
Abstract
Achalasia is a neurodegenerative disorder affecting esophageal sphincter function. Treatment options include non-surgical and surgical approaches, such as Heller myotomy (HM). Combining Dor fundoplication with HM is controversial but may prevent gastroesophageal reflux disease (GERD). This retrospective cohort study aimed to assess whether HM with Dor fundoplication reduces GERD rates and increases dysphagia rates. Eighty patients who underwent HM between January 2018 and August 2023 were included. Sixty-four patients had Dor fundoplication and were matched 4:1 to 16 patients without fundoplication. Records were reviewed for GERD and achalasia symptoms at various postoperative time points. No significant differences in GERD or dysphagia symptoms were found between the two groups at any time point. Similarly, there were no significant differences in chest pain or dysphagia treatment. In conclusion, this study suggests that the addition of Dor fundoplication to HM does not significantly impact postoperative GERD or achalasia-related symptoms.
Achalasia is a disorder in which the lower esophageal sphincter fails to relax properly due to neurodegeneration in the myenteric plexus. 1 To diagnose achalasia, upper endoscopy followed by manometry is commonly used. 2 Manometry confirms the incomplete relaxation of the lower esophageal sphincter. Additionally, a barium esophagram can help diagnose achalasia. 2 Treatment options include non-surgical and surgical options, such as Heller myotomy. The addition of fundoplication during Heller myotomy (HM) is a matter of debate. In our study, we compared postoperative GERD and achalasia symptoms in patients who underwent robotic HM with or without Dor fundoplication. Our hypothesis was that patients who had HM with Dor would have a lower rate of GERD symptoms and a higher rate of dysphagia.
A retrospective cohort study included 80 patients who underwent Heller myotomy between January 2018 and August 2023. Sixty-four patients underwent Dor fundoplication and were 4:1 matched by age, sex, BMI, achalasia subtype, smoking status, and GERD history, with 16 patients who did not undergo Dor fundoplication. Records were reviewed for GERD, achalasia symptoms, and chest pain at 3 months, 6 months, 1 year, and 2 years postoperatively for all patients if available. Associations were investigated using chi-squared or Fisher’s exact test.
172 patients with achalasia underwent LHM with or without Dor fundoplication. Propensity matching resulted in 64 patients in the Dor group and 16 patients in the non-Dor group. Most patients (83.75%) had type 2 achalasia. At 2 to 3 weeks postoperatively, there was no significant difference in the occurrence of GERD and dysphagia symptoms between non-Dor and Dor patients. This trend continued at 3 months, 6 months, 1 year, and 2 years, with no statistically significant differences observed (Figure 1). There were no statistically significant differences between the two groups regarding postoperative chest pain or dysphagia treatment, including dilation, steroids, Botox, reoperation, and speech therapy at 2 to 3 weeks, 3 months, 6 months, 1 year, and 2 years (Figure 2). Postoperative GERD, dysphagia, and chest pain. Postoperative dysphagia treatment.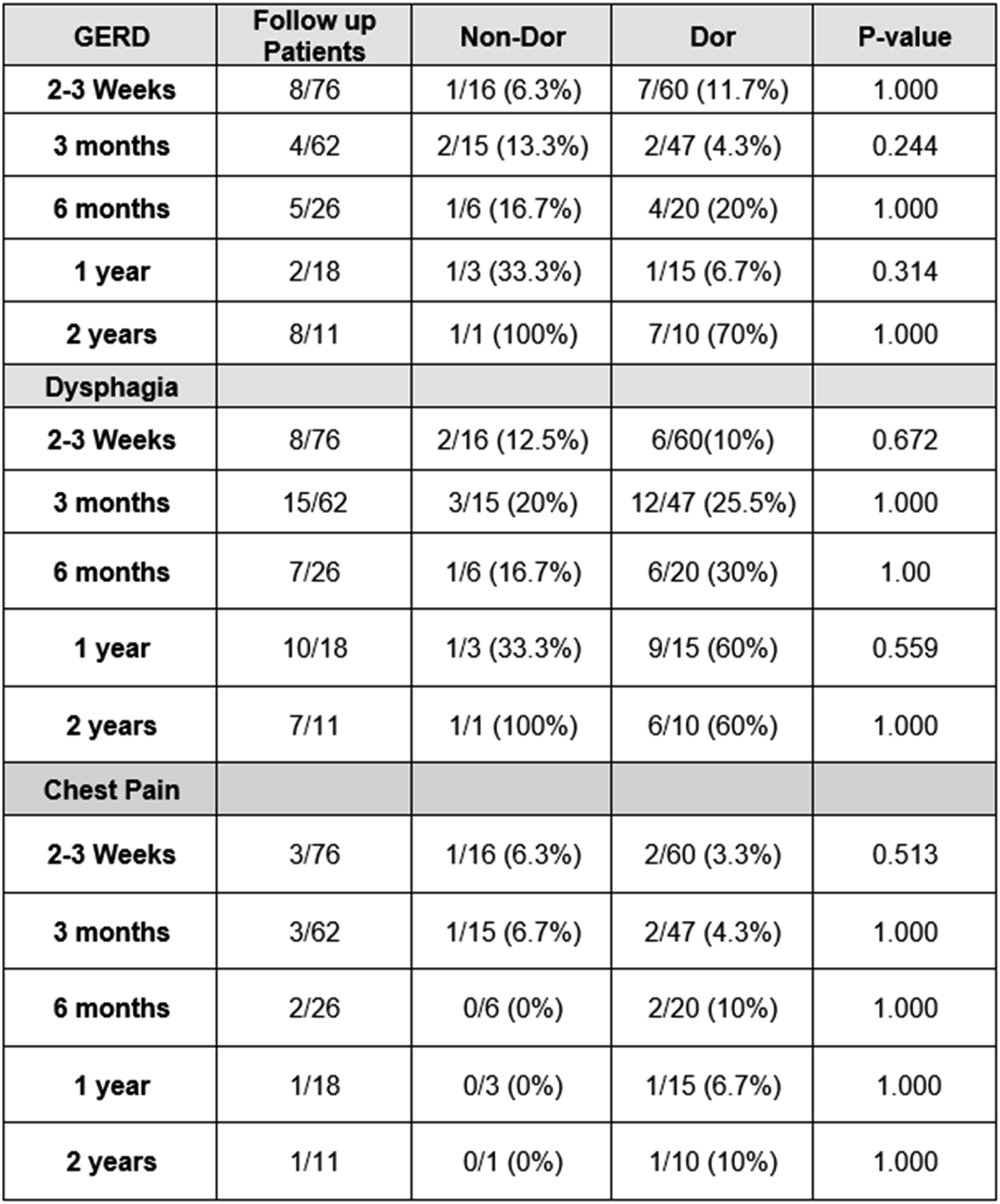
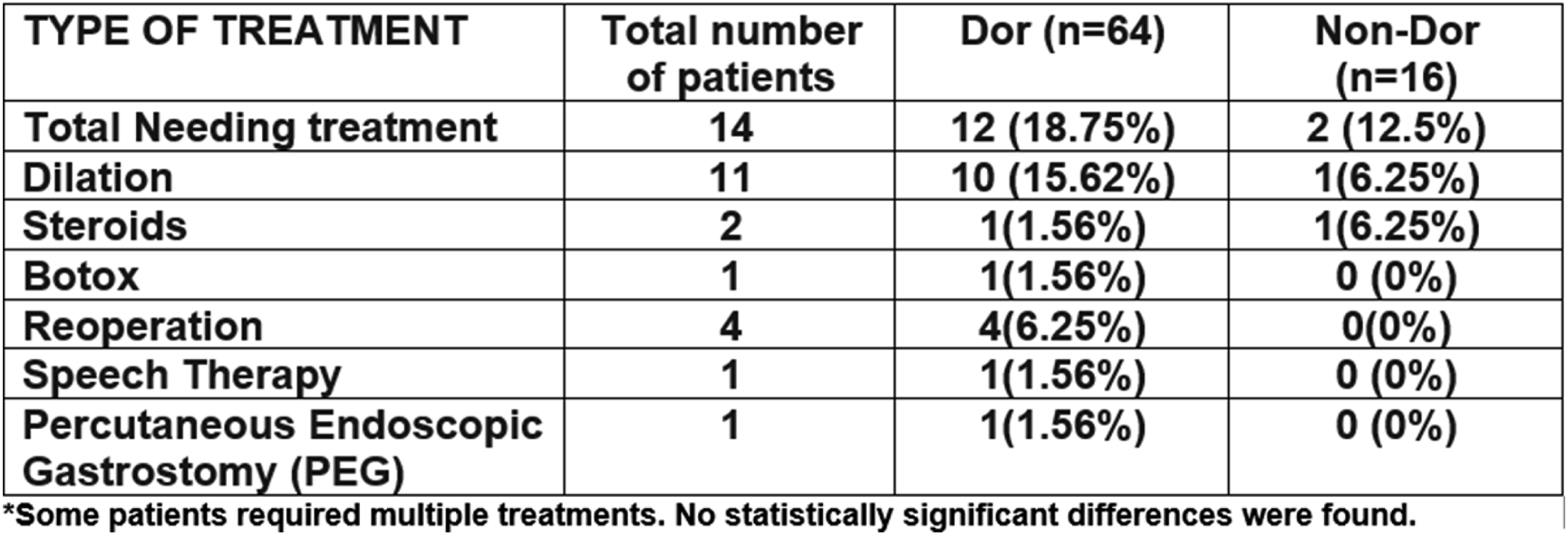
We studied patients with achalasia who had robotic HM with or without Dor fundoplication. Our findings showed no significant difference in symptoms between the groups in both short- and long-term follow-up. Heller myotomy with Dor fundoplication can improve symptoms of regurgitation and dysphagia. 3 In a study conducted by Rosemurgy et al (2018) on 135 patients undergoing LHM with Dor, there was a significant reduction in symptom severity, including dysphagia and regurgitation. 3 However, a meta-analysis found no differences in GERD symptoms between Heller myotomy and Heller myotomy with Dor fundoplication. 4 Our results suggest that adding an anti-reflux procedure to Heller myotomy did not prevent GERD symptoms or postoperative dysphagia. In terms of postoperative treatment, our study found no significant difference between the groups in terms of dilation, Botox, and steroids. The reoperation rate was also not significantly different between the groups. However, the Dor group had a higher incidence of dilation treatment and reoperation. Importantly, the Dor group experienced clinically significant dysphagia symptoms, requiring more frequent dilation and reoperation (Figure 2). Our limitations include a retrospective study design, limited available information at each follow-up, inconsistent follow-up, and a small sample size.
Our findings suggest that there is no significant difference in postoperative GERD and achalasia-related symptoms between patients who underwent Heller myotomy with or without Dor fundoplication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB statement
Study approval was provided by the University of South Florida Institutional Review Board.