
Abstract
Background
Alcohol use is frequent in trauma patients and alcohol withdrawal syndrome (AWS) is associated with significant morbidity. Benzodiazepines are commonly used for AWS, but may cause neurologic and respiratory adverse events (AEs). The objective was to evaluate the effectiveness and safety of a phenobarbital-based protocol for the treatment of AWS in non-intensive care unit (ICU) trauma patients.
Methods
Adult non-ICU trauma patients at high risk of or experiencing AWS PRE and POST implementation of a phenobarbital-based protocol were included. Outcomes were AWS-related complications (AWS-RC), benzodiazepine use, adjunctive medication use, hospital length of stay (HLOS), and medication-related AEs. Subgroup analyses were performed on patients with traumatic brain injury (TBI), rib fractures, and at high risk of severe AWS.
Results
Overall, 110 patients were included (51 PRE, 59 POST). AWS-RC developed in 17 PRE patients compared to 10 POST patients (33% vs 17%; P = .05). PRE patients were more likely to receive benzodiazepines (88% vs 42%, P < .0001) and higher total dose (11 vs 4 mg lorazepam equivalent; P = .001). No difference noted in HLOS (8 vs 8 days, P = .27), adjunctive medication use (49% vs 54%, P = .60), or AEs (57% vs 39%, P = .06). There was no difference in AWS-RC in the TBI subgroup (P = .19), less AEs in the rib fracture POST subgroup (P = .04), and less AWS-RC in the high risk of severe AWS POST subgroup (P = .03).
Discussion
A phenobarbital-based protocol in trauma patients is effective in preventing AWS-RC and decreasing benzodiazepine use without increasing AEs.
Key Takeaways
• A phenobarbital-based AWS protocol in non-intensive care adult trauma patients was effective in preventing AWS-related complications and decreasing benzodiazepine utilization. • The use of a phenobarbital-based AWS protocol did not increase the risk of medication-related adverse effects, including neurologic or respiratory depression.
Introduction
Alcohol use is associated with up to 30% of visits to US level I trauma centers. Positive admission ethanol tests are present in as many as 70% of trauma patients, 30% meet criteria for alcohol use disorder, and roughly 1% develop alcohol withdrawal syndrome (AWS).1,2 Although AWS is not associated with an increase in mortality, AWS in trauma patients has been associated with prolonged lengths of stay (LOS) and increased complications.1,3,4 One study reported delirium tremens in 11% of trauma patients with AWS and was associated with increased mortality. 3
Symptom-triggered therapy (STT) with benzodiazepines based on Clinical Institute Withdrawal Assessment for Alcohol-revised (CIWA-Ar) scoring is commonly utilized for the treatment of AWS. Benzodiazepine therapy has consistently demonstrated reduction in seizures, 5 but high dose benzodiazepines are associated with serious adverse events (AEs) such as delirium, central nervous system (CNS) depression, and respiratory depression. 6 The reliability of CIWA-Ar in hospitalized patients has been questioned, with studies reporting inappropriate utilization of CIWA-Ar in up to 50% of hospitalized patients.7,8 Recent guidelines recommend prophylaxis in patients at risk of developing severe or complicated AWS with either benzodiazepines or phenobarbital.9–11 While no validated tool has been established in the trauma population to determine AWS severity risk, the limitations of the CIWA-Ar and recent benzodiazepine shortages, have increased interest in the use of phenobarbital for prophylaxis and treatment of AWS. 11 A risk-stratified phenobarbital-based alcohol withdrawal protocol was evaluated in a medically ill population. 12 Although phenobarbital-treated patients were more likely to be at risk of severe AWS, there was no difference in AWS-related complications, intensive care unit (ICU) admissions, LOS, or AEs noted when compared to a fixed-dose regimen of benzodiazepines. 11 Additional studies have shown that phenobarbital use reduces benzodiazepine doses and prevents progression of AWS symptoms. 13
Protocolized management of AWS in the surgical-trauma population has demonstrated significant reduction in benzodiazepine use and ICU admissions. 14 Our institutional phenobarbital-based protocol provides a standardized approach to identify and treat trauma patients at high risk of severe AWS or already demonstrating severe AWS. The purpose of this study is to assess the effectiveness and safety outcomes of non-ICU trauma patients at risk of or experiencing AWS before and after implementation of a phenobarbital-based protocol.
Methods
This study was approved by the MaineHealth Institutional Review Board. A retrospective, single-center pre-post study evaluating non-ICU adult trauma patients who were at risk of or experiencing AWS was conducted. Patients were excluded if age <18 years, not admitted to a trauma service, not at risk of AWS, received an ethyl alcohol infusion, or had a known allergy to phenobarbital or another antiseizure drug. The phenobarbital-based AWS protocol was implemented in October 2018. Patients admitted between June 1, 2017 and May 31, 2018 were identified for the pre-implementation group (PRE) and patients admitted between November 1, 2018 and October 31, 2019 were identified for the post-implementation group (POST). A 6-month wash-out period occurred to allow for protocol implementation.
No standardized protocol existed during the PRE group to guide utilization of phenobarbital or other adjunctive agents and patients were managed primarily with STT benzodiazepine based on the CIWA-Ar. A standardized phenobarbital-based protocol was developed with the purpose of identifying and treating patients at high risk of severe AWS or already demonstrating severe AWS (Figure 1). High risk of severe AWS was defined as patients actively drinking within the past 30 days, with a history of previous AWS or with a positive admission blood alcohol level (BAL), plus a history of alcohol withdrawal seizures and/or delirium tremens. Severe AWS was defined as a CIWA-Ar score >16 and a history of alcohol use and symptom onset within 48 h of last drink. Additional high risk inclusion criteria were considered based on provider discretion. Adjunctive medications such as clonidine and antipsychotics were recommended in the phenobarbital-based protocol. Scheduled clonidine was recommended for autonomic symptoms (eg, tachycardia, hypertension, tremors, and sweating). As needed antipsychotics (eg, haloperidol and olanzapine) were recommended for agitation associated with hallucinations or disorientation. Benzodiazepines were to be discontinued upon phenobarbital initiation. If POST patients did not meet the phenobarbital-based protocol criteria, they were monitored with CIWA-Ar and received STT lorazepam if indicated. Institutional phenobarbital-based alcohol withdrawal protocol.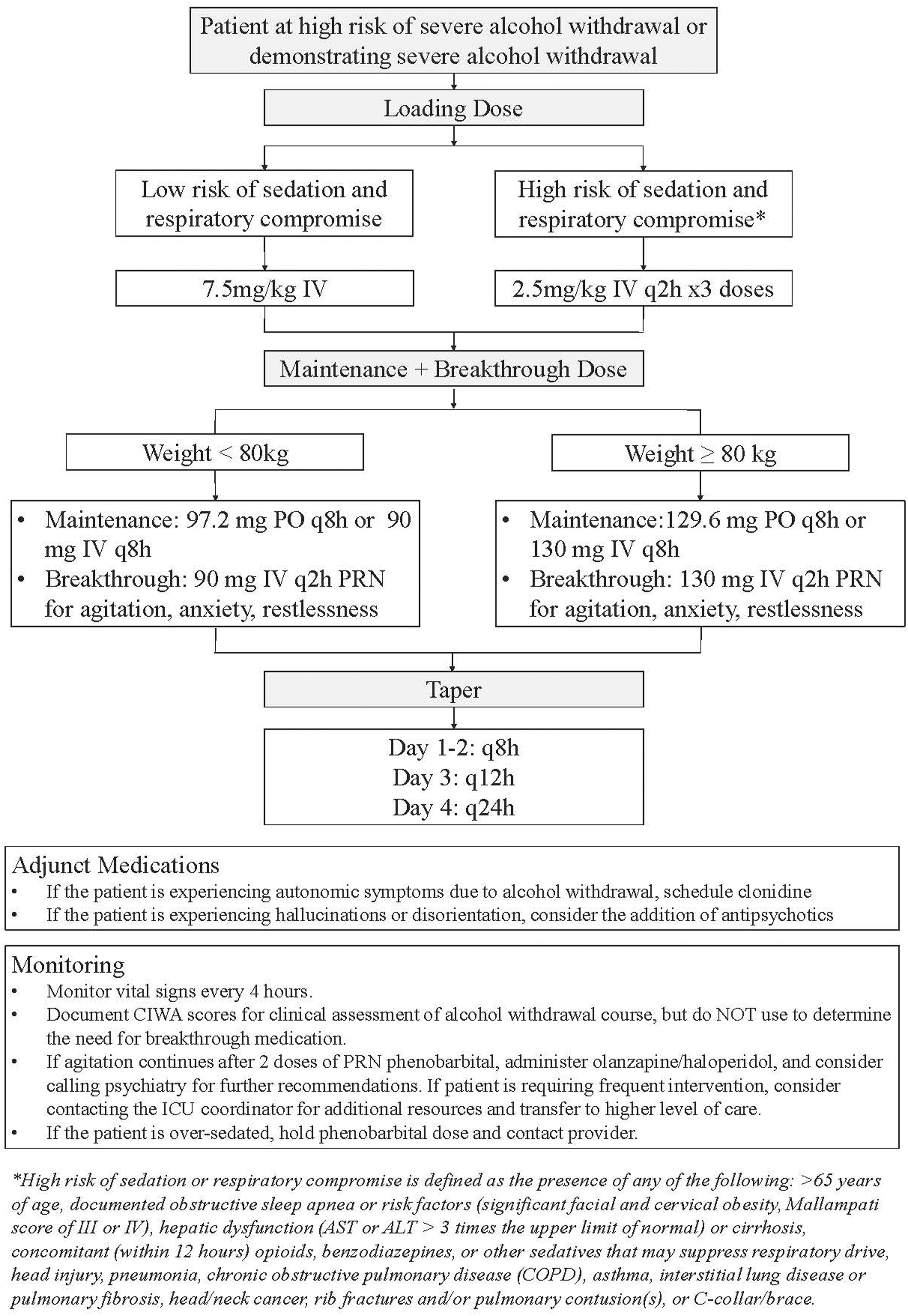
Primary effectiveness outcome was AWS-related complications (seizures, delirium tremens, and transfer to higher level of care). Secondary effectiveness outcomes were hospital length of stay (HLOS), benzodiazepine use, and adjunctive medication use. Safety outcomes evaluated were respiratory depression (defined as need for increased monitoring, new or increased oxygen requirement, or need for intubation), CNS depression (defined as documentation of somnolence, excessive sedation requiring medication holds, or Sedation Agitation Scale of 1-2 (if available) within 8 hours of drug administration), and AEs associated with phenobarbital including Stevens-Johnson Syndrome (SJS), drug reaction with eosinophilia and systemic symptoms (DRESS), propylene glycol toxicity, hepatotoxicity, or hypotension. Hepatotoxicity was defined as a new alanine aminotransferase >3 times the upper limit of normal (ULN), alkaline phosphatase or total bilirubin >2 times the ULN, or a doubling of the baseline value if it was already abnormal prior to phenobarbital initiation. 15 Hypotension was defined as a mean arterial pressure (MAP) of less than 65 mmHg or SBP ≤ 90 mmHg within 8 h of administration.16–19 Protocol adherence was assessed with patient indication, benzodiazepine discontinuation upon initiation of phenobarbital, and appropriateness of phenobarbital dosing. Subgroups analyzed included patients with high risk of severe AWS, patients with traumatic brain injury (TBI), as these patients may be at increased risk of CNS depression with these agents, and patients with rib fractures, as these patients may be at increased risk of respiratory depression with these agents.
Categorical variables were compared using the Chi square or Fisher’s exact test as appropriate, and continuous variables were compared with the Mann-Whitney U -test using R v1.4.1103 with a significance level of P < .05.
Results
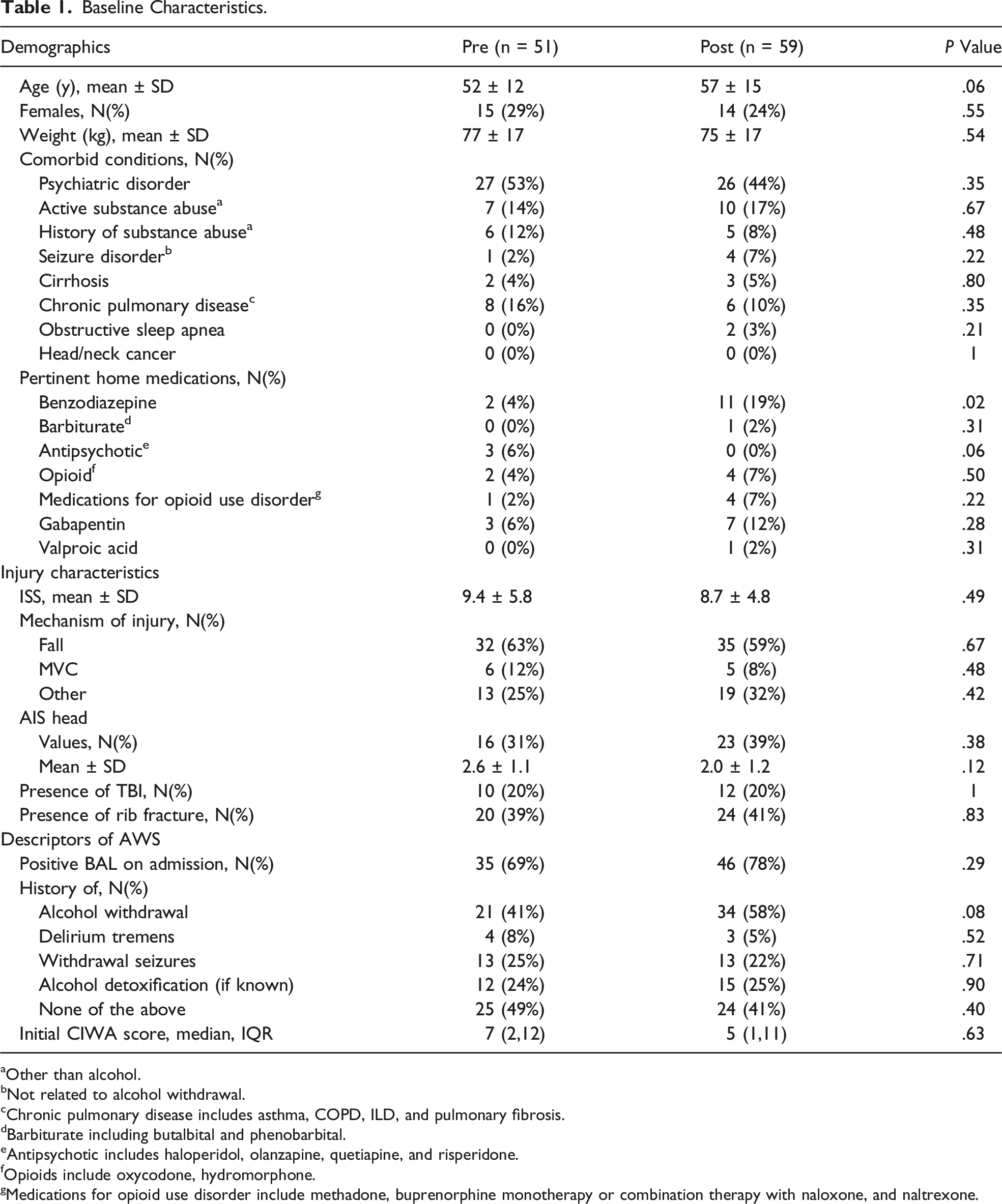
One hundred and ten patients were included with 51 patients in the PRE and 59 in the POST (Figure 2). Patients were similar in age, sex, and comorbid conditions (Table 1). POST patients were more commonly prescribed benzodiazepines at home (4% vs 19%, P = .02). Both groups had similar injury severity scores (ISS) (9.4 vs 8.7, P = .49), abbreviated injury score-head (AIS-head) (2.6 vs 2.0, P = .12), mechanism of injury, and presence of TBI or rib fractures. There was no difference in incidence of positive admission BAL or in documented history of AWS. Patient selection. Baseline Characteristics. aOther than alcohol. bNot related to alcohol withdrawal. cChronic pulmonary disease includes asthma, COPD, ILD, and pulmonary fibrosis. dBarbiturate including butalbital and phenobarbital. eAntipsychotic includes haloperidol, olanzapine, quetiapine, and risperidone. fOpioids include oxycodone, hydromorphone. gMedications for opioid use disorder include methadone, buprenorphine monotherapy or combination therapy with naloxone, and naltrexone.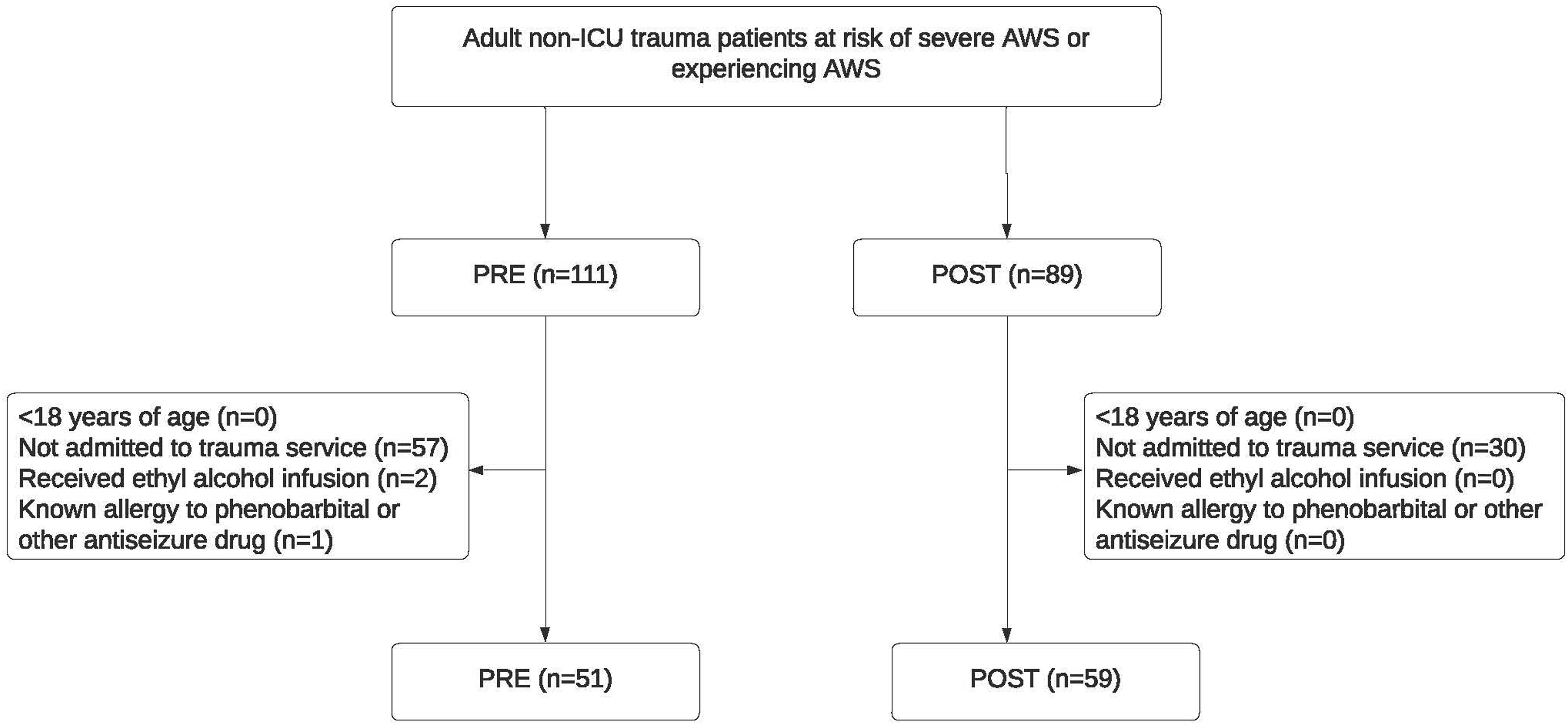
Management of AWS involved STT lorazepam alone in 31 PRE and 11 POST patients. Phenobarbital monotherapy was administered in 5 PRE and 34 POST patients. The remainder of patients received benzodiazepines followed by phenobarbital (14 PRE, 14 POST). One patient in the PRE group did not require any GABA agonist therapy.
Clinical Outcomes.
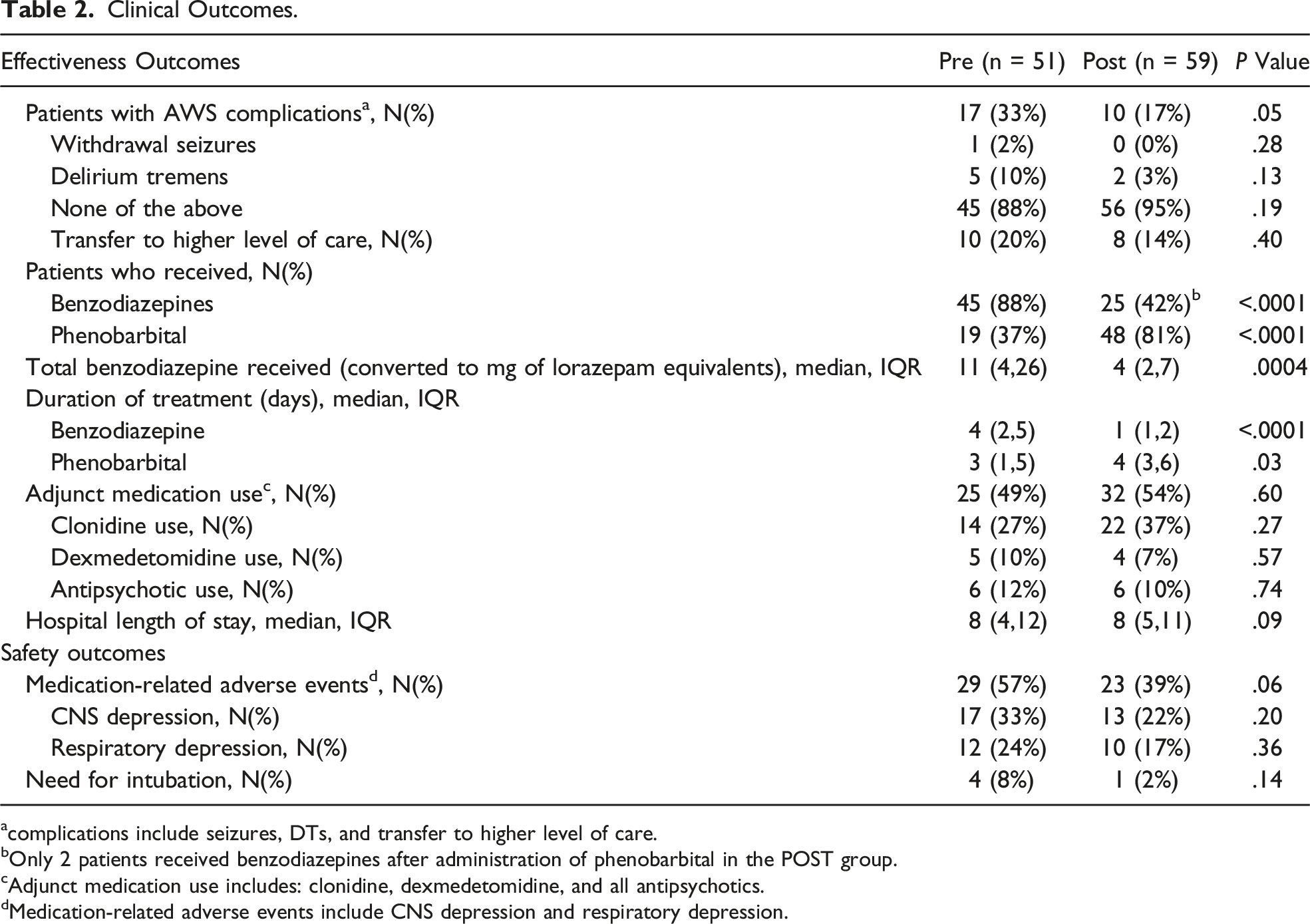
acomplications include seizures, DTs, and transfer to higher level of care.
bOnly 2 patients received benzodiazepines after administration of phenobarbital in the POST group.
cAdjunct medication use includes: clonidine, dexmedetomidine, and all antipsychotics.
dMedication-related adverse events include CNS depression and respiratory depression.
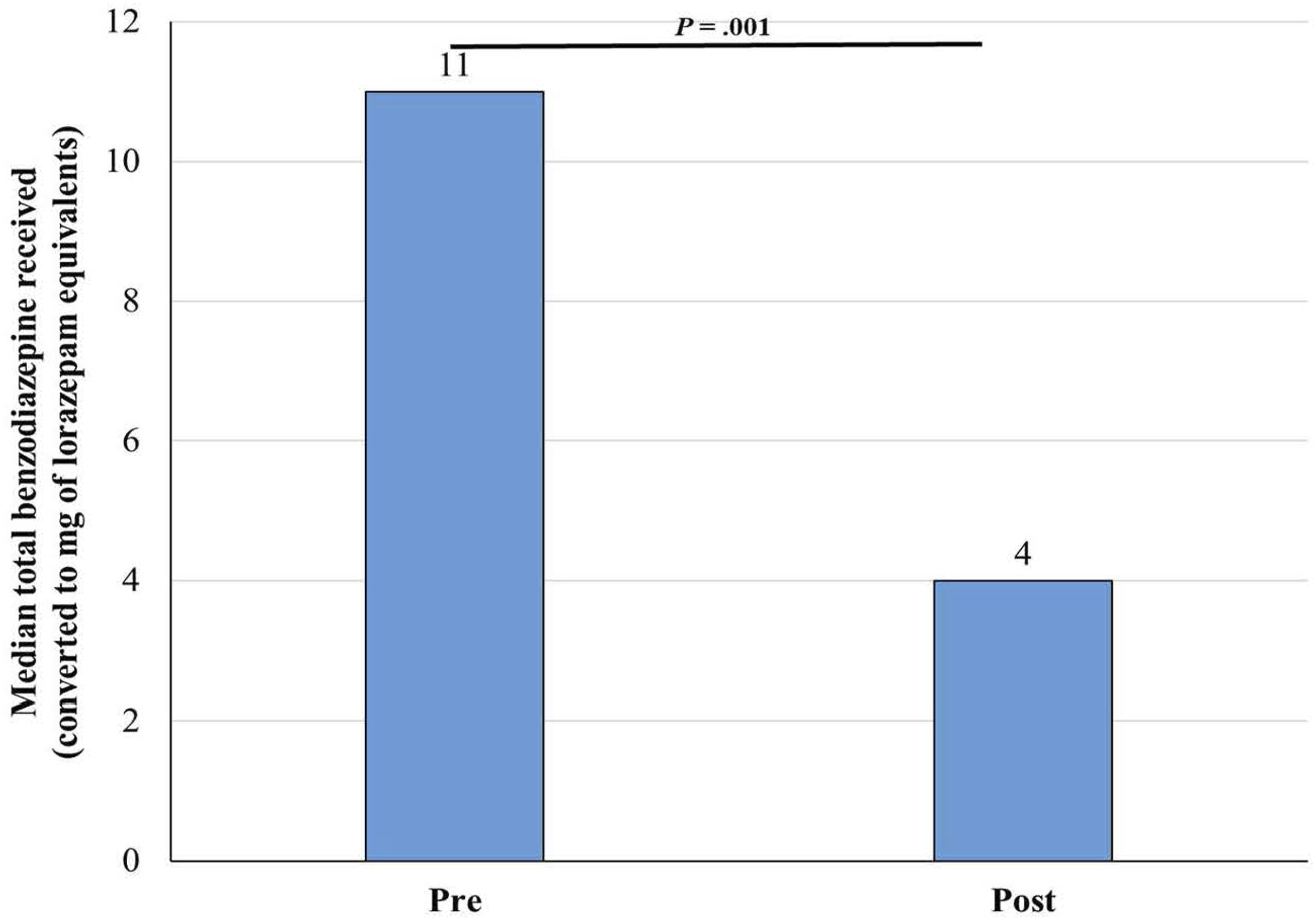
Benzodiazepine requirements PRE and POST phenobarbital-based protocol.
In terms of safety outcomes, 29 (57%) of PRE patients developed respiratory and CNS depression compared to 23 (39%) in the POST (P = .06). Among the patients who received phenobarbital, 6 patients experienced hypotension (2 PRE, 4 POST). Other contributors to hypotension (eg, medications and sepsis) were identified in 5 of the 6 cases. Of the 3 cases that required intervention, 2 patients were in ICU at time of hypotension, and 1 patient was in intermediate care. The interventions included phenobarbital dose held (n = 3), fluid bolus (n = 1), and initiation of vasopressor (n = 1). There were no documented events of SJS, DRESS, propylene glycol toxicity, or hepatotoxicity.
Subgroups Analysis.
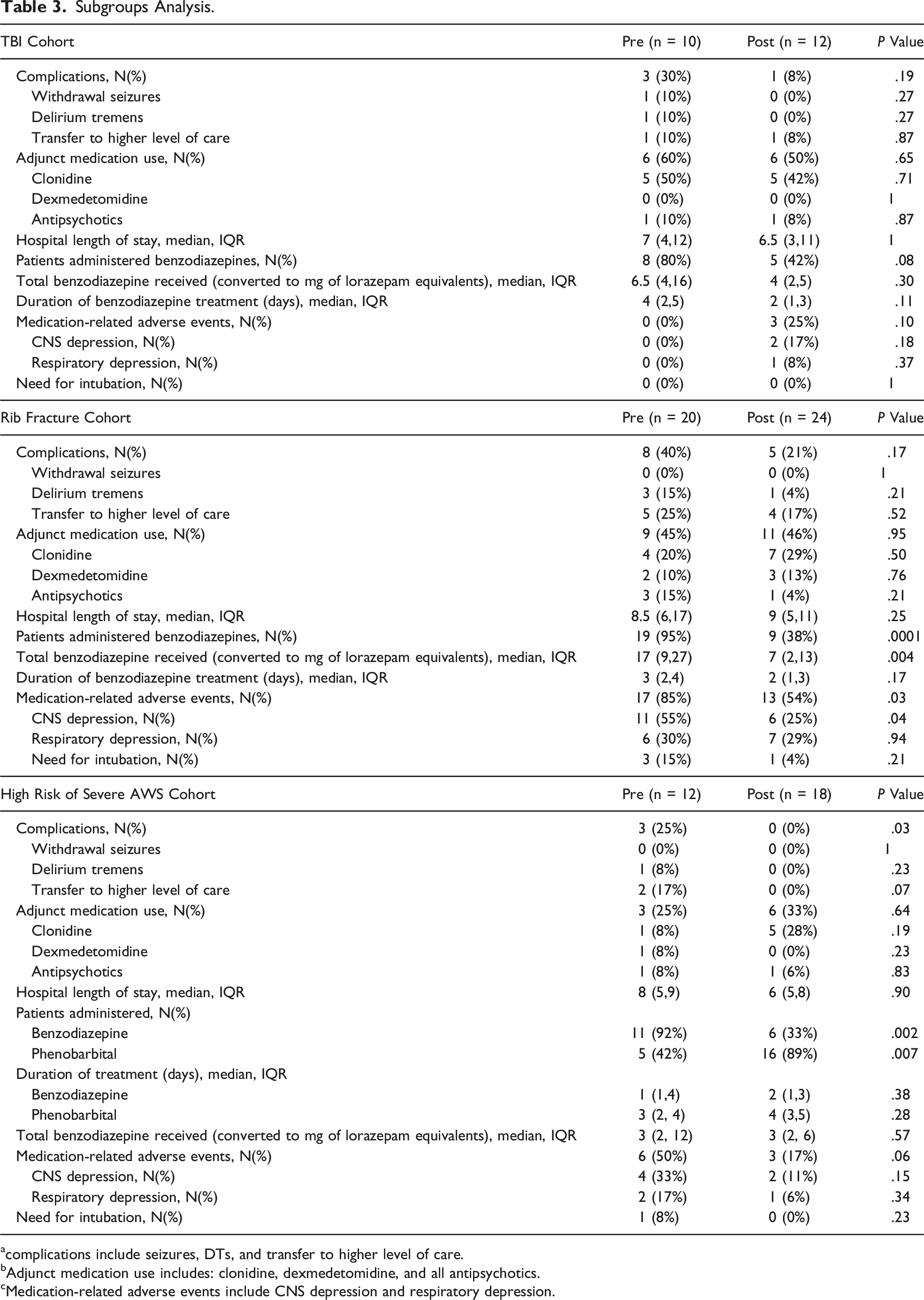
acomplications include seizures, DTs, and transfer to higher level of care.
bAdjunct medication use includes: clonidine, dexmedetomidine, and all antipsychotics.
cMedication-related adverse events include CNS depression and respiratory depression.
Overall protocol adherence in the POST group was high. Four patients (7%) were indicated for phenobarbital but did not receive it. While the phenobarbital-based protocol recommends discontinuing benzodiazepines upon phenobarbital initiation, 2 patients in the POST required discrete one-time doses of benzodiazepines after phenobarbital initiation for acute agitation. A total of 75% of loading doses, 93% of maintenance doses, and 71% of as needed doses were ordered appropriately per the phenobarbital-based AWS protocol. There was low adherence to protocol taper recommendations at 38%.
Discussion
In this study of non-ICU adult trauma patients who were at risk of or experiencing AWS, the implementation of a phenobarbital-based AWS protocol appears to be safe and effective in preventing AWS-related complications. There was no difference in the development of alcohol withdrawal seizures, delirium tremens, or need for transfer to a higher level of care. Results are similar to prior studies evaluating the use of phenobarbital for the management of AWS in trauma patients. Two previous studies evaluated critically ill surgical-trauma patients receiving phenobarbital for AWS.20,21 In a study of 31 patients receiving phenobarbital monotherapy, none of the patients developed AWS-related complications including seizures, alcoholic hallucinosis, or alcohol withdrawal delirium. 20 Another study of 60 patients receiving at least one dose of phenobarbital, initiated per provider discretion without protocol, suggested the time to initiation of phenobarbital was longer in patients with AWS-related complications. 21 Both trials lacked comparators, and support the use of a protocolized approach to phenobarbital use for AWS in the trauma population, such as in our study. A study of 85 surgical-trauma patients found that phenobarbital-treated patients were less likely to develop alcohol withdrawal delirium, uncomplicated AWS, or experience medication AEs compared to patients treated with a fixed-dose benzodiazepine-based protocol. 6 In addition, no differences in mortality or LOS were observed. Our study differs in that our PRE group patients were predominantly treated with STT benzodiazepines rather than a fixed-dose benzodiazepine regimen.
Similar to the aforementioned studies,6,20 our protocol includes not only treatment of AWS but early identification and phenobarbital prophylaxis of patients at high risk of severe AWS. We report on our high risk of severe AWS cohort and found that our POST patients were less likely to experience AWS-related complications compared to the PRE demonstrating the effectiveness of prophylactic phenobarbital. Overtreatment is a potential concern with pre-emptive treatment but there was no difference in medication-related AEs between the two groups and no intubations in the POST. Our findings are consistent with a recent publication by Kip et al that demonstrated a lower need for rescue therapy without increased AEs with the use of prophylactic phenobarbital in trauma patients. 22 In their study, 44% of patients were admitted to the ICU for phenobarbital initiation, phenobarbital use was not protocolized with only 13% received a phenobarbital loading dose, and HLOS was 5 days longer in the phenobarbital group. In contrast, our study provides a protocolized approach in which none of our patients were admitted to the ICU for phenobarbital initiation and HLOS was similar between PRE and POST groups. 22
Our protocol recommends a phenobarbital taper which may increase treatment duration, but we found no difference in HLOS. The lack of a difference between adjunctive medication use was likely a result of the phenobarbital-based protocol recommending adjunctive medications including clonidine and antipsychotics as clinically indicated. Patients in the POST were less likely to receive benzodiazepines given our protocol recommendation of stopping benzodiazepines upon phenobarbital initiation. No POST patients required more than 1 dose of benzodiazepines after phenobarbital initiation.
Phenobarbital appears safe for treatment of AWS in the trauma population with no difference in AEs. Both patients who required intubation within 8 hours of phenobarbital administration, one in the PRE and one in the POST, had other clinical explanations for respiratory failure including hospital-acquired pneumonia for the PRE patient and massive bilateral pulmonary embolism for the POST patient. Our study demonstrated that phenobarbital use did not increase risk of CNS or respiratory depression and appears to be safe in the high-risk TBI and rib fracture subgroups. Six patients who received phenobarbital experienced hypotension, but in the majority of cases, other contributors were involved. No other significant AEs associated with phenobarbital were documented.
There are several limitations to this study. Given the retrospective nature of this study, the data gathered was solely based on information documented in the electronic medical record (EMR) and Trauma Registry. Formal medication reconciliations were not documented for every patient and these data were reliant on admission notes. The incidence of withdrawal seizures and delirium tremens was based on documentation of diagnosis within the EMR. We did not use a validated tool, such as Prediction of Alcohol Withdrawal Severity Score (PAWSS), 23 to identify patients at high risk of severe alcohol withdrawal, but rather incorporated key components of this scale in our protocol. The initiation of phenobarbital vs STT lorazepam may be influenced by provider biases. The primary outcome could have been confounded by adjunctive medication use which we tried to minimize by collecting on pertinent adjunctive medications for the management of AWS. While held doses was part of the definition for CNS depression, we did not collect on the number of doses held which may have influenced our transfer to higher level of care, CNS and respiratory depression endpoints. Additionally, we did not have a standardized protocol for monitoring for phenobarbital-related AEs, such as hepatotoxicity or DRESS, and relied on chart review and documentation for identification of these AEs. Our small sample size may have influenced our ability to detect these rare AEs. Finally, this was a small, single-center study in trauma patients and may not be generalizable to other patient populations. Given the small sample size of our subgroups and lack of power analysis, further studies are needed to evaluate our findings.
This study adds to the growing body of literature on the effectiveness and safety of phenobarbital as an alternative to benzodiazepines for AWS management in the trauma population. This study demonstrates that a phenobarbital-based AWS protocol was effective in preventing AWS-related complications and decreasing benzodiazepine use without an increased risk of medication-related AEs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.