
Abstract
Background
Current guidelines for management of anorectal abscesses make no recommendations for operative vs bedside incision and drainage (I&D). The purpose of this study was to determine if management in the operating room is necessary to adequately drain anorectal abscesses and prevent short-term complications for patients presenting to the emergency department (ED).
Methods
Patients with perirectal abscesses were identified and divided into two groups based on intervention type: “bedside” or “operative.” Demographic, laboratory, and encounter data were obtained from the medical record. Study outcomes included 30-day complications (return to the ED, reintervention, and readmission). Data were analyzed with univariate and multivariate analyses using SPSS (version 28).
Results
A total of 113 patients with anorectal abscesses were identified. Sixty-six (58%) underwent bedside I&D and 47 (42%) operative I&D. The overall complication rate was 10%. A total of 9 patients (6 bedside and 3 operative) returned to the ED. Six of these patients required reintervention (5 bedside and 1 operative), and 1 was readmitted. Two patients from the bedside group required a second I&D during their index admission. Pre-procedure SIRS (P = .02) was found to be associated with 30-day complications. Provider specialty and training level were not associated with 30-day complications.
Discussion
In this study, for patients presenting to the ED, bedside drainage was found to be an adequate management strategy to achieve complete drainage without a significant increase in the rate of complications when compared to operative drainage.
Key Takeaways
• Bedside I&D is adequate for management of uncomplicated anorectal abscesses presenting to the emergency room. • Provider specialty and training level are not associated with short-term complications following incision and drainage of anorectal abscesses.
Introduction
Anorectal abscesses affect between 68,000 and 96,000 patients in the United States annually. 1 The mainstay of management is source control via incision and drainage (I&D). Postoperative complication rates exceed 30% and have been largely attributed to inadequate drainage at the time of index operation. 2 Complications can lead to multiple hospitalizations, increased cost, and decreased quality of life for the patient.
Drainage of anorectal abscesses may be performed either at bedside or in the operating room. Management in the operating room incurs significant associated cost and time commitment but may allow for a more thorough drainage. Bedside I&D, typically done with a local anesthetic, spares the patient general anesthesia but may be more painful, possibly leading to inadequate drainage.
Although the American Society of Colon and Rectal Surgeons (ASCRS) guidelines recommend prompt surgical drainage, they do not provide guidance regarding the best choice of setting for this intervention. 3
Previous studies have examined outcomes of both operative and bedside I&D in outpatient and mixed clinical settings.4,5 To this point, outcome data have yet to be presented directly comparing bedside and operative management for patients with anorectal abscess presenting to the ED - a setting in which they are frequently encountered.
The purpose of this study was to compare the outcomes of operative and bedside I&D in order to determine if bedside drainage is adequate to manage patients with uncomplicated anorectal abscesses presenting to the ED. The secondary aim of this study was to identify predictors of operative management as well as risk factors for short-term complications in this population.
Methods
We conducted a retrospective study approved by the Huntington Hospital institutional review board (Pro00073259). The study included patients who presented to the Huntington Hospital ED from 2015 to 2020 with an anorectal abscess. Only patients initially evaluated in the ED and who ultimately received I&D were included in the final analysis. Patients were identified using both International Classification of Disease (ICD) version 10 codes (K61.0, K61.2, K61.3, K61.39; L02.215; L02.31) as well as Current Procedural Terminology codes (10160, 45005, 45020, 45990, 46040, 46045, 46050, and 46930). Patients were divided into two groups based on the type of index procedure: bedside I&D or operative I&D. Procedures were performed by surgical attendings, surgical residents, or ED physicians.
Patient and clinical characteristics collected for this study included patient age, sex, race, BMI, medical comorbidities (hypertension, diabetes mellitus, chronic obstructive pulmonary disease, cardiac disease, and bleeding disorder), smoking status, steroid use, vitals, laboratories, history of prior anorectal abscess, presence of preoperative systemic inflammatory response syndrome (SIRS), wound cultures, procedural data, admission, length of stay (LOS), and 30-day reintervention or readmission. Patients with a history of prior abscess or fistula within a year of presentation, inflammatory bowel disease (IBD), hidradenitis, anorectal trauma, anal or rectal malignancy, necrotizing infections, complex abscesses (supralevator and horseshoe), and fistulae identified at index procedure were excluded.
Data are presented as either medians or as counts (with percentages). Counts and medians between groups were compared using Chi-squared analysis or Mann-Whitney U test, respectively. Covariates that were associated with outcomes at the level of P ≤ .1 in the univariate analysis were included in a binary logistic model. Statistical significance was set at P < .05. Data were analyzed using both univariate and multivariate analyses using SPSS (version 28).
Results
Patient Clinical Characteristics.
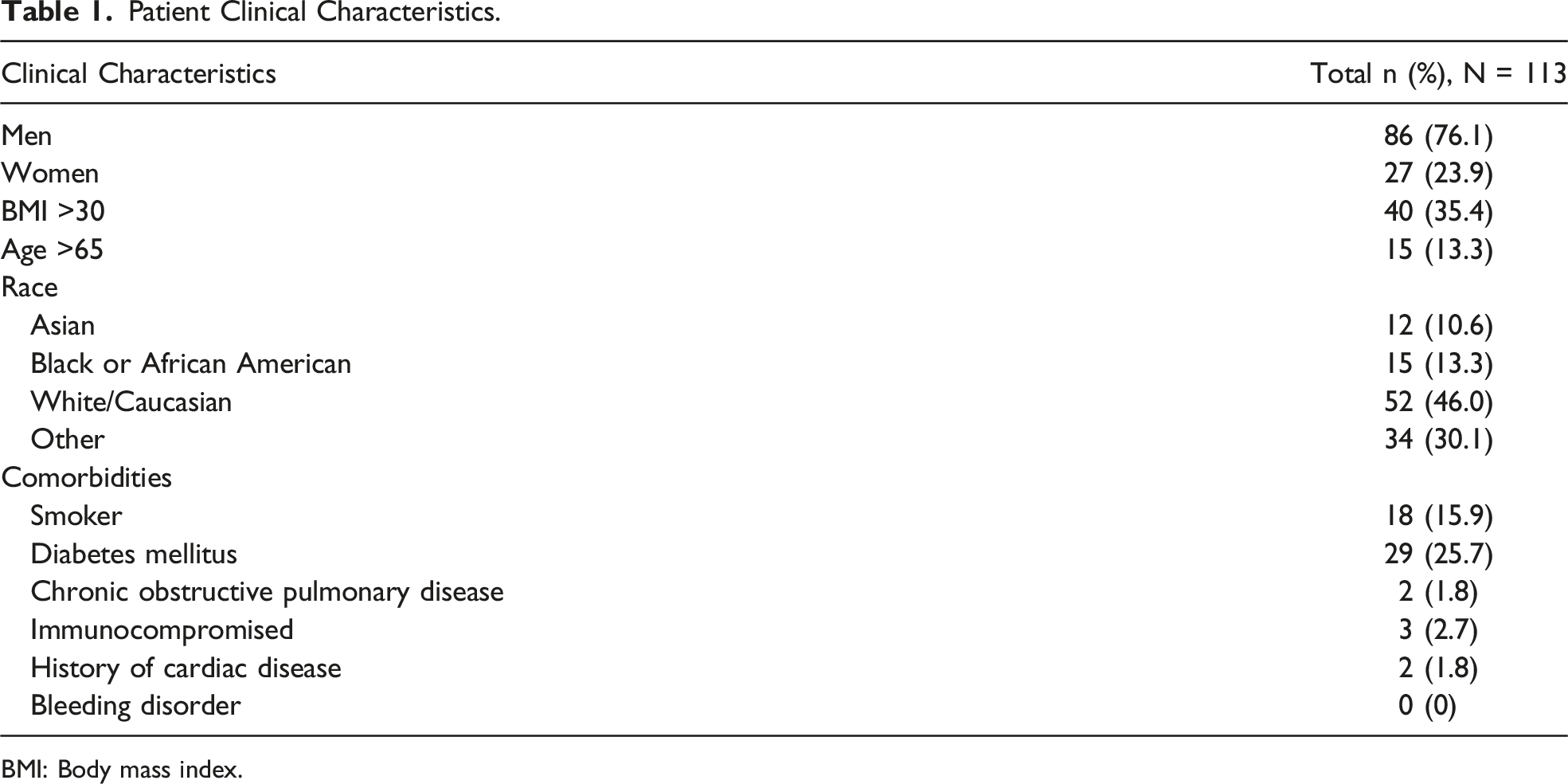
BMI: Body mass index.
Encounter Characteristics Associated With Drainage Type.
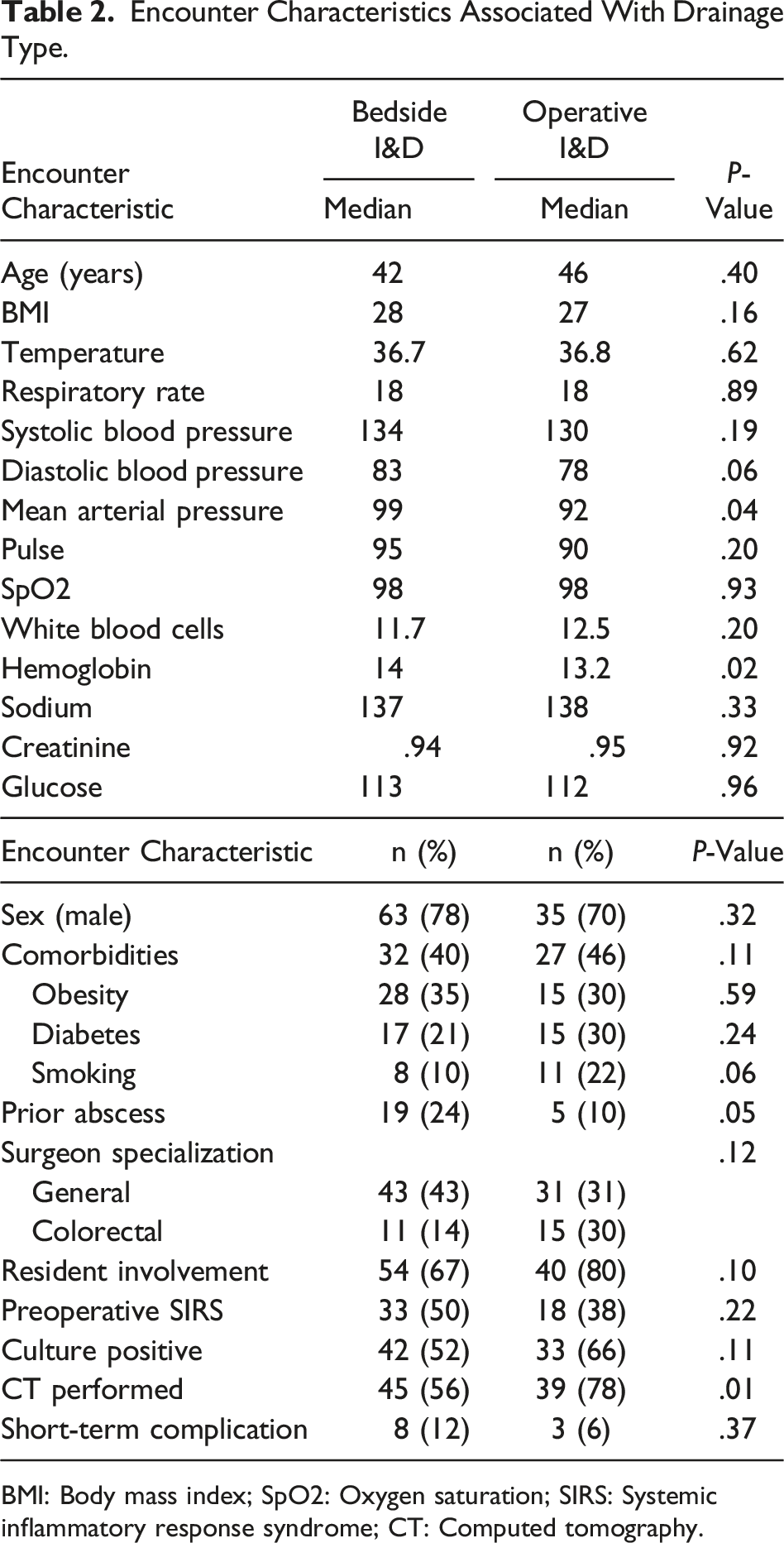
BMI: Body mass index; SpO2: Oxygen saturation; SIRS: Systemic inflammatory response syndrome; CT: Computed tomography.
Encounter Characteristics Predictive of Drainage Type on Multivariate Analysis.
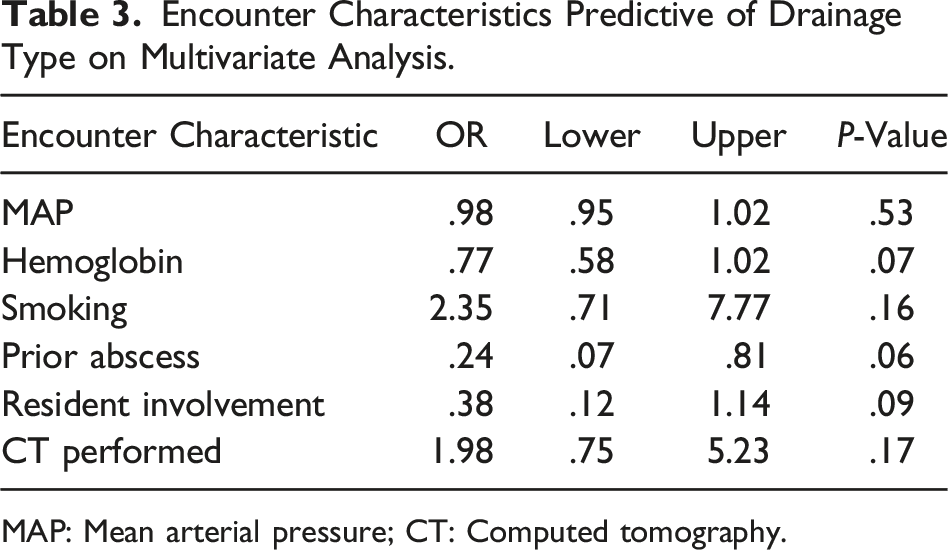
MAP: Mean arterial pressure; CT: Computed tomography.
Overall, 11 patients (10%) experienced 30-day complications. 8 complications were identified in the bedside group. 6 patients returned to the ED within 30 days—5 required reintervention and all were subsequently discharged. Two patients in this group required a second drainage procedure on their index admission. The rate of repeat drainage in this group was 11%.
In the operative group, 3 patients returned to the ED. 2 of these patients required repeat drainage, of which one was admitted and one discharged. The rate of repeat drainage in this group was 4%. No significant difference was found between short-term complications and index procedure type (P = .372). Similarly, no difference was found between rate of repeat drainage between groups (P = .301).
Initial Encounter Characteristics Associated With Early Complications.
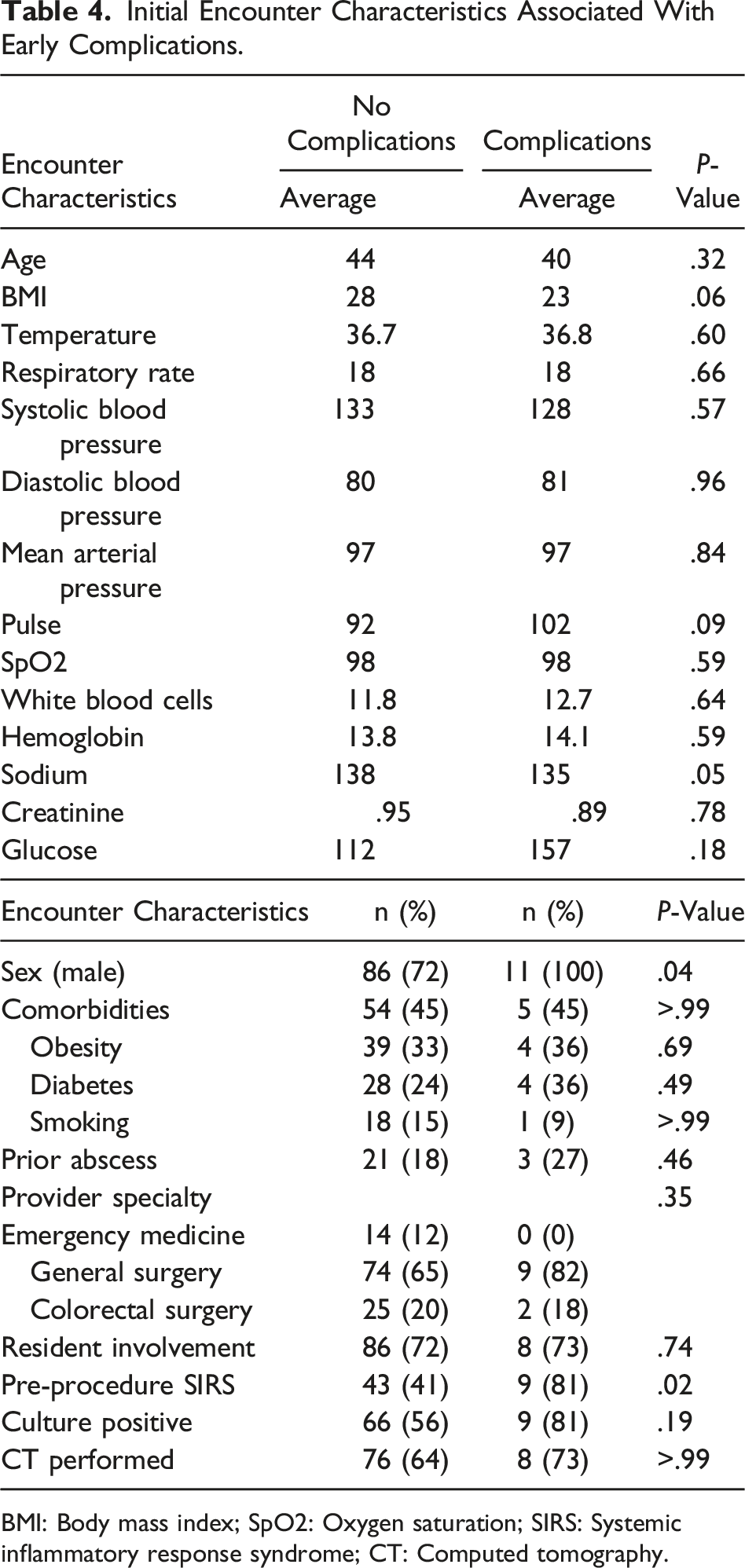
BMI: Body mass index; SpO2: Oxygen saturation; SIRS: Systemic inflammatory response syndrome; CT: Computed tomography.
Discussion
We evaluated the outcomes of different management strategies for anorectal abscess in patients presenting to the ED at a community hospital. Our results demonstrated that the majority of patients received surgical consultation and underwent bedside drainage in the ED setting before being discharged on the same day. The overall 30-day complication rate was 10%. No predictors of operative I&D were identified, and no difference was found in 30-day complications between management types. Pre-procedure SIRS was found to be a risk factor for short-term complications, though not predictive of operative drainage. Finally, resident level and physician specialty had no impact on our measured outcomes.
Two recent studies have similarly investigated different management strategies of anorectal abscess as well as associated complications. In 2020, Sho et al looked at short-term complications and patient risk factors associated with outpatient anorectal I&D in the operating room. 4 The authors found that 34% of patients undergoing outpatient operative drainage required admission, 3.4% required reoperation, and 3% required readmission. In 2023, Narayanan et al evaluated factors associated with abscess recurrence and fistula formation in patients undergoing operative or bedside drainage in mixed clinical settings within a large health care system. 5 They concluded that patients undergoing bedside drainage were more likely to develop recurrent abscesses or fistula-in-ano at 1 year. Although ED patients were likely included in this population, they were not identified and evaluated as a group. To our knowledge, ours is the first study that has looked at management of anorectal abscess in this unique population.
Patients with anorectal abscess commonly seek care in the ED. Central to our investigation was evaluating the efficacy of beside I&D in the management of all uncomplicated anorectal abscesses presenting in this setting. After multivariate analysis, no predictors of operative drainage were identified. Short-term complications, including repeat drainage, were also found to be independent of procedure type, suggesting that patients were adequately drained without the need to go to the operating room. Furthermore, of the patients who underwent beside I&D, 61% were discharged from the emergency department. In contrast, almost 100% of patients who were taken to the operating room were subsequently admitted. Our admission rates following bedside I&D (39%) were similar to Sho et al’s admission rates following elective operative I&D (34%), suggesting that our high admission rates may be reflective of institutional practices rather than a result of operative drainage or general anesthesia. Regardless, our results demonstrate that adequate drainage was achieved at the bedside with equal success and no increase in complications. The increased likelihood of discharge with bedside drainage offers improved convenience for patients as well as decreased utilization of hospital resources related to operating room and admission costs.
After treatment, abscess recurrence has been observed in up to 44% of patients and has largely been attributed to inadequate drainage.6-9 Our overall complication rate was 10%, similar to the rate of short-term complications found previously. 4 As management strategy was not tied to complications in our study, we evaluated other patient and provider factors for association with short-term complications (30-day return to the ED, readmission, and reintervention). Only pre-procedure SIRS was found to be a risk factor. Presence of SIRS in this patient population may be indicative of delayed presentation, infection from more virulent organisms, and/or larger, more complex abscesses, which may predispose patients to inadequate drainage and subsequent return to the ED with need for re-intervention.
Sho et al also identified pre-procedure SIRS as an independent risk factor for short-term complications—specifically admission with LOS >1 day and reoperation. Interestingly, the rate of pre-procedure SIRS in our study was 45%—almost double that found in the outpatient population by Sho et al. In their study, SIRS was attributed to a more advanced disease process and a factor possibly prompting providers to perform I&D in the operating room setting. Contrary to this reasoning, we found no connection between pre-procedure SIRS and operative I&D in a population with a higher rate of pre-procedure SIRS. This finding reinforces the fact that, even with signs of systemic illness, drainage in the operating room did not confer any additional benefit to patients from an outcomes perspective in our study. The discrepancies between our findings may indicate that it may not be the location of procedure that avoids complications but rather adequate drainage.
Perirectal abscess is a problem that is managed by a number of different practitioners. 1 In this study, 88% of patients received a surgical consultation while in the ED—the remainder were managed by the emergency medicine physician alone. Surgical residents of varying levels were involved in almost 90% of surgical consults. In the event that the patient was treated with bedside I&D, the surgical resident routinely saw the patient and performed the procedure after appropriate discussion with the attending surgeon. Surgical resident involvement was not a risk factor for short-term complications. Overall, no medical/surgical specialty or physician training level was associated with short-term complications or intervention type. This is the first study that has looked at practitioner data in a granular fashion for management of this pathology. Outcomes clearly support the involvement of both surgical residents and emergency medicine physicians in the management of uncomplicated perirectal abscesses.
This study had several limitations. Though our population was unique, our sample size was sufficiently small that all risk factors of short-term complications may not have been identified. Similarly, we could not meaningfully analyze risk factors for individual complications due to the small number of patients with recorded 30-day complications. While our complication rates were similar to Sho et al, rates published in the literature vary widely (10%-70%) and include both short- and long-term complications.1,2,6–10 Our relatively low rates may have been due to re-presentation of patients in the outpatient setting or at institutions outside of our ED.
Finally, though we identified SIRS as a risk factor for complications in the ED population, we were not able to establish if preoperative SIRS was acting as a surrogate for disease-specific variables such as abscess size and location. Further quantitative and qualitative characterization of abscesses with CT imaging, if available, would offer another avenue of investigation to further evaluate risk factors for both operative intervention and postoperative complications in this patient population.
In conclusion, patients presenting with perirectal abscess to the ED should be treated with prompt I&D. Bedside drainage is an adequate management strategy to achieve complete drainage in the ED for most patients. Our data suggests that the setting and practitioner specialty/training level has no bearing upon outcomes and should not delay treatment. While we were able to identify pre-procedure SIRS as a risk factor for short-term complications, further research is needed to better delineate additional risk factors and recommendations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.