
Abstract
Introduction
Unintentional injury is the leading cause of death among children. Much can be gleaned from the adult literature in understanding the characteristics that lead to recidivism in efforts to establish interventions for prevention. Our study aims to evaluate the rates, demographics, and features of pediatric trauma recidivism.
Methods
This was a retrospective single-institution review at a level-1 pediatric trauma center of children and young adults (ages 0-28) with traumatic injuries from January 2008 to April 2023. Patients with 1 or more prior visits to our institution’s trauma center (recidivists) were identified and compared with those with single admissions. Chi-square tests were used to statistically analyze the two groups.
Results
Pediatric/young adult trauma recidivists were 4.4% of the total trauma population captured (n = 14,613). Of the total trauma group, 55% were under 18 years old. Recidivists had higher percentages of patients who were male (82% vs 69%, P < .01), African American (36% vs 24%, P < .01), involved in penetrating trauma (33% vs 17%, P < .01), self-pay/uninsured (17% vs 12%, P < .01), and have abuse reported (5% vs 4%, P = .04). The primary county for recidivism patients was Forsyth with most patients from a specific zip code in an urban area of the county. The average time between visits for recidivists was 1,066 days.
Conclusions
Pediatric/young adult trauma recidivism is associated with specific characteristics including male, African American race, penetrating trauma, and uninsured status. Recidivists are primarily presenting from a zip code with low socioeconomic status. It is critical to develop targeted interventions to help this population in trauma prevention.
Introduction
In 2021, the US experienced 62 million injuries of which there were 224,935 preventable deaths, costing 1.2 trillion dollars. 1 Cunningham et al analyzed the data for the major cause of death of children and adolescents in the US up to 2016. 2 At that time, motor vehicle crashes accounted for the largest number of annual deaths, followed by firearm injuries. In 2020, firearm violence became the leading cause of death. 3 It has been reported that there is an increased incidence of these injuries and subsequent injuries (recidivism) in defined populations or as the result of certain behavior and may provide a target for future intervention. There have been relatively few of these studies focused on children and young adults.
In an urban emergency department in Newark, NJ, 896 pediatric patients were discharged with a firearm injury over a 12 year period. The recidivism rate was 8.8% including 9 patients who were admitted for gunshot wounds on 3 separate occasions with a 22% mortality rate. Also of note, all recidivists were male and 53% came from a three square mile area. 4 Another retrospective study that examined firearm recidivism in Newark, NJ, over a period of 18 years found that most of the recidivists were African American males. 5
In a retrospective cohort study in Houston, 21% of injured patients were readmitted for traumatic injury. Patients on Medicaid were nearly three times more likely to be readmitted for a traumatic injury. 6 In a study from San Francisco, out of 890 patients who were victims of violent injury, independent predictors of recidivism were black race (OR = 2.1), male sex (OR = 2), injury due to firearms (OR = 1.7), and living in the lowest zip code socioeconomic quartile (OR = 1.59). They suggested that the socioeconomic position of their neighborhood of residence independently correlated with their risk of violent injury. 7
A group from the Maryland analyzed 46,266 trauma patients and of those, 7% (3147) had one or more admission over a 10 year period than patients who had a single admission over the study period. The trauma registry was linked to the National Death Index (NDI) to determine the cause and time of death after hospital discharge. National Death Index linkage of this nature has been shown to have greater than 95% sensitivity and 99% specificity. 8 The study found that recidivists were more likely to be younger, male, black, have a blood alcohol greater than 8 mg/dl, have a positive urine drug screen, and suffer a penetrating injury than non-recidivists. Recidivists had a higher long-term mortality. 8 A study based in Baltimore, Maryland, found that black men are overrepresented among trauma recidivists. The study used secondary data analysis and identified a group of 191 low income black men who were treated at the level-1 trauma center. Of this specific patient population, 58% were identified as having been admitted more than one time to the hospital for a trauma-related injury. 9 Researchers at a children’s hospital in Washington DC looked at the National Readmissions database from 2010 to 2015 and analyzed the data for patients ≤18 years with major traumatic injuries. Of the 286,508 patients analyzed, recidivists represented 2.9% of the population. The study found that recidivists had a higher proportion of severe head injury and were more likely to have public insurance. 10
In summary, these studies suggest that after a violent injury in children and young adults, recidivism is more frequent in victims who are black, from low socioeconomic neighborhoods, firearm injury victims, male, and have a positive blood or alcohol screen.
We decided to focus on recidivism after taking care of a victim of a school shooting. Our group had previously cared for the shooter when he was shot by the victim. Their roles were subsequently reversed and resulted in a fatality. This incident made us pause and wonder whether we could have changed the outcome and focused our work on the issue of recidivism.
Materials/Methods
This is a single-institution retrospective review at a level-1 adult/pediatric trauma center, which focused on patients ages 0-28 years old who presented with traumatic injuries. Patients with traumatic injuries were recorded from January 2008 to April 2023 per the institutional trauma registry. The adult trauma registry, emergency department log, and state trauma registry were also used to analyze recidivists. Demographics were recorded including age, sex, ethnicity, and insurance status. Injury Severity Score (ISS), mechanism of injury (MOI), disposition, length of stay, and abuse were also analyzed.
Patients were defined as recidivists if they appeared twice or more in the registry. Patients were defined as non-recidivists if they appeared only once in the registry. This registry only includes patients at the single institution, which is an 885-bed tertiary care hospital located in Winston-Salem, North Carolina, serving patients in 24 counties. Data was analyzed and descriptive statistics were generated along with chi-square and Student t-tests used to determine significance between recidivists and non-recidivists (Stata, version SE 18, StataCorp). Length of stay data was not available for all patients (missing in 5,419 patients), and analysis of length of stay was performed using data from patients for which this variable was available. Our study was approved by our institution’s IRB.
Results
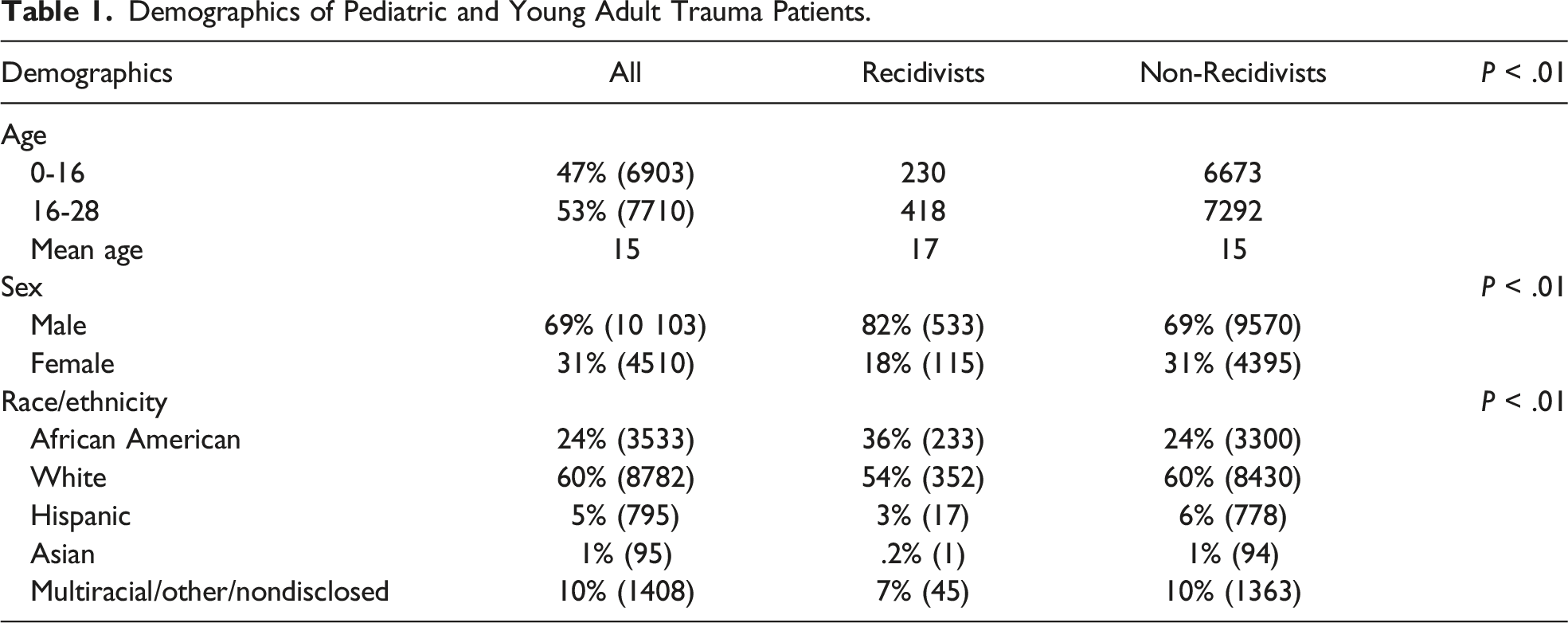
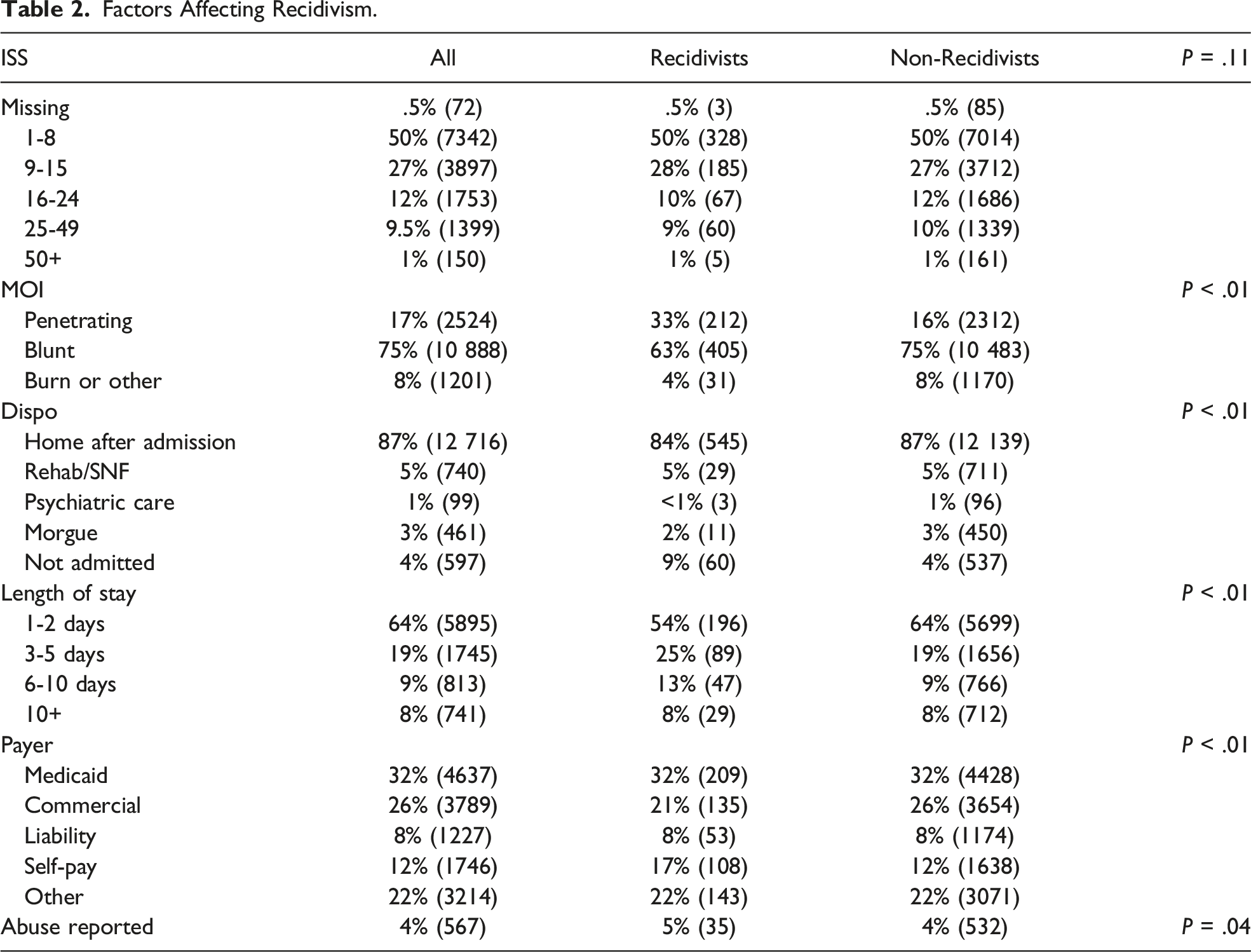
From January 2008 to April 2023, there were 14,613 patients between ages 0 and 28 in the trauma registry. Pediatric and young adult trauma recidivists comprised 4.4% of the total trauma population. Of the patients in the cohort, 47% were ages 0-16 and 54% were 16-28 with a mean age of 15 years old for the entire group. 69% were male, and 31% were female. Race/ethnicity data showed 24% were African American, 60% were white, 5% were Hispanic, 1% were Asian, and 10% were multiracial or did not disclose this information. Notably, recidivists exhibited distinct characteristics compared to the general trauma population. These characteristics included a higher percentage of males (recidivist 82% vs non-recidivists 69%, P < .01), individuals of African American descent (36% vs 24%, P < .01), cases involving penetrating trauma (33% vs 17%, P < .01), self-pay/uninsured status (17% vs 12%, P < .01), longer length of stay (25% vs 19%, P < .01), patients not admitted or left against medical advice (9% vs 4%, P < .01), and reported cases of abuse (5% vs 4%, P = .04). Other characteristics investigated that were not statistically significant were Injury Severity Score (ISS).
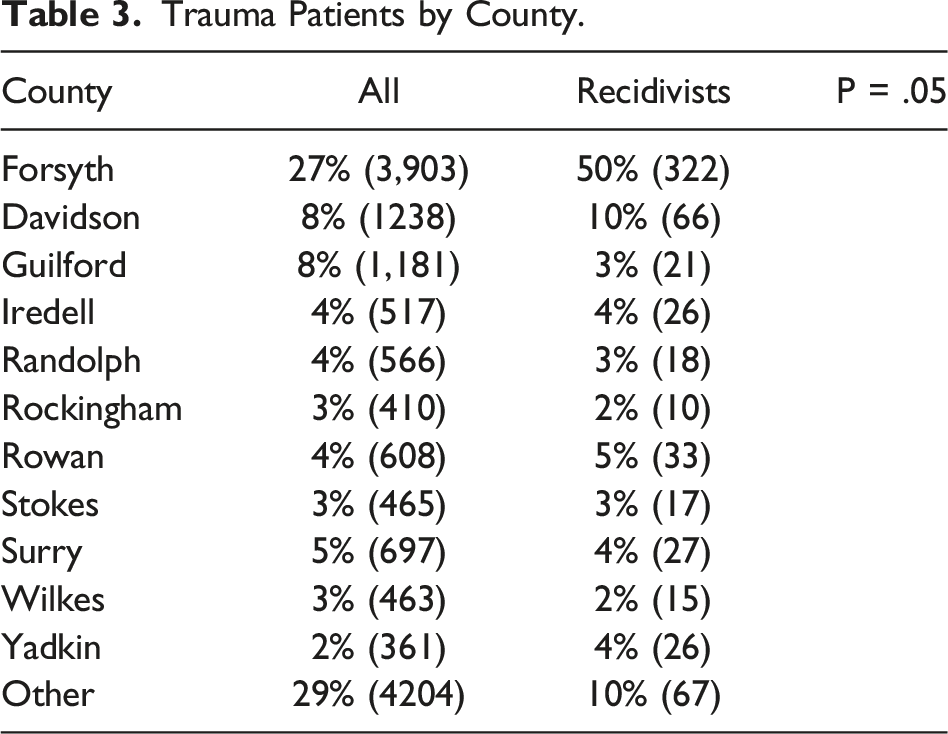
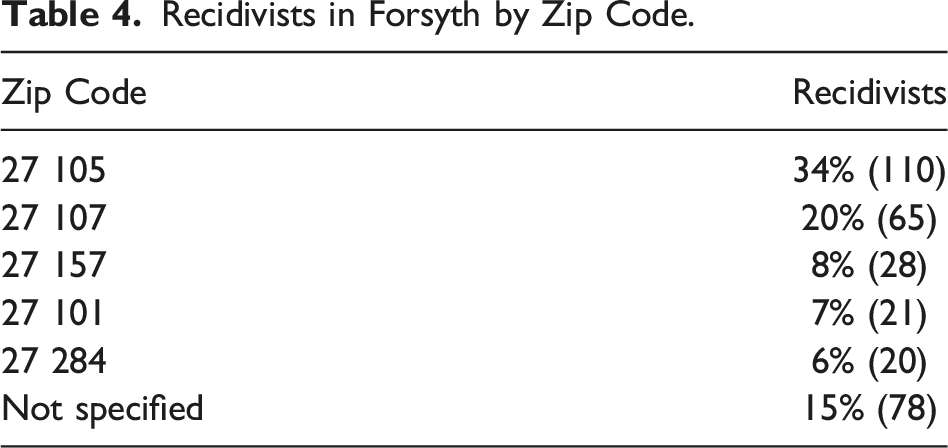
Geographically, the primary county for recidivism cases was Forsyth, with the majority of patients originating from the 27 105 zip code. Notably, this area was characterized by low socioeconomic status. Additionally, the average time between visits for recidivists was 1066 days.
Discussion
Demographics of Pediatric and Young Adult Trauma Patients.
Factors Affecting Recidivism.
Trauma Patients by County.
Recidivists in Forsyth by Zip Code.
Another significant aspect impacting the interpretation of our study results is the observed association between trauma recidivism and distinct patterns in health care utilization. Notably, recidivists were found to have a longer length of stay and were more likely to either not be admitted or leave against medical advice (AMA). The extended length of stay among recidivists suggests complex health care needs, which one may assume typically involves more severe injuries or complications. However, it is noteworthy that our study did not identify a significant difference in injury severity scores between pediatric and young adult trauma recidivists and the general trauma population. This finding suggests that, despite the distinct characteristics and health care utilization patterns observed among recidivists, the severity of the initial injuries leading to hospitalization may not differ significantly from those of non-recidivists. A plausible hypothesis for an extended length of stay in patients who return with a traumatic injury may stem from insufficient resources identified during discharge planning, resulting in an extended duration spent on formulating an adequate discharge plan. It is important to note, that unfortunately data for length of stay was missing for many patients (n = 5419), thus this information does not reflect the entire cohort. Further investigation into the interplay of behavioral, environmental, and socioeconomic factors is crucial for unraveling the complexity of trauma recidivism and tailoring interventions that address the underlying causes beyond the immediate physical injuries. Recognizing this lack of difference in injury severity scores is pivotal for refining our understanding of the multifaceted nature of pediatric and young adult trauma recidivism.
Moreover, the higher likelihood of not being admitted or leaving AMA emphasizes challenges in ensuring continuity of care for this vulnerable population. Understanding the factors influencing these health care utilization patterns is essential for designing interventions that address not only the immediate trauma-related issues but also the broader complexities associated with recidivism and patient adherence to recommended medical care. Future research should delve into the specific reasons behind these utilization patterns, considering both clinical and psychosocial factors, to inform targeted strategies aimed at optimizing health care outcomes for pediatric and young adult trauma recidivists.
While our study provides valuable insights into pediatric and young adult trauma recidivism, it is crucial to acknowledge certain limitations that may impact the generalizability and interpretation of the findings. One being this research is based on data collected from a single center, which can limit the generalizability of the results to a broader population. Trauma demographics and risk factors can vary across different regions and health care settings; however, our data points toward the general trends of recidivism data in the adult population. Additionally, mortality data was not available for all patients in this study. The absence of mortality data represents a notable limitation in our study, impacting the comprehensiveness and interpretation of the results. Without access to information on mortality rates among pediatric and young adult trauma recidivists, our understanding of the overall impact and severity of trauma-related incidents is incomplete. Mortality data is pivotal in assessing the ultimate outcomes of traumatic events and understanding the potential lethality of injuries sustained. The lack of such information limits our ability to draw conclusions about the long-term consequences of trauma recidivism, including survival rates and the potential interplay between recurrent trauma and mortality risk. Additionally, mortality data could provide insights into whether specific demographic or clinical factors are associated with more severe outcomes, thus influencing the development of targeted interventions aimed at reducing both the incidence and severity of pediatric and young adult trauma recidivism. Future research endeavors should prioritize the inclusion of mortality data to enhance the depth and robustness of findings in this critical area of study.
Conclusion
In conclusion, the study provides valuable insights into the distinct characteristics and patterns associated with pediatric and young adult trauma recidivism. The identified risk factors, including gender, race, type of trauma, socioeconomic status, and abuse history, lay the foundation for targeted interventions. Developing preventive measures that address the multifaceted nature of trauma recurrence is crucial.
By contextualizing our findings within the broader landscape of pediatric trauma recidivism research, we contribute to a more holistic understanding of the factors influencing recurrent incidents. This synthesis of evidence reinforces the urgency of adopting a multidimensional approach in developing interventions. Recognizing the interconnectedness of demographic, socioeconomic, and geographic factors is crucial for the design of effective, tailored strategies aimed at breaking the cycle of trauma among pediatric and young adult populations.
The geographical concentration of recidivism cases in Forsyth County, particularly a zip code in an area of the county with lower socioeconomic status, calls for community-specific initiatives that consider the local socioeconomic context. Implementing interventions that bridge the gap in health care access, address underlying social determinants, and provide support for abuse survivors can contribute to breaking the cycle of trauma. Ultimately, this research underscores the urgency of developing and implementing tailored interventions to support pediatric and young adult trauma recidivists, aiming not only at treating injuries but also at preventing future occurrences and improving overall well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.