
Abstract
Background
Video-assisted thoracoscopic surgery (VATS) is a practical resource in the management of traumatic hemothorax. However, it carries inherent risks and should be mobilized cost-effectively. In this study, we investigated the ideal VATS timing using cost analysis.
Methods
617 cases of unilateral traumatic hemothorax from 2012 to 2022 were identified in our trauma database. We extracted encounter cost, length of stay (LOS), and operative cost information. Using Kruskal-Walli’s test, we compared the cost and LOS for patients who underwent VATS or continued nonoperative management in the first 7 days of admission. Additionally, we computed the daily proportion of patients initially managed nonoperatively but ultimately underwent VATS. P-values <.05 were considered significant.
Results
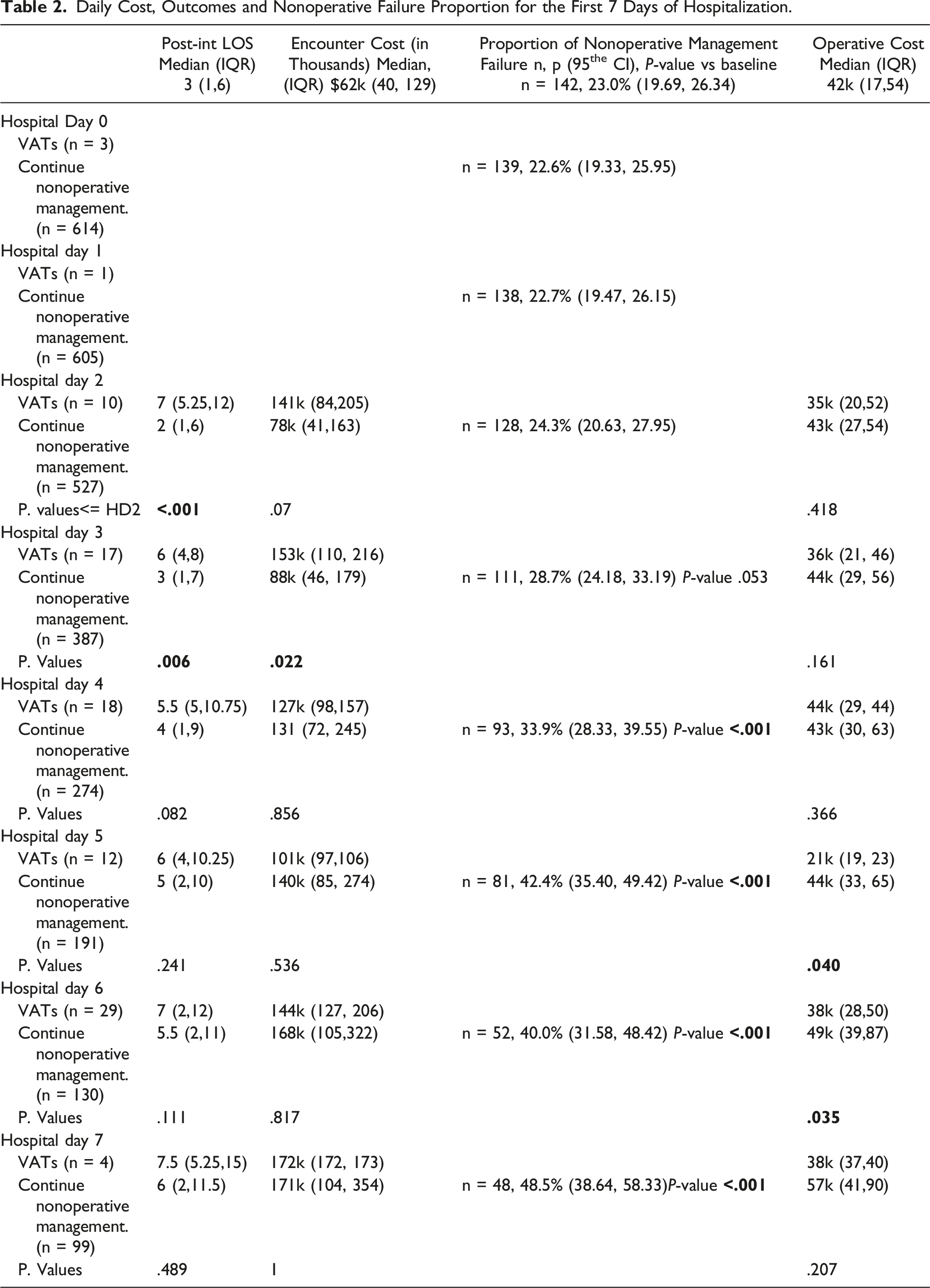
The median encounter cost of cases managed operatively before hospital day 4 (HD4) was higher than those managed nonoperatively. This difference was $63k on HD2 (P-value .07) and was statistically significant for HD3 (difference of $65k, P-value .02). The median LOS with operational management on HD2 and 3 was 7 and 6 respectively vs median LOS of 2 and 3 with nonoperative management on those days (P-value <.001, .01 respectively). The proportion of patients who failed nonoperative management did not change from baseline until HD4 (23% (95% CI 19.7, 26.3) vs 33.9% (95% CI 28.3, 39.6), P-value <.001).
Discussion
Early mobilization of VATS before hospital day 4 increases the overall hospital cost without offering any length of stay benefit. Continuing nonoperative management longer than 4 days is associated with a high failure rate and a costlier operation.
Keywords
Key Takeaways
• Tube thoracostomy is an effective tool for the management of traumatic hemothorax. • Based on the cost profile and outcomes of traumatic hemothorax patients managed definitively with tube thoracostomy, it should be the gold standard for the care of these patients. • To maximize the cost-effective mobilization of a valuable resource, VATS should be reserved for patients who retained hemothorax on hospital day 4 (or 3).
Introduction
Hemothorax 1 is one of the most common complications of thoracic trauma.1-3 Most cases of traumatic hemothorax can be treated with tube thoracotomy.4,5 However, surgical management is recommended to manage the retained blood products when it fails.1-5 The rationale for definitive management of retained hemothorax is to prevent further complications, including empyema and lung trapping.1-6 Most guidelines recommend Video-assisted thoracoscopic surgery (VATS) as the preferred intervention when tube thoracotomy fails, assuming that there are no contraindications to surgery or minimally invasive surgery.7-9 VATS is effective at evacuating the retained blood products and better tolerated than open thoracotomy.6-9 The quality of evidence comparing VATS to thrombolysis is more muddled. Thrombolysis may be cheaper than VATS, but only if additional interventions are not warranted. 10 Current guidelines recommend thrombolysis as an adjunct to care or for patients who are risk-prohibitive for surgery.8,11 Given VATS’s (contested) superiority as the subsequent line treatment for retained hemothorax, several efforts have been made to establish the optimal timing for performing VATS.7,8,12
Despite its role, VATS is a major thoracic surgery with inherent risks and should ideally be reserved for patients most likely to fail nonoperative management with tube thoracotomy. Additionally, while some efforts have been made to understand regional cost variations in managing hemothorax, 13 current guidelines6-8,11 do not account for operative cost, balanced against outcomes, when comparing different treatment strategies.
Prioritizing cost over quality of care in emergent or urgent contexts would be, to put it mildly, underhanded; nonetheless, the financial burden of care obtained by a stable patient continues to affect their life much after their recovery. Additionally, with the emergence of value-based care as the benchmark for care and reimbursement, it is imperative that we pay close attention to the financial implications of providing care for our patients. We aspire to rectify the lack of transparency regarding pricing information in the existing surgical literature through the implementation of this research. In order to address the matter of ideal VATS timing, we combined the cost-effectiveness of VATS with the results observed in patients who were treated with tube thoracotomy. In this study, retained hemothorax was defined as hemothorax that persisted after the insertion of a tube.
Methods
Study Setting
This was a retrospective review of cases of traumatic hemothorax that presented to the author’s hospital from 2012 to 2022. Author’s institution is a Level 1 trauma center verified by the American College of Surgeons. As the only Level 1 hospital in the author’s city metropolitan area, it has a wide catchment, including the Western and Central regions of authors’ state and neighboring state.
Study Population
Cases were defined as traumatic hemothorax that required at least tube thoracostomy. UofL Hospital has maintained a prospective database of all trauma patients since the 1900s. We queried the database based on the following criteria: (1) Live presentation and completed management of the traumatic hemothorax before discharge or death; (2) Cases with no prior thoracotomies preceding VATS during that encounter; and (3) Cases involving unilateral chest or bilateral chest with the same management for both sides including timing. Cases were further restricted based on the abbreviated injury severity score (AIS) and the injury severity score (ISS). Cases with injury AIS of 2 could have an ISS of at most 12. Cases with injury AIS of 3 could have an ISS of at most twenty-two, cases with injury AIS of 4 could have an ISS of at most twenty-five, and cases with an injury AIS of 5 could have an ISS of at most 26.
Variables
The trauma registry provided demographic data on age, sex, injury type, AIS, and ISS, as well as LOS, ICU LOS, ventilator dependency (vent days), VATS timing, and the incidence of unplanned ICU upgrading, unanticipated intubation, pneumonia, and empyema. For patients treated with tube thoracotomy alone, we checked their electronic medical record (EMR) for tube discontinuation timing. From the EMR, we also derived the financial identification number (FIN) to uniquely identify patients by encounter. Our financial department retrieved the VATS operative cost and cohort encounter cost after receiving the FIN. The pre- and post-intervention LOS was calculated by subtracting VATS or tube cessation from the LOS.
Statistical Analysis
We performed a survival analysis for patients with tube thoracostomy to establish an expected treatment course. Then, we split each definitive treatment group in 2 based on the median survival time identified from the survival analysis. We used Kruskal-Walli’s test, Dunn’s pairwise comparison with Holm’s adjustment method to analyze quantitative variables, and the Chi-square test to analyze categorical variables. Additionally, to examine complication trends, a contingency table was constructed with each of the 4 management groups in the row and the number of occurrences of each complication in the column. The odds of complication were computed relative to one of our tube thoracostomy groups. We also derived the daily nonoperative failure proportion. This was done by dividing the number of cases managed nonoperatively at the beginning of a given day that eventually required VATS with the total number of cases pending definitive management. Finally, for the first 7 days of hospitalization, the post-intervention LOS and encounter cost for patients who were operated on each day was compared to the encounter cost of continuing nonoperative management. Also, the operative cost for patients who underwent VATS daily was compared to the operative cost of later operations. Due to the relatively fewer operative cases on hospital days 0 and 1, the calculations for days 0 to 2 were combined and reported as <=HD2. The two-sided P-value for all statistical tests and the 95% confidence interval were reported. P-values <.05 were considered statistically significant.
Data was analyzed using R software including R commander (Fox J, Marquez MM, Bouchet-Valat M (2023). Rcmdr: R Commander. R package version 4.2.1, https://socialsciences.mcmaster.ca/jfox/Misc/Rcmdr/.), and R studio (R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/).
Ethical Considerations
This study received ethical approval from the Institutional Review Board (IRB) at UofL (IRB number 21.0584). This study was classified as a study exempt with an open-end date.
Results
1013 cases of traumatic hemothorax that required at least tube thoracostomy were identified. The following cases were excluded based on the inclusion criteria: 66 cases who presented dead or died shortly after arrival, 20 had thoracotomy before VATS, 7 died before definitive management of their hemothorax, and 13 had bilateral injuries. Additionally, 290 exceeded the AIS and ISS restrictions, and we also excluded them, leaving 617 cases for analysis. 475 (77%) were definitively managed with tube drainage alone; the rest required VATS.
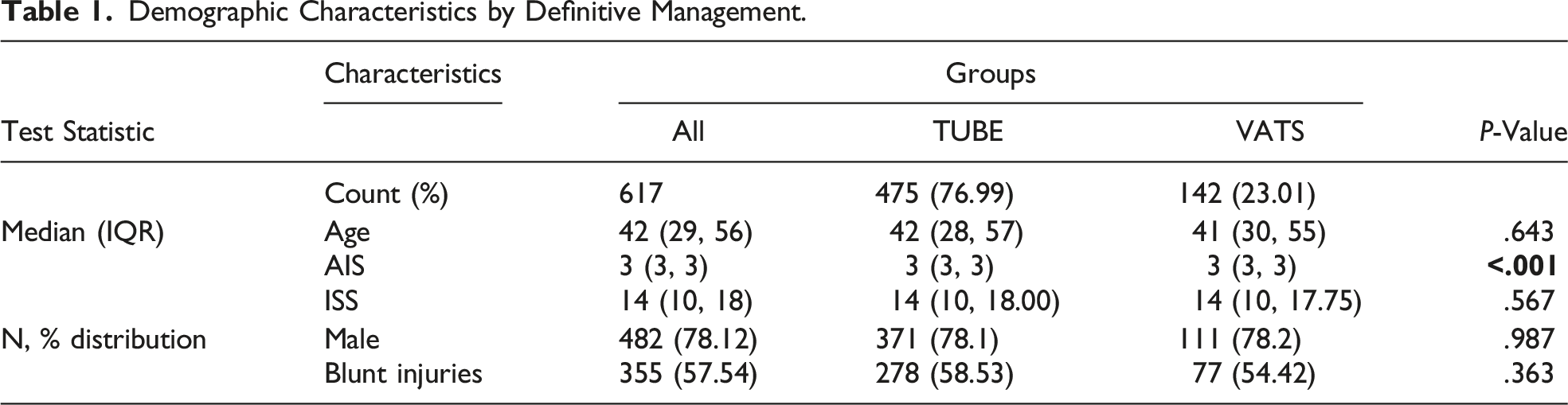
Demographic Characteristics by Definitive Management.
Survival Analysis, Four-Group Cost, and Outcome Analysis
The expected duration of tube management (ie, median survival time) for patients managed with tube alone was 4 days. The survival risk on hospital day 4 was .381 (Figure 1). Our management groups were each split in 2 based on the median survival time. 294 cases were managed with tube thoracotomy within 4 days (TUBE<=4) and 181 beyond 4 days (TUBE>4). Forty-nine cases were handled with VATS within 4 days (VATS<=4) and 93 beyond 4 days (VATS>4). Survival curve for patients managed with tube thoracostomy alone. Figure 1 depicts the survival curve for patients managed with tube thoracostomy alone. The median survival time, hospital day 4, is bolded for emphasis. The survival risk on hospital day 4, .38, is also bold in the table below and traced on the figure.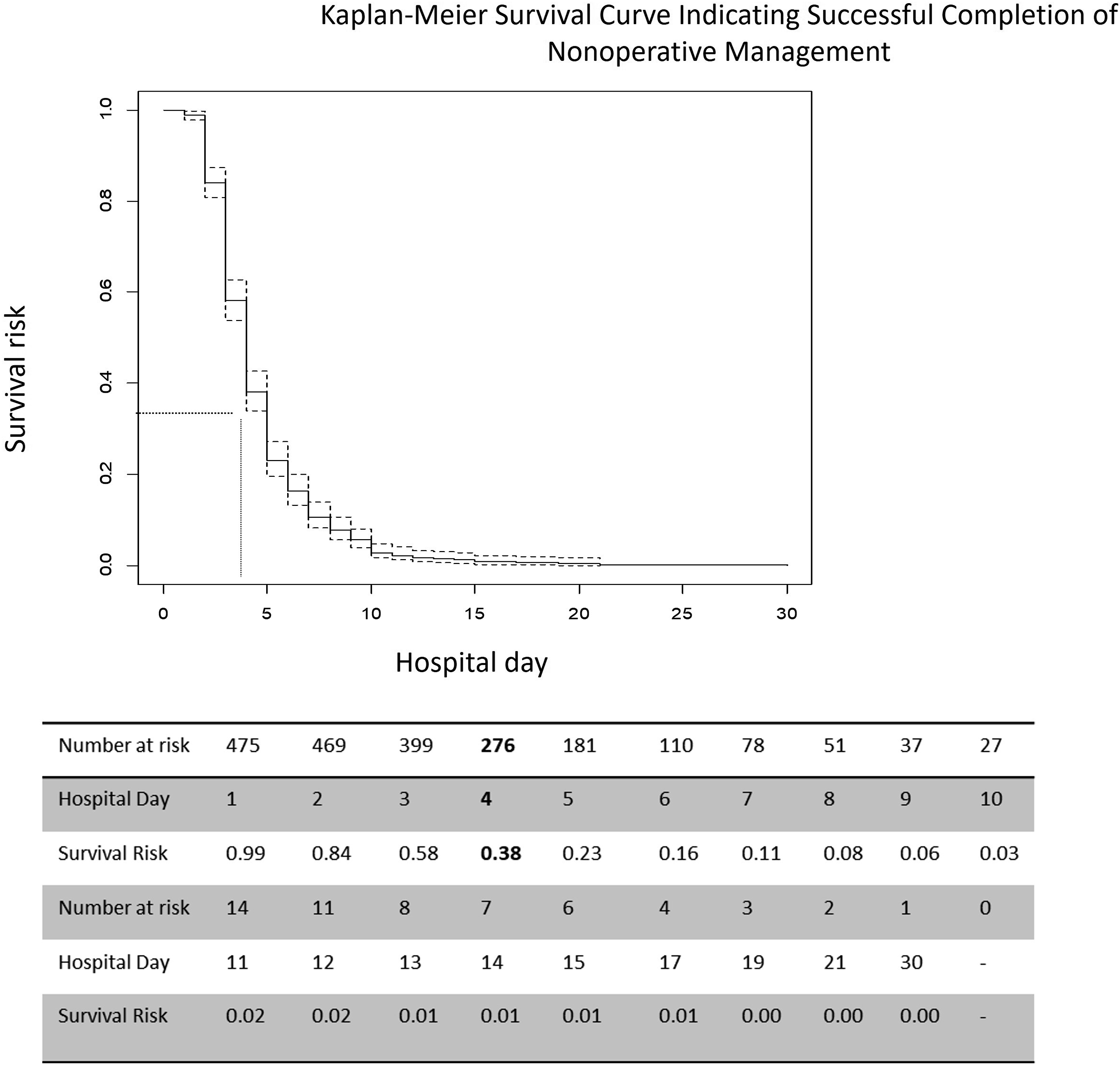
Details results are included in Supplemental Table/Figure 1. LOS was shortest for the TUBE<=4 group and longest for the VATS>4 groups (median 4 vs 15 days IQR 3 vs 11, P-value <.001). The LOS was equivalent for the TUBE>4 and the VATS<=4 management groups (LOS 10 vs 9, IQR 7, respectively). The median ICU LOS and IQR for the 4 groups TUBE<=4, VATS <=4, TUBE>4, and VATS >4 were 0 (2), 1 (4), 3 (6), and 3 (8), respectively. There was no difference in ICU LOS between the TUBE>4 and VATS<= groups and between the TUBE>4 AND VATS>4 groups. The differences in ICU LOS between the other pairs were significant. Compared to the TUBE<=4 group (median day 0, IQR 1), the groups that were managed after hospital day 4 had more prolonged ventilator dependency (TUBE>4 median days 6, IQR 3; VATS >4 median day zero IQR 3, P-values <.001, respectively.
The median Pre-int LOS and IQR for the 4 groups TUBE<=4, VATS <=4, TUBE>4, and VATS >4 were 3 (2), 6 (3), 3(2), and 8 (4), respectively. The median Post-int LOS and IQR for the 4 groups TUBE<=4, VATS <=4, TUBE>4, and VATS >4 were 1 (4), 2 (5), 7 (6), and 5 (5), respectively. There was no difference in time to definitive management for the TUBE<=4 and VATS<=4 groups. However, the post-management LOS was longer for the VATS<=4 group compared to the TUBE<=4 group (P-value <.001). Similarly, there was no difference in time to definitive management for the TUBE>4 and VATS>4 groups, but the TUBE>4 group had a shorter post-management LOS compared to the VATS>4 group (P-value <.001).
Regarding complications among our 4 groups, the odds of pneumonia after hospital day 4 in the VATS<= 4 group was 11.24 times higher than the odds of pneumonia in the TUBE <=4 group (95%CI (2.59, 48.73, P-value .002). There was no statistical difference in the strength of the association of unplanned ICU upgrades, unplanned intubations, or empyema between those 2 groups. Supplemental Table 2 contains detailed results comparing the odds of each complication between the TUBE <=4 groups and the TUBE > 4 and VATS >4 groups.
Daily Management Decision, Cost, and Outcome Analysis
Twenty-three percent of cases initially managed with tube thoracotomy failed nonoperative management (P-value, <.001, 95% CI 19.69, 26.34). Starting from hospital day 4, the nonoperative failure proportion increased dramatically and differed from the baseline proportion (33.9% vs 23.0%, P-value <.001, Figure 2). This trend continued, peaking on hospital day thirteen when we observed a nonoperative failure proportion of 58.5% (vs 23.0% P-value .002). Daily conversation to operative management. Figure 2 illustrates the daily nonoperative failure proportion over time in our study. “Nonoperative failure proportion” was defined as the proportion of patients who started each day with nonoperative management but later required VATS. The failure proportion of .339 on hospital day 4 was the first statistically significant increase from the baseline failure proportion of .23.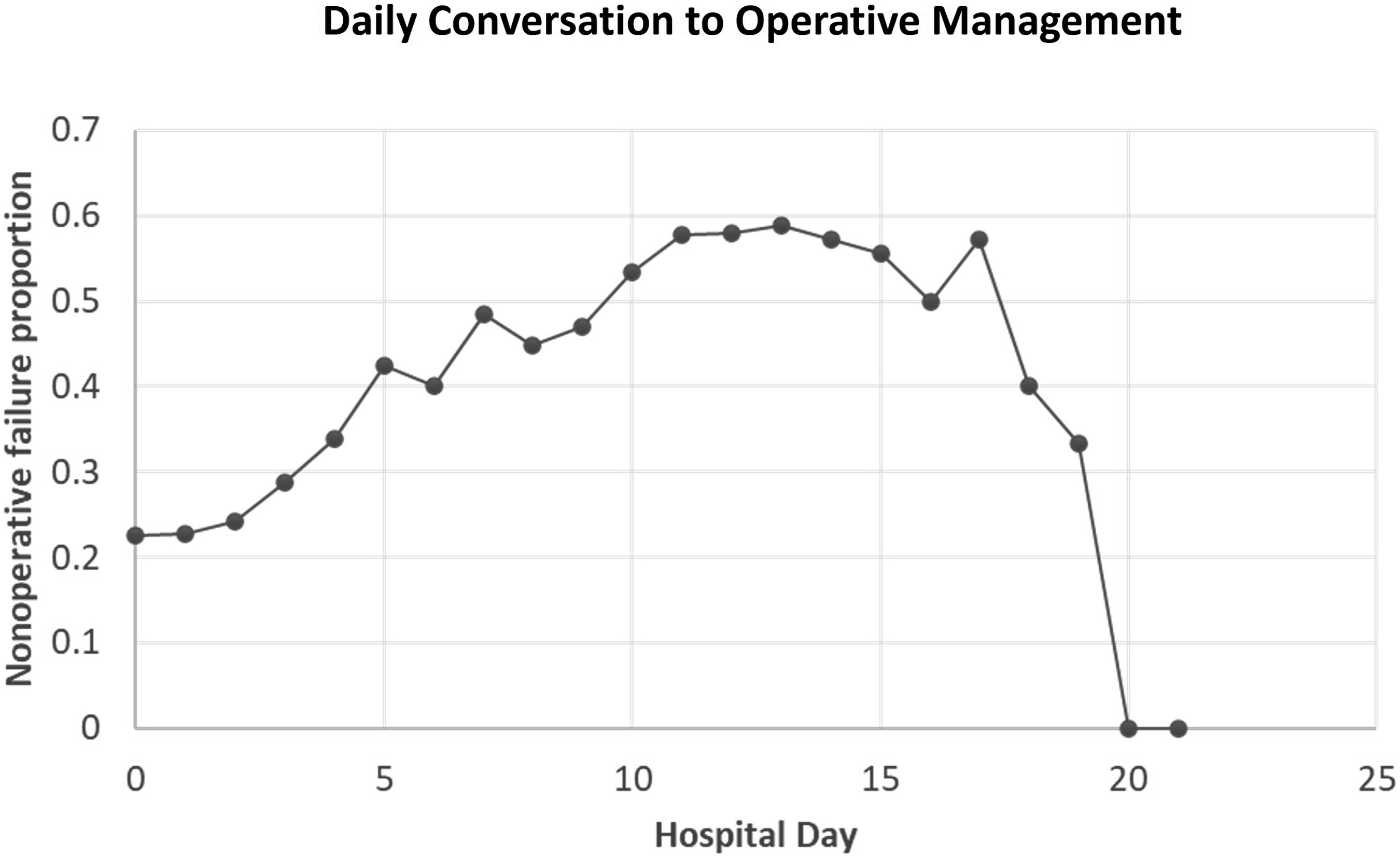
Daily Cost, Outcomes and Nonoperative Failure Proportion for the First 7 Days of Hospitalization.
Discussion
In summary, by restricting the AIS/ISS, we selectively analyzed the cost and outcome of patients primarily admitted for the management of traumatic hemothorax. Age, sex, and injury severity were similar in TUBE and VATS management groups. Chest tubes were typically removed on hospital day 4 for our population. The survival risk for hospital day 4 was .381, implying 61.9% of chest tubes had been removed. We next evaluated cost and results for 4 patient groups: those who had the tube terminated after the median survival time and those who received VATS within similar timeframes. Patients contained with VATS within 4 days had a longer ICU LOS, longer post-intervention LOS, and greater chances of pneumonia even after definitive tube management. VATS before hospital day 4 had greater encounter costs than nonoperative management. In the 4 days of hospitalization, nonoperative care was better than VATS for early discharge and reducing unexpected ICU upgrades, intubations, empyema, and pneumonia. From hospital day 4, 1 in 3 patients failed nonoperative care and needed VATS, which became more expensive from day 5 (Table 2). Patients who received earlier final management had a shorter LOS than those who had VATS after hospital day 4 (Supplemental Table 1). Interestingly, VATS within 4 days had no LOS advantage over tube management beyond 4 days. Due to the high nonoperative failure rate and higher complication risk, further management should be avoided.
These findings suggest tube drainage alone is the best treatment. When it lasted longer than hospital day 4, tube drainage’s cost and LOS advantages declined. Operating using VATS within 4 days is a sensible compromise to reduce the risk of complications and high cost of a later procedure. But this has 2 issues. First, VATS in 4 days costs much more than tube management. Second, 2 management choices are proposed simultaneously. To maximize tube drainage and speed up surgery, patients without an urgent or emergency need for operational care should be allowed up to 3 days of tube drainage and operated on hospital day 4.
Current guidelines advocate for VATS within 3 or 4 days based on the outcomes between late and early VATS.8,10 Our study first approaches the issue of timing based on the expected course of patients managed with tube thoracostomy. Then, after analyzing the cost of care delivered and outcomes, we conclude that VATS earlier than hospital day 3 is expensive, without offering any LOS benefit. Those patients had longer post-intervention LOS than those who continued nonoperative management in the first 3 days of hospitalization. We attribute this surprising finding to surgery recovery time as the 2 early management groups had similar ages, AIS, and ISS (Supplemental Figure 2/Table 3). Additionally, the success rate of nonoperatively managed within the first 3 days is high enough to necessitate a more cautious mobilization of VATS resources.
Primary traumatic hemothorax was the admitting diagnosis in our study. In patients with more severe injuries who are likely to stay more than 4 days in the hospital, our earlier recommendations are even more important. Since their stay is not driven by controlling their traumatic hemothorax, earlier VATS may raise costs without LOS benefit. When health care costs are rising without population health improving, it’s wise to closely review our patients’ care costs. Guidelines speed up care. 13 As value-based care becomes more common, surgical research must consider operational cost while creating and amending guidelines. Cost analysis can be used in selective trauma patient decision-making, according to this study. Our cost integration recommendation is clinically justified and reduces patient costs for specialist care.
Patients with severe injuries should interpret this study’s injury severity score-based eligibility cautiously. Patients who presented earlier than 2016 had missing cost data. Administrative mistakes prevented some patients from receiving cost data. The approach handled missing data via paired deletion, however incomplete data may have contributed to the null result in the cost analysis of hospital day 2 patients (Table 1), despite a “common sense” difference in median cost between surgical and nonoperative patients. As single-institution research in the author’s region, the cost of managing traumatic hemothorax may vary by geography and operational style. 14
Supplemental Material
Supplemental Material - Not So Vats: How Early Is Too Early In The Operative Management Of Patients With Traumatic Hemothorax?
Supplemental Material for Not So Vats: How Early Is Too Early In The Operative Management Of Patients With Traumatic Hemothorax? by Chinweotuto V. Uma, William B. Risinger, Suhail Nath, Samuel J. Pera, and Jason W. Smith in The American Surgeon
Supplemental Material
Supplemental Material - Not So Vats: How Early Is Too Early In The Operative Management Of Patients With Traumatic Hemothorax?
Supplemental Material for Not So Vats: How Early Is Too Early In The Operative Management Of Patients With Traumatic Hemothorax? by Chinweotuto V. Uma, William B. Risinger, Suhail Nath, Samuel J. Pera, and Jason W. Smith in The American Surgeon
Supplemental Material
Supplemental Material - Not So Vats: How Early Is Too Early In The Operative Management Of Patients With Traumatic Hemothorax?
Supplemental Material for Not So Vats: How Early Is Too Early In The Operative Management Of Patients With Traumatic Hemothorax? by Chinweotuto V. Uma, William B. Risinger, Suhail Nath, Samuel J. Pera, and Jason W. Smith in The American Surgeon
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.