
Abstract
Background
Disparities secondary to underinsurance present throughout the surgical care continuum. Community free clinics are uniquely capable to provide health care services to the medically underserved, but surgery often falls outside their scope of care.
Methods
Retrospective chart review was conducted on consecutive community free clinic patients receiving free surgical services via referral to a partnering ambulatory surgery center between March 2016 and September 2021. Those with documented contact information were recruited 1-3 years post-procedure for long-term quality-of-life (LTQOL) outcomes assessment via modified Veterans RAND 12-item health survey.
Results
Of 142 included patients, 95.7% identified as Hispanic/Latino and 75.6% were uninsured. Twelve patients had cancerous or precancerous lesions detected and/or removed through diagnostic or definitive procedures. 3.5% experienced postoperative complication including bacterial (n = 2) or fungal (n = 1) surgical site infection and wound dehiscence (n = 2). With a 48.9% response rate, no significant differences in sociodemographic or clinical characteristics were found between surveyed vs non-surveyed patients. Of surveyed patients, 59.7% and 52.2% reported pre-/post-operative improvement in physical health and emotional health, respectively.
Discussion
Free diagnostic screening procedures provided timely diagnoses while free definitive surgeries safely and positively impacted long-term patient-reported physical health. Longitudinal, multidisciplinary follow-up and social support may be warranted to concurrently improve emotional and mental health in similarly underinsured populations.
Key Takeaway
• A free clinic-ambulatory surgery center partnership is possible and benefits communities. • Our free surgery model offered greater access to diagnostic screening procedures for underinsured patients. • Patients reported improvements in physical and mental health after receiving free surgery through our model.
Introduction
Disparities in surgical outcomes may be compounded by patients’ ethnicity, medical history, and socioeconomic status. Data suggest that a significant portion of patients experience significant barriers to care including access to insurance. Of Orange County’s population, 34.1% identifies as Hispanic or Latino and has the lowest rates of insurance enrollment compared to any other demographic group in Orange County. 1 Moreover, uninsured or government-insured patients are less likely to receive surgical care in high volume hospitals compared to patients with private insurance. 2 Despite making up a substantial percentage of the population, these patients comprise a relatively smaller fraction of the throughput of surgical practices and clinics.
Diagnostic delays alongside insurance issues of access to care present important burdens of disease that are especially relevant today given the aftermath of the COVID-19 pandemic. These pose a threat to the patient’s ability to access safe and affordable care. Community free clinics are an important resource in bridging the gap in coverage and services, but surgical conditions and procedures are often beyond their scope of care, leading to delays in the provision of care and further exacerbations of underlying medical inequities. The existing literature suggests that community clinics offering cost-free surgical care to underserved populations can prevent resource-intensive hospital stays. 3
Despite these examples, there remains a tremendous unmet need to provide surgical services to minority groups with little access to care. To address this need, a local free community clinic formed a partnership with a private, Medicare-certified ambulatory surgery center (ASC) to heavily discount the use of the facility. Currently, every month, two free surgery days at the ASC in one operating room are dedicated to the uninsured. The ASC charges $6000 per month for the facility which is paid by donors. The surgeries are performed with volunteer surgeons, anesthesiologists, scrub techs, and nurses. Case numbers per day vary widely based on availability of volunteer staff and type of surgeries being done, but approximately six to eight cases are done per day.
Patients underwent the free surgery day screening and selection process at Lestonnac Free Clinic, a private, non-profit organization and comprehensive community free clinic providing primary medical, dental, and vision care to the underinsured population in the greater Orange County, California locale. To qualify for free surgery days, patients with conditions that warranted low to moderate risk elective outpatient surgery were first screened by their providers. Any patients screened as high risk based on preoperative American Society of Anesthesiologists (ASA) classification (ASA score >3) and comorbidities, such as patients with history of ischemic heart disease or cerebrovascular events, were excluded from consideration for free surgery. After screening, providers placed patients on a waitlist, where they were scheduled for their procedures at the ASC based on patient and surgical staff availability. Preoperative evaluation and planning including bowel prep was done at the clinic prior to the surgery day. Upon discharge from their outpatient procedures, these patients were typically scheduled to return to the free clinic for follow-up.
This program initially began as once every couple of months and grew to twice a month due to the high demand for surgical procedures. We sought to evaluate the clinical and quality of life impact on the patients who received surgical services through the free clinic-surgery center partnership.
Methods
Study Design and Retrospective Chart Review
Following approval by the University of California, Irvine Institutional Review Board under approval #775, retrospective chart review was conducted. Consecutive patients presenting to free surgery days at the ASC between March 2016 (when the program began) and September 2021 were identified. Patients with any ascertainable medical records were included. Primary study outcomes were self-reported quality of life measures assessed through a survey administered to patients via telephone call one to three years post-procedure. Pre- and postoperative clinical notes, surgical referral notes, procedure notes, and laboratory, imaging, and pathology report narratives were identified in paper records and the electronic health record (Brilogy Corporation, Santa Ana, CA) and reviewed for follow-up status and number of follow-up visits, significant postoperative pain (≥6 on a scale of 1-10), postoperative complications (ie, surgical wound infection or wound dehiscence), postoperative recurrence of hernia or prolapse, and revision procedures, which comprised secondary study outcomes. Independent sociodemographic and clinicopathologic study variables included age, sex, race/ethnicity, primary spoken language, insurance status, annual household income by U.S. quintiles, comorbidities (eg, type II diabetes and hypertension), ASA score, indication for referral, procedure type (ie, endoscopic, general, urologic/gynecologic, and other), time on waitlist, and pathology, if relevant. 4 National percentile and state decile Area Deprivation Index (ADI) values were determined by cross-referencing census tracts corresponding to patient zip codes to 2018 American Community Survey data.5-7
Survey of Long-Term Quality of Life Outcomes
Questions were adapted from the Veterans RAND 12-item health survey (VR-12) and the Patient-Reported Outcomes Measurement Information System (PROMIS) (see
All patients included for retrospective chart review with documented telephone contact information were approached for survey participation by one of three bilingual English- and Spanish-speaking members of the study team. Those responsive within three contact attempts, each with intentional variation by time of day and day of the week, were appropriately consented and included for survey study. Patients who were not responsive to contact after three attempts were considered nonresponders.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics software version 28.0.0.0 (IBM Corporation, Armonk, NY) and P-values <.05 were considered statistically significant. Categorical data were reported as percentages, and continuous data were reported as means ± standard deviation. Relative equivalence of the surveyed and non-surveyed cohorts was assessed by independent samples t-tests and chi-square tests applied, respectively, to continuous and categorical demographic and clinical variables.
Results
Patient Selection and Survey Response
A total of 154 patients were identified as having received at least one free surgical procedure through a referral from the free clinic between March 2016 and September 2021. Medical records could not be located for twelve of these patients. As such, 142 patients were deemed eligible for retrospective chart review and surveying. Of these 142, five patients lacked documented contact information; as such, contact was attempted for a total of 137 patients, with 67 successfully completing the survey within three attempts, leading to a 48.9% response rate (Figure 1). Flowchart of patients included in Quality of Life analysis.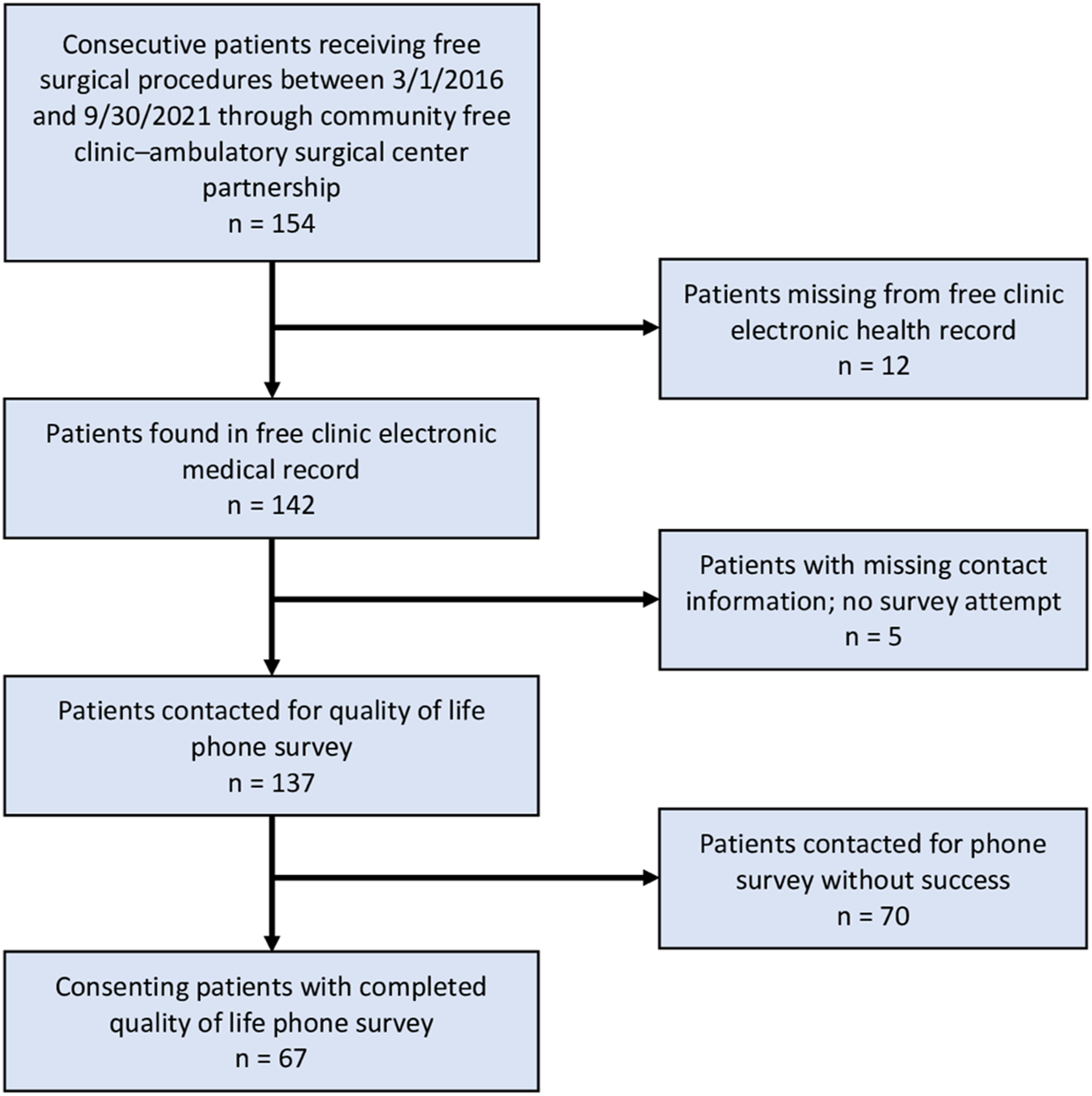
Our patient population had an average age of 52.2 ± 9.3 years and consisted of 57.0% female patients, 95.7% who identified as Hispanic/Latino, 89.2% primarily Spanish-speaking patients, and 75.6% uninsured patients. Out of our total patient cohort, 24.4% had government insurance, but these patients were primarily covered under California emergency Medicaid which does not give them access to outpatient or specialty services. Mean ADI was 24.6 ± 20.1 by national percentile and 6.4 ± 2.0 by state decile.
Relative Baseline Equivalence of Free Surgery Day Patient Demographics and Clinical Characteristics by Survey Completion Status (n = 142).
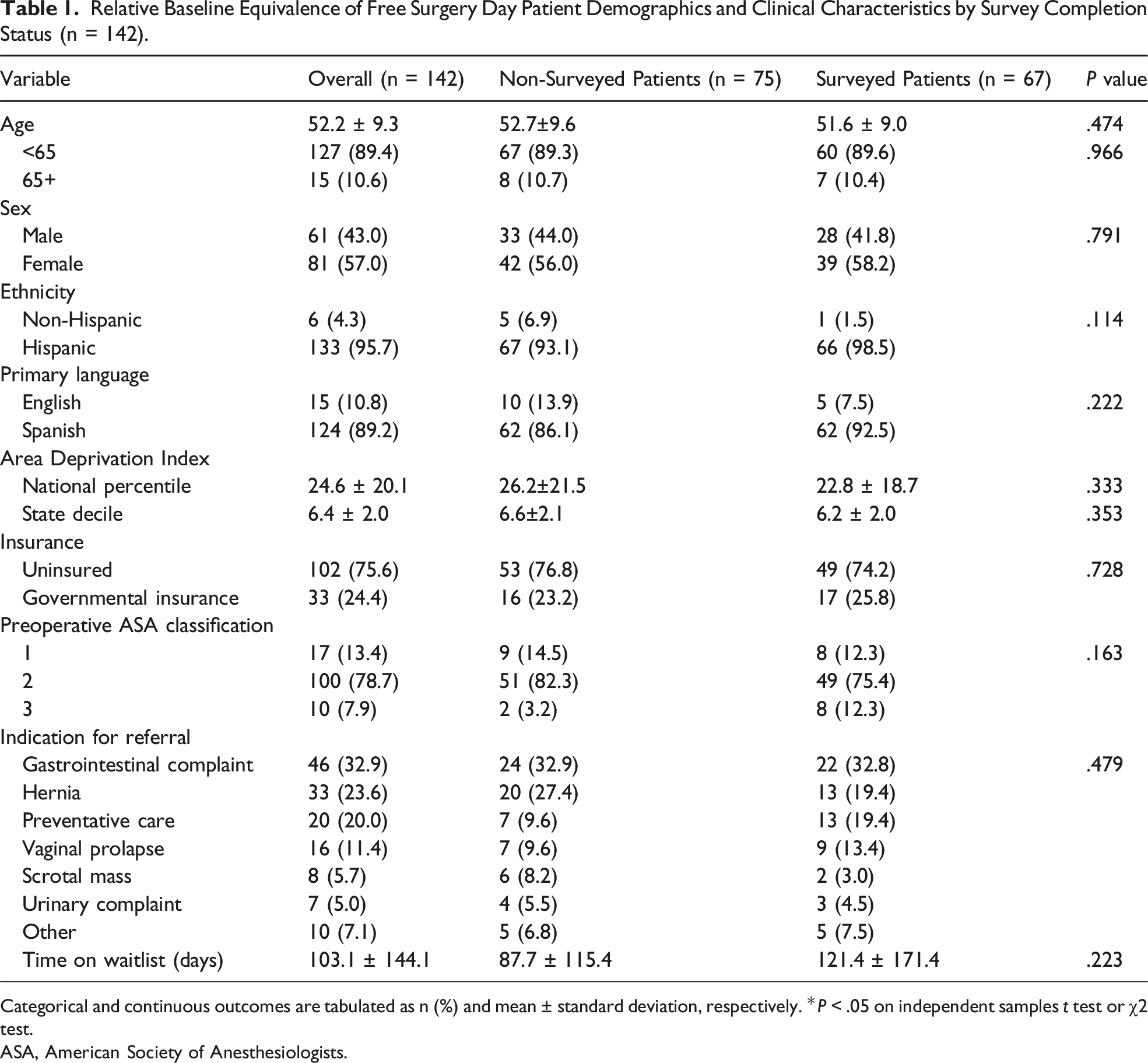
Categorical and continuous outcomes are tabulated as n (%) and mean ± standard deviation, respectively. *P < .05 on independent samples t test or χ2 test.
ASA, American Society of Anesthesiologists.
Retrospective Chart Review
Of 142 total procedures, 66 were endoscopic, 36 were general surgery, 35 were urologic/gynecologic, and 5 were classified as other types, including ophthalmologic and orthopedic procedures. The most frequent endoscopic procedures performed were isolated colonoscopy (74.2%, 49/66), concurrent esophagogastroduodenoscopy (EGD) and colonoscopy (15.2%, 10/66), and isolated EGD (10.6%, 7/66). Within the general surgery category, inguinal hernia repair was the most common procedure (55.6%, 20/36), followed by abdominal hernia repair (27.8%, 10/36). Colporrhaphy (54.3%, 19/35), cystoscopy (20.0%, 7/35), and scrotal mass excision (20.0%, 7/35) comprised the predominant urologic/gynecologic procedures. The Other category encompassed miscellaneous procedures including pterygium excision, total knee replacement, and total hip replacement.
All Procedures Performed During Free Surgery Days and Pathological Findings (n = 142).
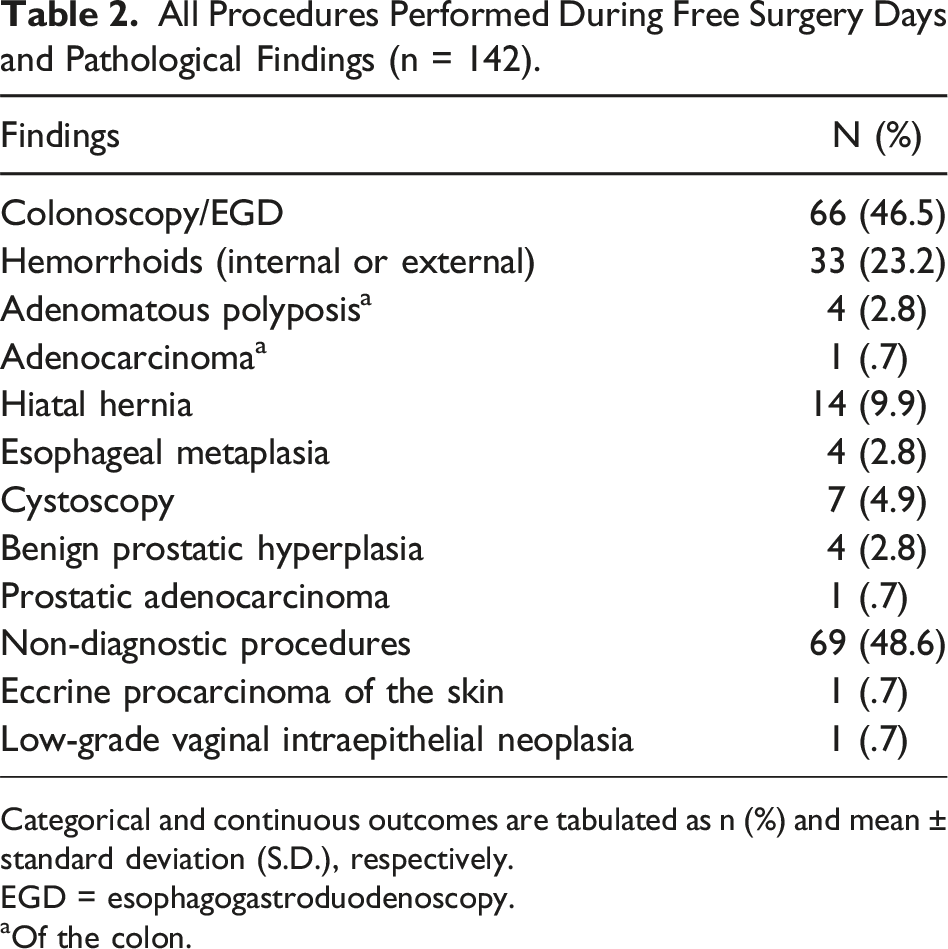
Categorical and continuous outcomes are tabulated as n (%) and mean ± standard deviation (S.D.), respectively.
EGD = esophagogastroduodenoscopy.
aOf the colon.
Patient-Reported Postoperative and Long-Term Quality of Life Outcomes
Overall Postoperative Outcomes in the Free Surgery Day Patient Population (n = 142).
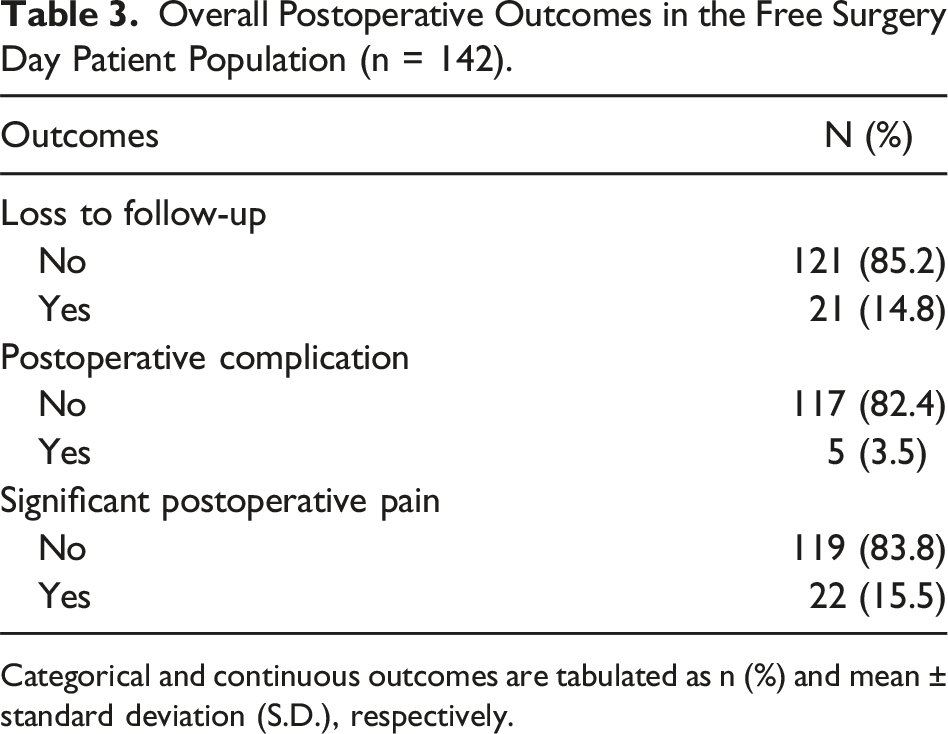
Categorical and continuous outcomes are tabulated as n (%) and mean ± standard deviation (S.D.), respectively.
Free Surgery Day Patient-Reported Long-Term Outcomes According to Survey Responses (n = 67).
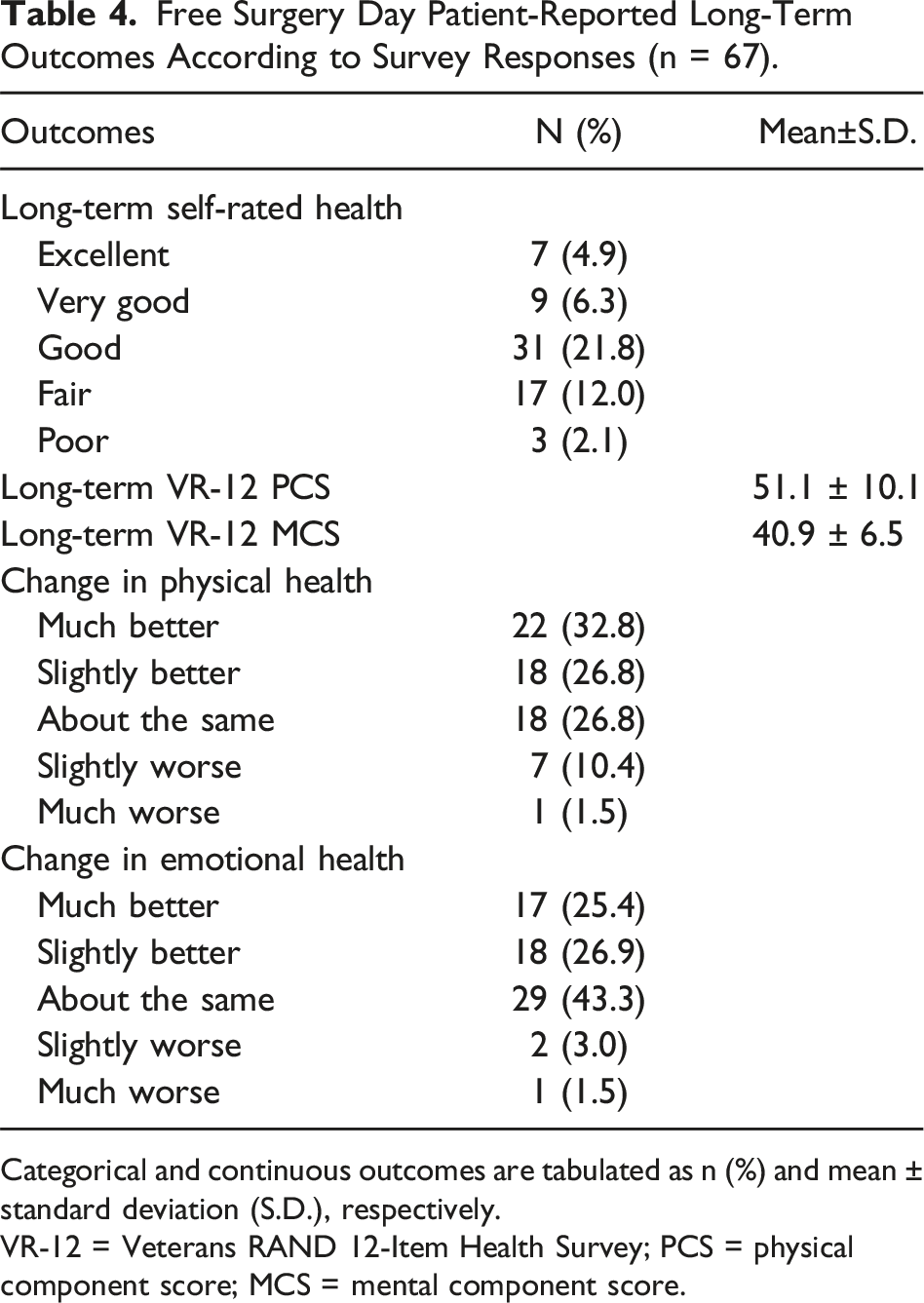
Categorical and continuous outcomes are tabulated as n (%) and mean ± standard deviation (S.D.), respectively.
VR-12 = Veterans RAND 12-Item Health Survey; PCS = physical component score; MCS = mental component score.
Discussion
This single center, retrospective study found that a surgical center-free clinic partnership providing free surgical services effectively improved surgical access in an underinsured population. In this study, we apply a mixed PROMIS and VR-12 adapted survey model to quantify the impact on patient physical and emotional health after a variety of surgical procedures facilitated in a free clinic setting. We chose these tools because past studies have demonstrated that scores derived from the PROMIS and VR-12 are valid in accurately measuring patient-reported outcomes in various surgical contexts, and the two scores are associated and able to be linked.14,15
Overall, patients benefited from enhanced quality of life after receiving procedures through this free surgery model, though with greater rates of self-reported improvement in physical health components compared to measures of emotional problems. Patients also reported overall postoperative LTQOL scores via VR-12 PCS and MCS comparable to those endorsed by the general US population. 15 Previous studies have reported that lower physical and emotional health scores on the PROMIS survey are predictive of increased hospitalization risk. 16 Considering that most of our patient cohort consisted of un- and underinsured individuals, the similarity in self-reported quality of life measures to national scores after free surgery is especially notable. This may suggest that hospitalization risk for these patients was similar to that of the general, healthy population, which is critical for low-income, under-resourced patients who may be vulnerable to catastrophic health expenditure.
In our surveyed patient cohort, there was a trend to an improvement in emotional health, but impact on emotional health was less remarkable than the impact on physical health. Pre-procedure, baseline MCS was not measured, thus the change in MCS after procedures could not be easily quantified. However, the post-procedure long-term MCS was less than long-term PCS and less than that of the general population. The lack of considerable improvement in emotional health after surgery could be due to pre-existing stressors, which are known to be elevated in patients of lower socioeconomic status, and likely largely unaddressed in our patient cohort. 17 Furthermore, the uncertainty of a diagnosis especially if the patient has symptoms may cause undue stress and impact the daily emotional health of the patients. Additionally, previous literature has reported that the uninsured have disproportionate lack of access to mental health services compared to the insured patient population. 18 These findings are consistent with our study population, and further research is necessary to elucidate possible modifications that could be enacted in the free surgery model to improve patient satisfaction, perhaps including longitudinal and multidisciplinary follow-up and patient navigation for referral to additional social and community resources.
An especially notable finding in our study was that free surgery had a low overall morbidity (3.5%) despite a presumed lack of resources. The morbidity rate of our free surgery model was comparable to, if not less than, the national morbidity rate for elective general surgery procedures (6.7%). 19 This could be attributed to the involvement of skilled nursing and anesthesiology personnel on-site at the ambulatory surgery center, which is a privilege that not many surgical centers in under-resourced settings have access to. However, the patients in our study were also screened before their procedures for any comorbidities that may place them at significant risk for complications for outpatient surgery, and patients deemed high risk by their providers were not eligible to be placed on the free surgery waitlist. This was due to the lack of ability to admit patients at the surgery center postoperatively if they were to have any complications. Thus, only low to moderate risk patients had surgery at the surgery center, and this may have introduced some potential for selection bias in reporting complication rates. Access to anesthesiology and perioperative care may have positively influenced patient satisfaction in our free surgery model as well, leading to better patient follow-up and complication prevention. Thus, patient perceptions of the availability of these services in under-resourced areas warrants further study. Nevertheless, this finding supports the notion that our current free surgery model is safe for elective low and moderate risk procedures and does not place otherwise marginalized patients at greater risk of morbidity or mortality.
The diagnostic procedures that were performed yielded critical pathological findings sensitive to timeliness including cases of dysplasia, metaplasia, and carcinoma. A total of twelve patients had precancerous or cancerous lesions detected and/or removed during these procedures. Diagnostic procedures are not only financially burdensome for uninsured patients, but they are also difficult to access, especially if these patients are not receiving routine medical care. Most notably, cancer screening rates are lower in un- and underinsured patient populations, and these patients are more likely to be diagnosed with advanced-stage solid cancers. 20 Our study suggests a free surgery model may help address this disparity by increasing access for diagnostic procedures that patients may have otherwise not received. Future cost-benefit analyses for free surgery costs compared to long-term patient health savings may be useful to determine the cost-savings impact of free surgery, especially diagnostic procedures, for uninsured patients navigating the current health care system in the US. Most notably, access to diagnostic screening for cancer in the uninsured is necessary as it can improve outcomes from cancer. For example, colorectal cancer or precancerous lesions can be cured with early detection and treatment but cannot be addressed if they are not diagnosed. Furthermore, as the free clinic is now performing fecal immunochemical tests (FIT) as a screening tool, access to the more sensitive and specific colonoscopy is warranted to evaluate for and possibly treat colorectal cancer.
Our study is not without limitations. Due to our study being a retrospective study, it lacks granularity in many aspects such as clinical details, laboratory values, and individual patient experiences with the free surgery model. As mentioned previously, extensive screening requisites for free surgery eligibility may have introduced a degree of selection bias into the clinical outcomes of the model. Additionally, the relatively small patient population included in our single center study and high number of missing records (n = 12) limits generalizability of this study. Also, this model may not be easily replicated in other areas, such as in communities that lack the adequate resources to provide free services at an ambulatory surgical center. Follow-up rates to assess for complications as well as phone survey response rates were also relatively low, so our results may not accurately represent the target patient population. The phone-facilitated survey introduced the possibility of response bias, in which patients with stronger opinions about their surgeries were more likely to respond to the survey, possibly skewing our results. This is especially notable with our survey response rate of less than 50%. Additionally, it is important to note that many of the patients receiving care at the free clinic may be of undocumented immigration status, which could have contributed to a lower phone survey response rate if undocumented patients were wary to disclose personal information in caution against punitive action.
Conclusion
In conclusion, this study represents a description of the impact of free surgery for the underinsured populations in the US. With a free clinic-ambulatory surgery center partnership model, access to diagnostic screening procedures provided timely diagnoses of conditions, especially cancers, that may abrogate advanced disease with earlier detection. Additionally, free definitive surgeries, such as hernia repairs, safely and positively impacted long-term patient-reported physical health. Additional studies are warranted to further analyze the feasibility of enacting similar models in other under-resourced populations of different sociodemographic makeup as well as possible areas for improvement in the current model. Longitudinal and multidisciplinary follow-up and social support may be warranted to concurrently improve emotional and mental health in similarly underinsured populations of surgical patients.
Supplemental Material
Supplemental Material - Surgical Care Through a Community Free Clinic-Ambulatory Surgical Center Partnership
Supplemental Material for Surgical Care Through a Community Free Clinic-Ambulatory Surgical Center Partnership by Flora S. Park, Jonathan C. Pang, Christopher D. Yang, Dalia Breziner, Karlos O. Manzanarez-Felix, Juan Pablo Hoyos, Andres M. Ruiz, Claudia A. Alvarez, Lourdes Y. Swentek, and Theresa L. Chin in American Surgeon
Footnotes
Acknowledgments
Thank you to the staff and Board of Directors of the Lestonnac Free Clinic in Orange, CA for providing access to surgical care of the uninsured. Thank you to the American Los Angeles Physicians of Indian Origin (ALAPIO) and the Sarva Mangal Family Trust for the generous funding for the free surgery days. Thank you to the Beverly Hills Surgery Center for the partnership that makes free surgery days possible. Thank you to Dr. Nitin Shah who is responsible for the coordination of the free surgery days.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Theresa L. Chin reports her current position as an unpaid volunteer physician member of the Lestonnac Free Clinic Board of Directors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.