operate, and transfer the attending service to hospitalists after surgery vs at discharge. Post-operatively, the patient is managed by hospitalist service with orthopedics following for a minimum of 2 days to remain available. The hospital osteoporosis clinic provides follow-up care to help prevent future fractures. This study compares clinical outcomes in hip fracture patients treated before and after implementation of this fragility pathway. Hip fragility fracture pathway.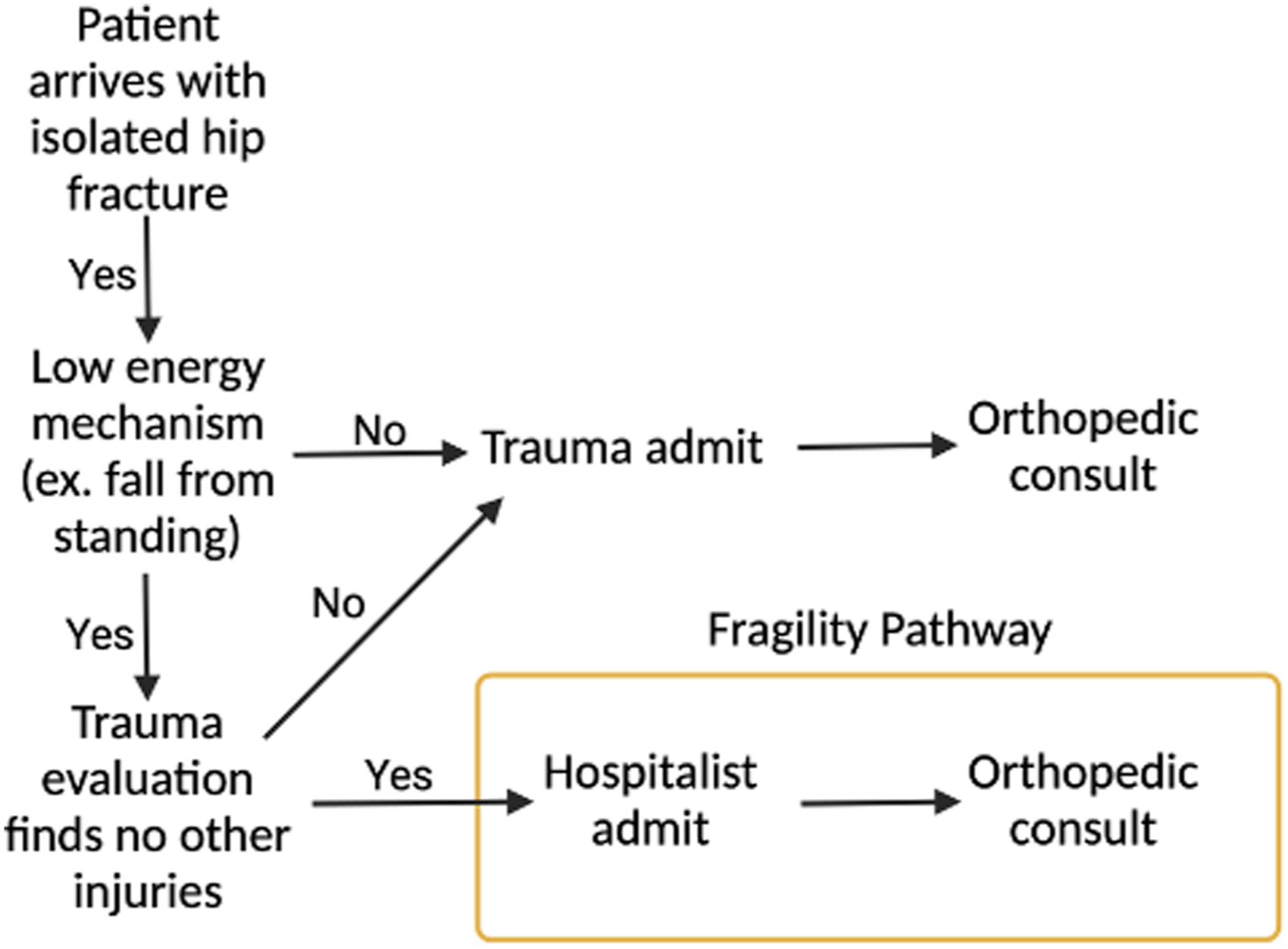
The study included all patients 55 and older, from 2 years before the pathway (PRE) (June 30, 2019-June 30, 2021) and approximately 2 years after (POS) (July 1, 2021-May 1, 2023), with a hip fragility fracture. Intertrochanteric, subtrochanteric, femoral neck, and periprosthetic fractures with a mechanism of injury limited to falls from standing height or less were included. Acetabular and pathologic fractures as well as those resulting from high energy mechanisms were excluded.
The outcome measures included deep venous thrombosis, pulmonary embolus, hospital mortality, 30-day mortality, disposition to hospice, non-operative rate, unplanned ICU admission, time to surgery, and length of stay. Admitting service was also recorded. Cohort demographics (age, sex, comorbidities defined by the American Society of Anesthesia Score (ASA), etc.) were compared to ensure that groups are similar, and outcomes were measured using chi-squared analysis or Fisher’s exact test for categorical variables and unpaired t test or Mann-Whitney U for continuous variables (depending upon needing statistical assumptions of normality and homogeneity of variance). For categorical variables if a significant effect is detected, unadjusted odds ratios with 95% confidence intervals were calculated. Means and standard deviations (parametric) or medians and interquartile ranges (non-parametric) were reported and interpreted for continuous values. Frequencies and percentages were reported and interpreted for categorical outcomes. Multivariate analysis for mortality was performed using logistic regression to yield adjusted odds ratios with 95% confidence intervals. Multiple and/or Poisson’s regression was performed on the continuous outcomes of time to surgery and length of stay. Unstandardized beta coefficients, their respective standard errors, and standardized beta coefficients were reported, along with the F-test associated with increased variance. All analyses were performed using SPSS version 29 and statistical significance was assumed at an alpha value of .05. Limitations include the COVID-19 pandemic which affected both patient cohorts and likely had an impact on multiple measures.
There were 777 patients in the study—383 PRE and 394 POS. Trauma was the admitting service of 3.4% of PRE patients and 96.1% were admitted by hospitalist services. In the POS cohort, trauma was not the admitting service for any patients, hospitalists admitted 98.8%, and orthopedics admitted 1.0%.
POS patients had a slightly lower median age (P = .12, PRE: 80.0 and POS: 77.5), but all other demographics were not significantly different. There was a significant difference in the admitting service as trauma dropped from 3.4% in the PRE cohort to 0% in the POS cohort. No significant differences were observed in rate of DVT/PE, hospital mortality, 30-day mortality, disposition to hospice, non-operative rate, or unplanned ICU admission. Hospital length of stay increased (P = .001, median PRE: 117 hours and POS: 128 hours) as did time to surgery (P < .001, median PRE: 15 hours 52 minutes and POS: 19 hours 13 minutes) (Figure 2). Patient outcomes PRE vs POS.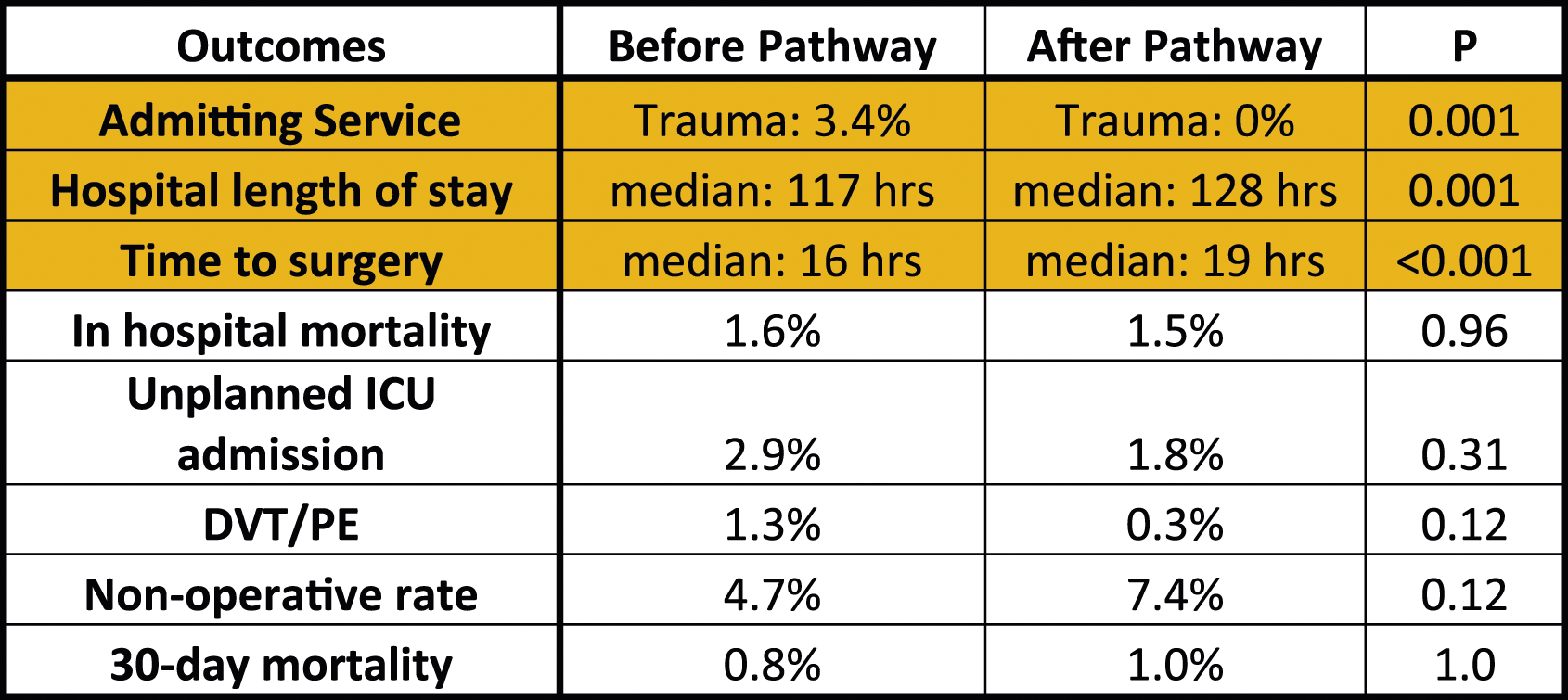
In this study, it is shown that implementation of a hip fragility pathway did not affect mortality or morbidity but was found to be associated with increased time to surgery and hospital length of stay. Although the time to surgery did increase, it remained under the American Academy of Orthopaedic Surgery 48-hour recommendations that is well-accepted best practice. This effect may reflect COVID-19 which likely had a greater impact on the POS cohort or could be the result of other unmeasured factors. There was a significant drop in trauma as the admitting service from 3.4% to 0%, demonstrating adherence to the fragility pathway protocols. This is important as the goal of the fragility pathway is to get hip fragility fracture patients in the care of hospitalists to enable treatment of complex morbidities. Despite the change in patient management, no changes were found in mortality or morbidity. Looking forward, there is more research to be done for hip fragility fracture pathways especially relating to influences on time to surgery and length of stay such as program acceptance and understanding as well as outside factors. Studies have shown that although there are many strategies for hip fragility fractures, the most effective technique is the use of evaluation metrics and iterative improvements to ensure that changes are quantified and are improved.4 With a better understanding of how best to design and implement these pathways, efficient and effective care can be better provided to this patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.