
Abstract
Peritoneal adhesion is a common cause of small bowel obstruction (SBO). In this study, we included 40 adult patients who had SBO, or partial obstructive symptoms. In the abdominal instillation of crystalloid fluid (AICF) cohort, 16 patients underwent lysis of adhesions and abdominal crystalloid fluid instillation at the end of the procedure. In the control (CO) group, 24 patients received lysis of adhesions without fluid instillation. AICF was achieved by the abdominal instillation of 1864 ± 97.5 mL of crystalloid fluid. We analyzed the recurrence of peritoneal adhesions resulting in reoperation for SBO within the 64.3 ± 9.15 months of follow-up time for the CO and the 70.5 ± 13.16-month follow-up for the AICF group. The AICF group had a lower SBO recurrence rate of 12.5% compared to the CO group’s 41.6% rate (P = .049). Taken together, AICF decreased the recurrence of SBO requiring reoperation secondary to adhesion formation compared to the lysis of adhesions alone, as seen in the CO group.
Keywords
Article
Small bowel obstruction (SBO) accounts for about 15% of all surgical admissions in the United States, with a common cause: peritoneal adhesions. 1 A promising method to prevent postoperative peritoneal adhesions is the use of abdominal instillation of high-molecular-weight dextran or lactated Ringer’s (LR) solution at the end of surgery. 2 It has been shown that LR solution remains in the abdominal cavity long enough to prevent adhesion formation after a laparoscopic operation for infertility. 2
We hypothesized that the abdominal instillation of crystalloid fluid (AICF) could be beneficial in reducing postoperative peritoneal adhesion formation and the need for SBO reoperations. Institutional Review Board approval was obtained before we started this study. We analyzed a total of 40 patients with an SBO who underwent an operation for lysis of adhesions, followed by abdominal instillation of crystalloid fluid (either LR or normal saline solution) in the AICF cohort or no fluid instillation at the end of surgery in the control (CO) group. In this combined retrospective and prospective study, we included eight retrospective cases in addition to the many more prospective ones to increase the total number of participants. We chose patients who underwent a “clean” lysis of peritoneal adhesion surgery only, without any additional procedures such as enterotomies, anastomosis creation, and any abdominal malignancy. The decision regarding which patients were assigned to be a part of the AICF cohort was based on the judgment and preference of the operating surgeons.
We evaluated patient demographics, indications for surgery, and the type and amount of crystalloid fluid applied. All adhesions were graded as extensive or not extensive during surgery, which was based on the surgeon’s operative notes. Patients were followed up for at least 3 years postoperatively. Chi-square test, Fisher’s exact test and Student’s t-test were performed to compare variables in the AICF and CO cohorts, using GraphPad Prism for Windows.
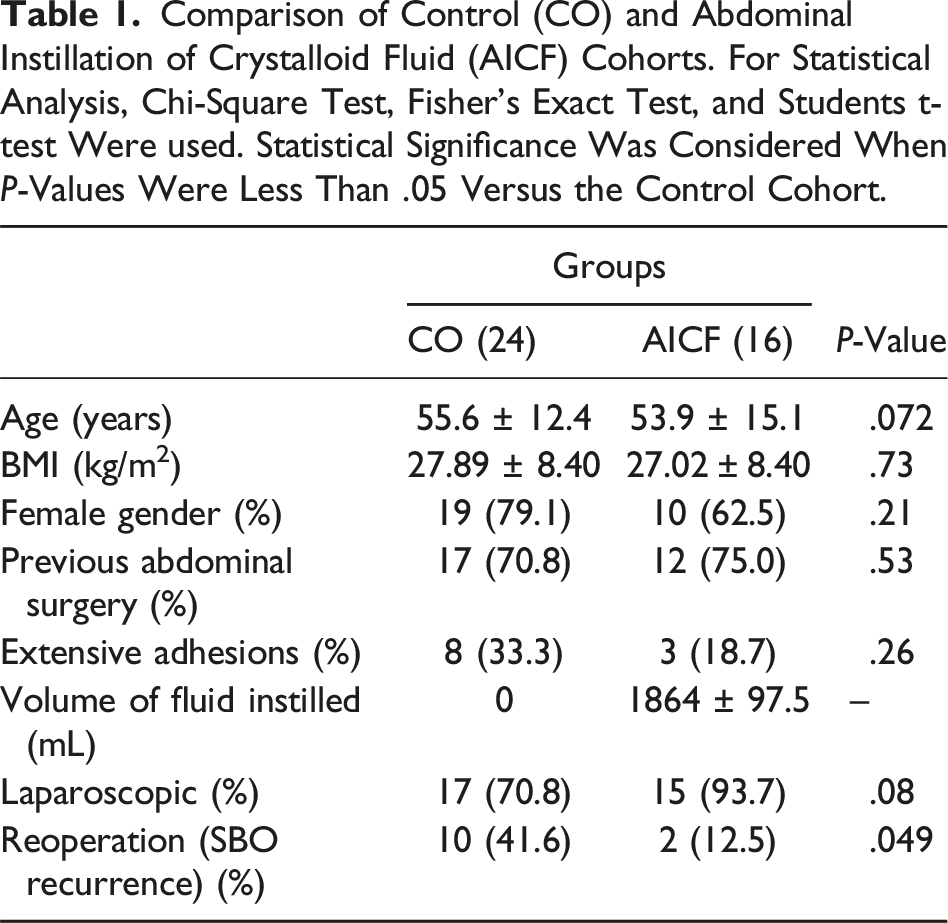
Comparison of Control (CO) and Abdominal Instillation of Crystalloid Fluid (AICF) Cohorts. For Statistical Analysis, Chi-Square Test, Fisher’s Exact Test, and Students t-test Were used. Statistical Significance Was Considered When P-Values Were Less Than .05 Versus the Control Cohort.
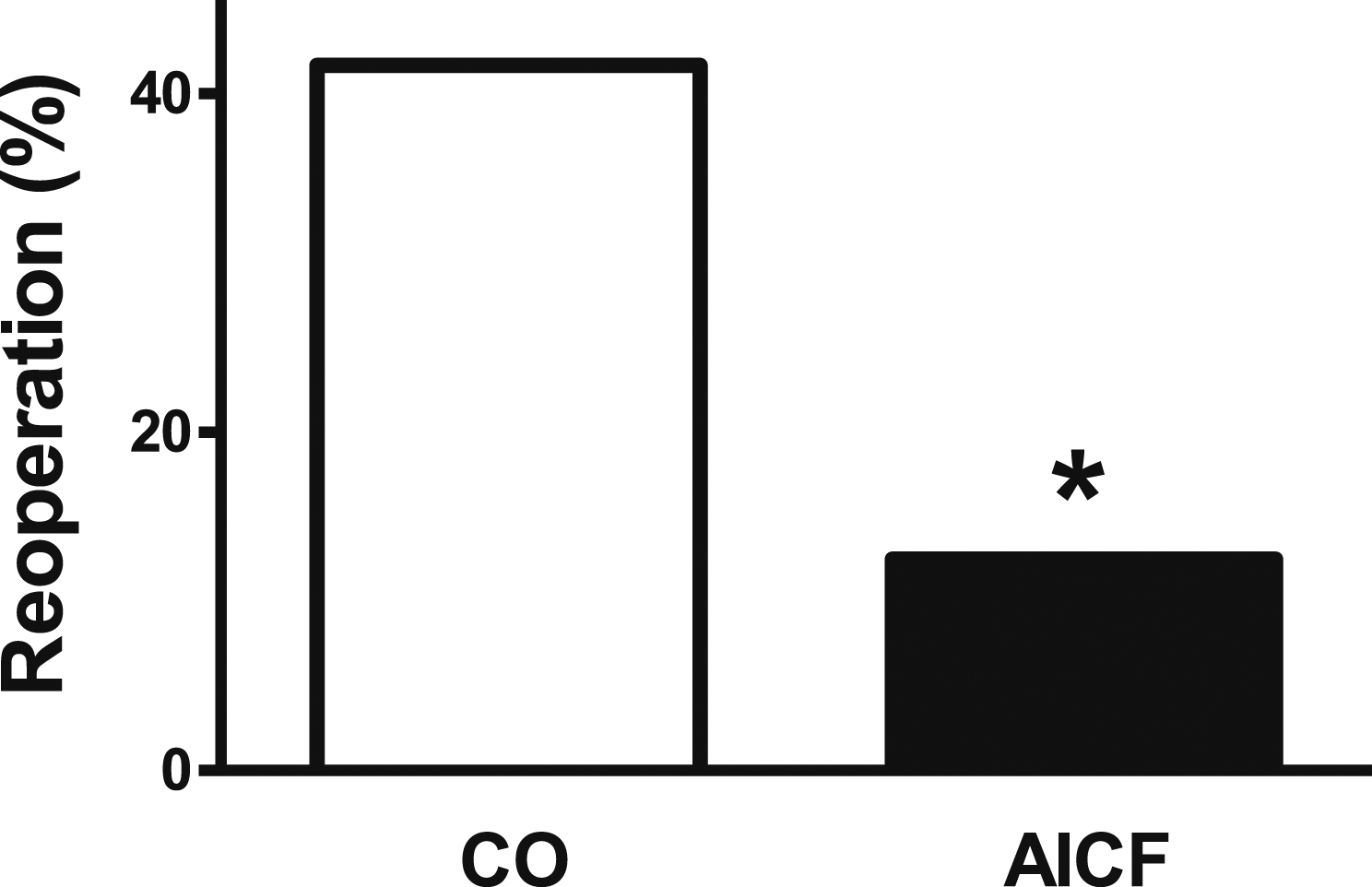
Comparison of reoperation rate for SBO from intestinal adhesions in the control (CO) and the abdominal instillation of crystalloid fluid (AICF) cohorts within 3 years after initial lysis of adhesions. For statistical analysis, chi-square test and Fisher’s exact test were performed. Statistical significance was considered when P values were less than .05 vs the control cohort (P = .049).
Patient age, gender distribution, body mass index (BMI), and previous abdominal surgery in their medical history were similar in both cohorts (Table 1). We followed the patient outcomes and documented the recurrence of peritoneal adhesions resulting in SBO within the 64.3 ± 9.15 months of follow-up time for the CO and the 70.5 ± 13.16-month follow-up for the AICF group. Regarding the extent of adhesions, the grouping of patients into the AICF or control cohorts was not based on the severity of adhesions. We believe that with higher numbers in the study, the distribution of these two levels of adhesions would have evened out better among the cohorts. In the current study, we did not see a significant indication for the possibility of direct causation between the severity of current adhesions and the future recurrence of new ones after the surgery. Adhesion recurrence was considered only when reoperation was needed for SBO caused by new peritoneal adhesions. Neither of the cohorts had any patients who received non-operative management of SBO during the follow-up time. No patients developed significant postoperative complications other than subsequent adhesions and SBO in both groups, albeit at a significantly different rate. In terms of pathology, all patients included in this study had benign adhesive diseases with no malignant SBO.
In summary, we found that AICF was associated with lower rates of postoperative SBO needing surgery again. This is in line with several reports about the adhesion-preventing benefits of hydro-flotation and abdominal fluid instillation.3-5 Particularly, after gynecological surgeries, lower rates of adhesion formation have been reported following hydro-flotation or gel agent administration.3-5 Among them, a randomized controlled trial also documented a reduction in the de novo formation of peritoneal adhesions following a postoperative intraperitoneal wash with lactated Ringer’s solution for 48 hours following myomectomy. 5 Despite the success of this inexpensive, safe, and effective treatment, it is surprising that it is not as widely used in gastrointestinal surgery as it is in gynecology. Overall, abdominal instillation of crystalloid fluid may prevent the recurrence of abdominal adhesions, which would normally require subsequent reoperations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.