
Abstract
In cases of uncontrollable hepatic hemorrhage or acute hepatic failure after trauma, liver transplantation can be a lifesaving procedure. Traumatic tricuspid valve injuries are rare, and symptoms can range from indolent to acute right heart failure. When concomitant, traumatic liver transplant and tricuspid injuries have significant physiologic interplay and management implications. We present a 14-year-old male injured in an all-terrain vehicle accident, who sustained a devastating disruption of the common bile duct and celiac artery injury, leading to acute hepatic failure, necessitating a two-stage liver transplantation. He was subsequently found to have a severe traumatic tricuspid injury, which required tricuspid valve replacement. At 4 years post-injury, he is without major complications. This is the first case presentation of the cooccurrence of these complex pathologies. Importantly, we demonstrate the complex decision-making surrounding traumatic liver transplantation and timing of subsequent tricuspid valve repair, weighing the complex interplay of these 2 pathologies.
A 14-year-old male struck a tree with an all-terrain vehicle (ATV) at high speed. After impact, the ATV rolled over his chest and abdomen. He was transported to a local level 2 trauma center, where his exam was normal except for tire-shaped abrasions across his chest and abdomen, and diffuse ecchymosis across the lower back. CT scan of the chest, abdomen, and pelvis demonstrated grade V liver (Figure 1), grade III spleen, grade V right kidney, and grade III left kidney injuries. Due to his clinical stability, he was initially managed non-operatively. Over the next 5 days, he became febrile, was jaundiced, and had increasing abdominal pain and his total bilirubin increased to 4.7 mg/dL, prompting a HIDA scan which demonstrated a bile leak. Endoscopic retrograde cholangiopancreatography (ERCP), performed on post-trauma day (PTD) 7, showed contrast extravasation from the mid-common bile duct (CBD) and a biliary stent was placed. On PTD 8, the total bilirubin increased to 17.3 mg/dL. He was taken to the operating room (OR) for a diagnostic laparoscopy, where a complete transection of the CBD with the stent protruding from the injury and 6 liters of bile in the abdomen were identified. A Jackson-Pratt drain was placed, and he was transferred to the closest pediatric level 1 trauma center. Representative image from patient’s initial CT chest, abdomen, and pelvis, demonstrating extension of hepatic laceration to the inferior vena cava and right portal vein.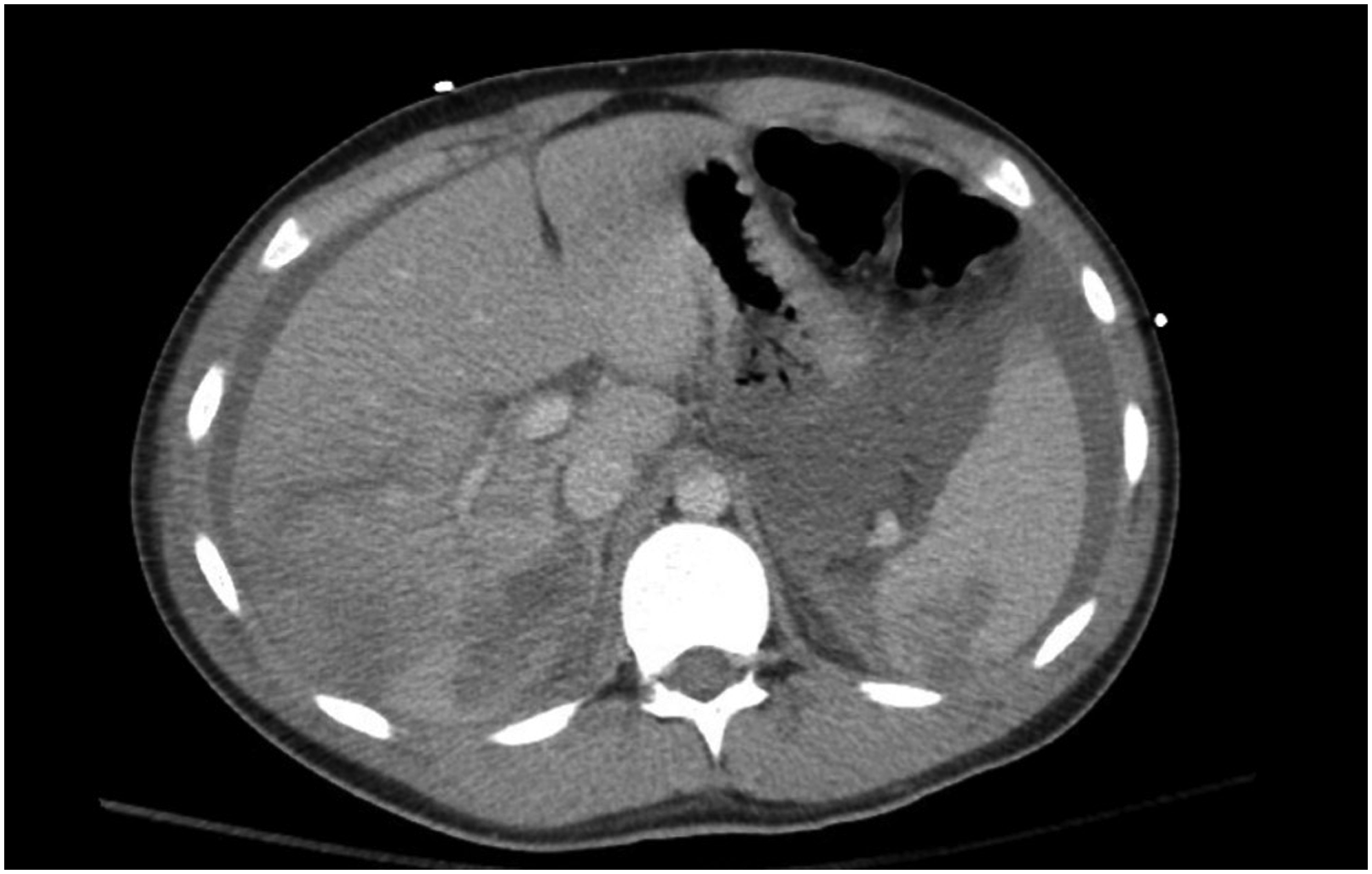
On arrival, he was jaundiced, tachycardic, and lethargic but arousable, with laboratory values notable for a while blood cell count of 45.1 × 109/L, total bilirubin of 15.4 mg/dL, alanine aminotransferase (ALT) 2415 u/L, aspartate aminotransferase (AST) 5343 u/L, lactate 9.5 mmol/L, international normalized ratio (INR) 2.5, and creatinine 2.46 µ/dL. He was promptly taken for a damage control laparotomy, redemonstrating the CBD transection. The stent was removed, the CBD was ligated, a drain was placed into the common hepatic duct, and a temporary abdominal closure was placed. On PTD 10, a CT angiogram of the abdomen revealed complete non-opacification of the celiac artery with minimal arterial blood flow extending into the branches of the celiac axis and the hepatic parenchyma. On PTD 11, he remained profoundly acidotic and coagulopathic, with increasing laboratory evidence of acute fulminant hepatic failure, so a total hepatectomy, splenectomy, and creation of an end-to-side portocaval shunt were performed, with status 1A listing for emergent liver transplantation. Immediately post-operation, he developed a junctional cardiac rhythm, with a rate of 60-70 beats per minute. In conjunction with the cardiology team, this was felt to be likely due to his hyperammonemic state, though blunt cardiac injury was considered. After an anhepatic period of 26 hours, he returned to the OR on PTD 12 for completion of a two-stage orthotopic liver transplant, with a choledochoduodenostomy reconstruction, due to the extent of biliary trauma. On PTD 17, a transthoracic echocardiogram (TTE), and subsequently transesophageal echocardiogram (TEE), was obtained due to ongoing junctional heart rhythm, development of a pleural effusion, and a slow venous ooze from his surgical incisions, which demonstrated severe tricuspid regurgitation, a flail tricuspid valve, disruption of the anterior leaflet chordae tendineae, and flow reversal in the IVC. Due to concern for tricuspid regurgitation leading to hepatic graft dysfunction, his cardiovascular status was promptly optimized with aggressive diuresis and preload reduction. With this, his hepatic graft demonstrated appropriate function despite ongoing tricuspid regurgitation, so repair of his tricuspid valve was delayed until PTD 57. In the OR, he was found to have a posterior tricuspid valve leaflet that was 50% avulsed from annulus, complete avulsion of the cortical and papillary support to posterior leaflet, and significant chordal and papillary muscle rupture of the anterior leaflet. Primary tricuspid valve repair was unsuccessful, so a 29 mm Edwards pericardial tissue valve was placed. On PTD 73, he was discharged home tolerating a regular diet and ongoing physical therapy. At the time of writing, 4 years after his injury, he has had no major complications, is actively participating in sports, and has returned to ATV riding.
The liver is the most frequently injured abdominal organ in pediatric blunt trauma, with 90% of injuries amenable to nonoperative management and the remainder of cases requiring embolization or operative management. 1 Rarely, cases involving significant vascular injury or acute hepatic failure may be uniquely managed by liver transplantation. First described in 1987 by Thomas Starzl, liver transplantation for trauma is rare, only described in case reports and small case series, with long-term survival rates ranging from 51% to 84%, with a patient age range of 4 to 68 years, though the exact number of pediatric cases performed to date is unknown. 2 Published indications for post-traumatic liver transplant have included hepatic hemorrhage, portal vein thrombosis, bile duct necrosis, and acute hepatic failure. Two techniques have been described for liver transplantation after traumatic injury: single- and two-stage transplantation. Single-stage liver transplant is the most common liver transplant operation overall, in which the diseased recipient liver is removed in the same operation as a healthy donor liver is placed. However, as in this case, with acute fulminant hepatic failure or extensive hepatic trauma, it may be necessary to perform a two-stage transplant, in which a total hepatectomy with creation of a portocaval anastomosis is performed, prior to listing the patient for emergent two-stage transplantation, followed by a second surgery for graft implantation if the patient survives. Up to 30% of patients will die during the anhepatic phase; however, anhepatic phases as long as 66 hours have been reported. Notably, this child ultimately survived a 26-hour anhepatic period and actually stabilized once his native liver was removed.
Further complicating this patient’s course, a significant tricuspid valve injury was identified after liver transplantation. Traumatic tricuspid injury is rare and its presentation can range from asymptomatic to acute right heart failure or hemodynamically significant arrhythmia, depending on the extent of myocardial contusion, valvular injury, and resultant incompetence. 3 Diagnosis of tricuspid valve injury is made with transthoracic, or ideally transesophageal, echocardiography with identification of tricuspid regurgitation and valvular incompetence. 3 Consistent with the notoriously indolent initial presentation of traumatic tricuspid valve injury, this child’s injury was not identified until PTD 17, when TTE and TEE demonstrated acute tricuspid valvular regurgitation, with evidence of flow reversal in the IVC. In retrospect, this child’s only initial symptom prior to liver transplant that could be attributed to tricuspid injury was new onset junctional heart rhythm on PTD 11, when a TTE with limited views failed to demonstrate tricuspid injury. Collectively, the indolent course, and delayed diagnosis, of this child’s tricuspid valve injury underscores the importance of maintaining a high index of suspicion for valvular injury after thoracic trauma, anytime cardiac dysfunction (new arrhythmia, edema, hemodynamic changes, etc) arises. Here, a foremost concern in the setting of recent liver transplant with concomitant tricuspid insufficiency was the potential repercussions of central venous hypertension on the health of the liver graft. In adults, there is data clearly suggesting that liver transplant graft viability and overall mortality are negatively impacted by ongoing tricuspid regurgitation. 4 Here, due to the extent of the tricuspid injury, there was preoperative concern that a valve prosthetic may be necessary. In the setting of recent bile leak, delayed abdominal closure, and post-transplant immunosuppression, the risk of systemic infection with a prosthetic valve was initially felt to be prohibitively high. Ultimately, the child was successfully managed medically with diuresis and blood pressure control for over 1 month before valvular replacement. During this time, there was importantly no evidence of consequent graft dysfunction and his potential risk for superimposed infection was able to be mitigated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.