
Abstract
Objectives
Patients with peripheral artery disease (PAD) often require treatment with open lower extremity revascularization (LER). Patients with PAD often have other comorbidities and associated conditions that affect procedural outcomes, including abdominal stomas. The aim of this work is to investigate the impact that stomas may have on postoperative outcomes and complications.
Methods
We performed a 5-year (2016-2020) analysis of the Nationwide Readmission Database. We identified all adult patients undergoing open LER. These patients were categorized into 2 groups: stoma and no-stoma. Propensity score matching (1:1) was used to control for demographics and comorbidities. Index admission outcomes and readmission rate were examined.
Results
212,275 open LER patients were identified. A matched cohort of 3088 patients (1:1 stoma vs no-stoma) was obtained. Patients with stomas had higher rates of several postoperative complications: acute posthemorrhagic anemia (29.1%, P < 0.01), acute kidney injury (21.4%, P < 0.001), index sepsis (10.3%, P < 0.001), and index SSI (2.8%, P < 0.001). There were no significant statistical differences between the 2 groups for acute myocardial infarction. Those with stomas had worse outcomes: greater in-hospital mortality (4.7%, P < 0.05), length of stays (median 7 days, P < 0.001), total charges (median 108,037 dollars, P < 0.001), discharges to long-term care facilities (30.8%, P < 0.001), discharges to their own homes needing home health care (30.1%, P < 0.001), 30-day readmission rates (23.2%, P < 0.01), and 30-day readmission mortality (6.1%, P < 0.01).
Conclusions
Concurrent abdominal stoma is associated with increased postoperative morbidity and mortality after open LER. Further prospective studies are needed to validate these results.
Keywords
Background
Peripheral artery disease (PAD) affects between 8 and 12.5 million persons in the United States, and greater than 200 million people worldwide. 1 PAD is responsible for significant morbidity and mortality as the crude 5-year death rate following diagnosis is 33.2%—a rate of 82.4 deaths per 1000 patient years (PY). 2 Mortality and surgical site infection (SSI) following open lower extremity revascularization (LER) have been characterized as clinically significant in several studies.3-7 Studies have yet to investigate these outcomes in patients who have concurrent abdominal stomas (gastrostomy, ileostomy, or colostomy).
It is known that PAD and conditions leading to stoma placement such as colorectal cancer share common comorbidities such as age, hypertension (HTN), hyperlipidemia (HLD), obesity, type 2 diabetes mellitus (DM), and tobacco smoking.8-17 Given that (1) the US population is aging (leading to increased prevalence in PAD), 18 (2) 750,000 people in the US live with ostomies, and (3) 130,000 ostomies are created each year 19 —a dedicated study is needed to examine the associations and impacts that these conditions have on one another. To our knowledge, there is currently no published data that details the incidence and prevalence of PAD in patients with concurrent abdominal stomas.
The present study aimed to evaluate postoperative complications and outcomes following open LER in patients with abdominal stomas focusing on index admission sepsis, index admission SSI, index admission mortality, index length of stay (LOS), index total charges, index patient disposition, 30-day readmission rates, and 30-day readmission mortality. We hypothesize that those with stomas will have greater rates of these complications and outcomes.
Materials and Methods
Data Collection
The Healthcare Cost and Utilization Project (HCUP) is one of the largest collections of hospital care data in the United States. HCUP Nationwide Readmission Database (NRD) data includes 30 geographically dispersed states, accounting for 62% of the total U.S. resident population, and 60% of all U.S. hospitalizations. 20 HCUP diagnosis and procedure information was coded by The International Classification of Diseases 9th edition Clinical Modification (ICD-9-CM) before 2016, and a new version of coding system ICD-10-CM was applied into HCUP in 2016. In this retrospective study, we utilized the most recent 4-year release (2016-2019) of NRD database, which will avoid code transformation bias/inaccuracy between ICD-9-CM and ICD-10-CM.
In NRD database, all admission records are de-identified. Given this, researchers are not privy to patients’ identifiable data. As such, this study was exempted from Institutional Review Board approval. Demographic information of patients’ admission records, including age, gender, length of stay, days between each admission, primary payer (Medicare, Medicaid, private, others), household income (median household income for patient’s ZIP code), and disposition after hospitalization (Routine/home, transfer to rehab facility, and home health care) were collected. Hospital characteristics included bed size and ownership (private, public, and governmental). Diagnosis and procedure information including ICD-10-CM diagnosis and ICD-10-PCS procedure codes, Diagnosis Related Group (DRG) codes, and Major Diagnostic Category (MDC) codes were analyzed in this study. Coding criterion from Charlson Comorbidity Index (CCI) comorbidity measures were applied to determine the patients’ comorbidity index. 21 Specific codes related to patient identification, comorbidities, and complications are provided in Supplemental Table 1.
Patient Selection
Pre-Match Characteristics of the Study Sample.
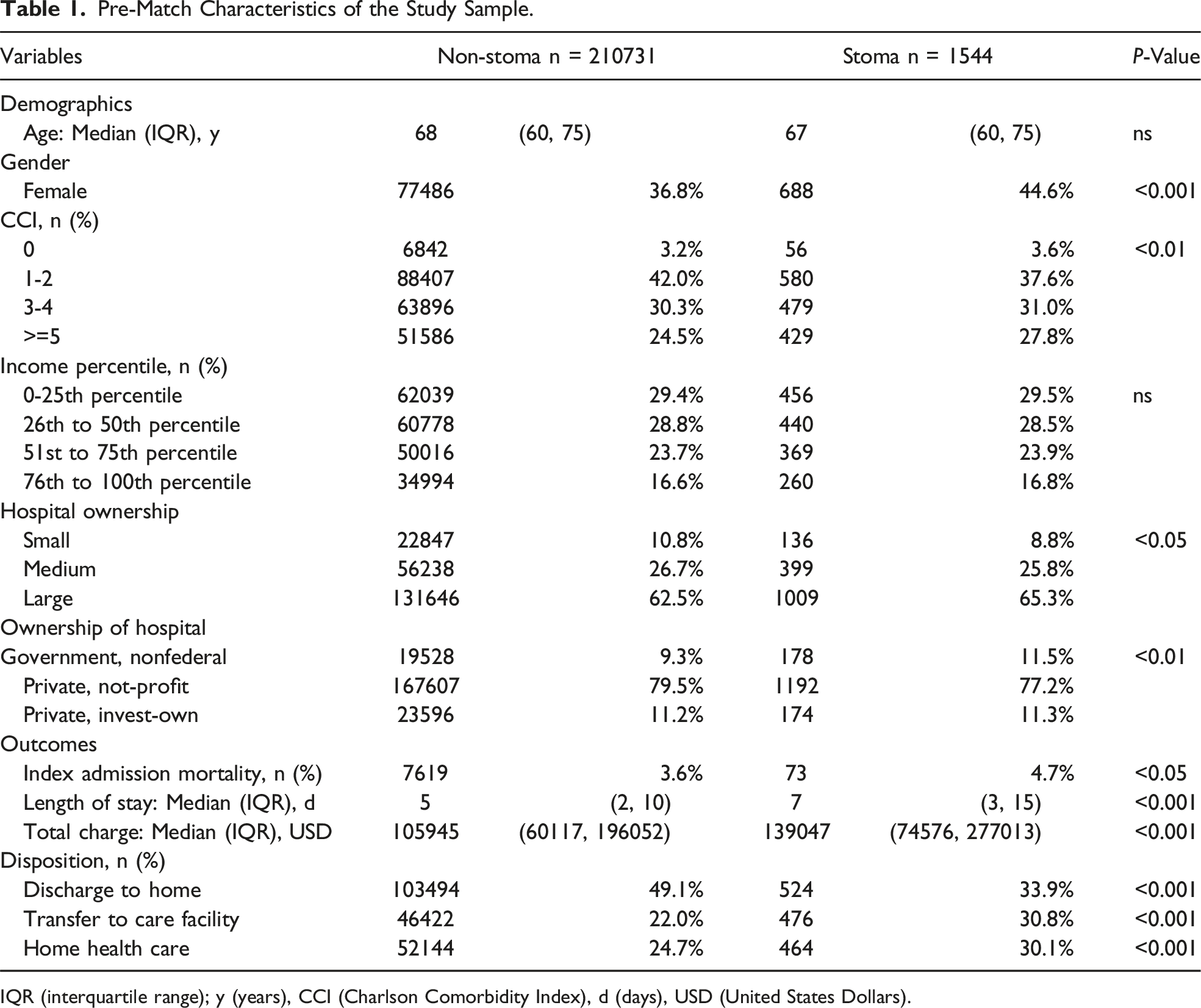
IQR (interquartile range); y (years), CCI (Charlson Comorbidity Index), d (days), USD (United States Dollars).
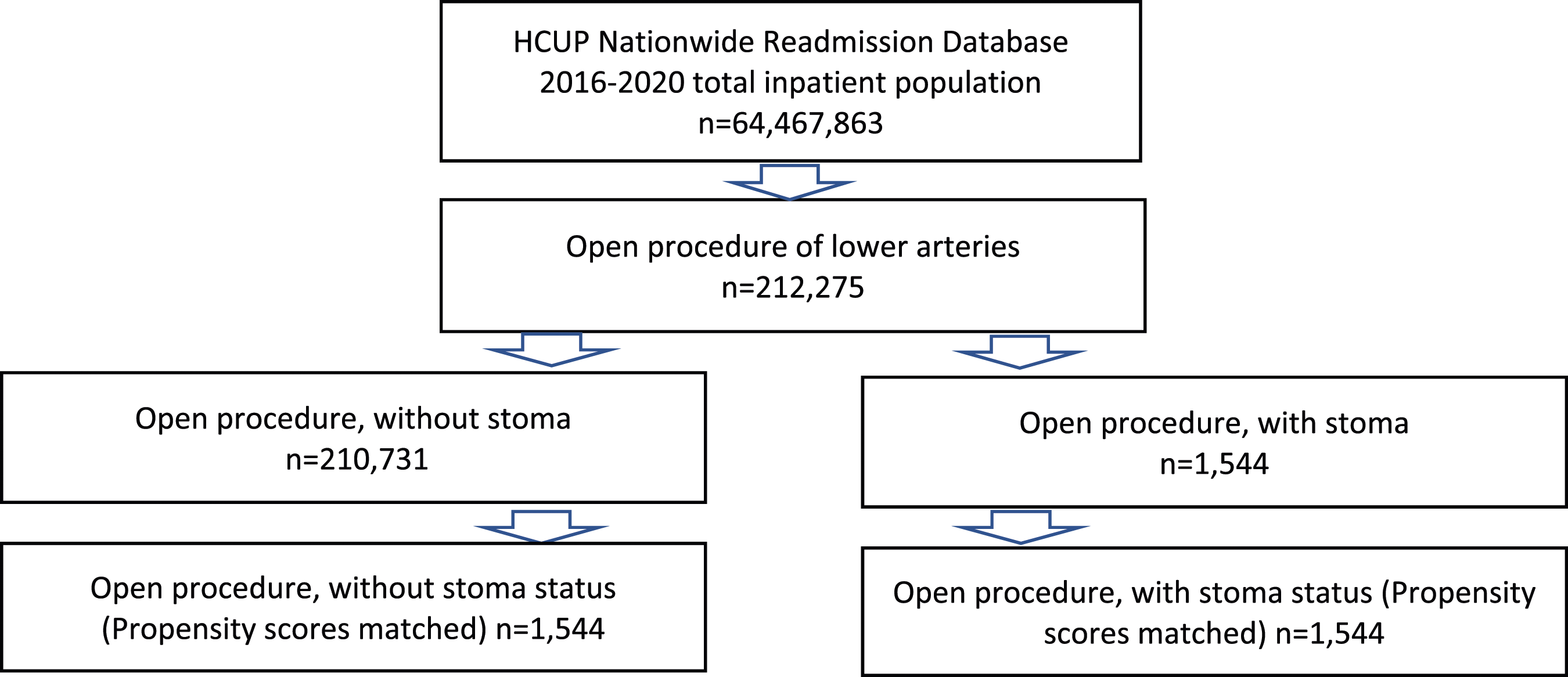
Diagram of candidate selection and study design.
Post-match Characteristics of the Study Sample.
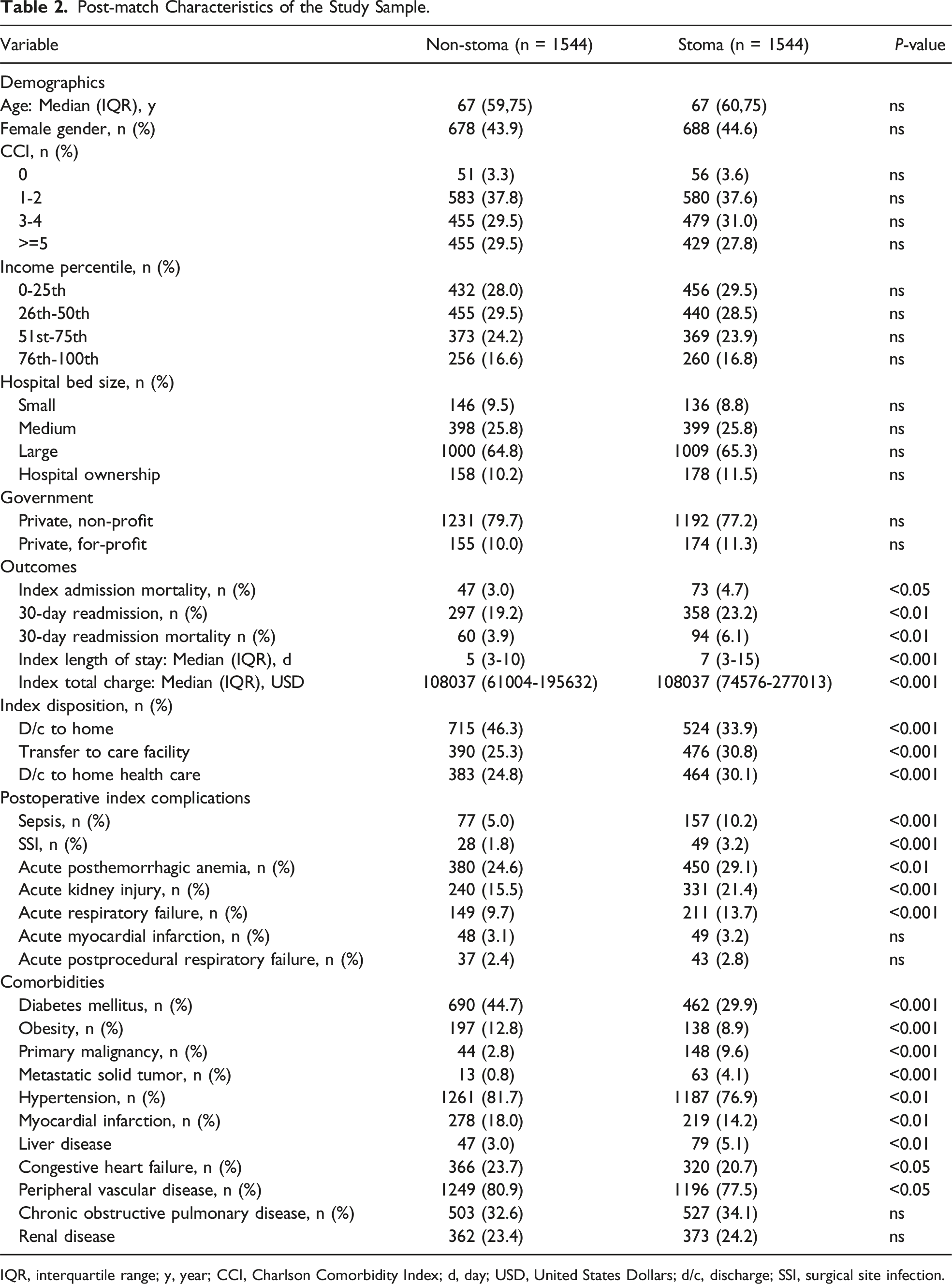
IQR, interquartile range; y, year; CCI, Charlson Comorbidity Index; d, day; USD, United States Dollars; d/c, discharge; SSI, surgical site infection.
Statistical Analysis
All analysis was performed by statistical software SPSS and R. Database related work was done by SQL under “sqldf” R package. Histogram of readmission data was made by R. The numerical variables age, LOS, and total charge were described by median and interquartile ranges (IQR) due to the fact that these variables were not normally distributed. The differences between those with stomas and those without stomas were analyzed by Wilcoxon signed-rank test without assumption of parametric distribution. Total charges at time of patients’ discharge from each year have been adjusted to the Consumer Price Index (CPI) for medical care cost of 2021 before analysis. Binary variables including gender, comorbidities, and complications status were analyzed by chi-square test. Data pertaining to CCI, household income, disposition, and hospital characteristics were analyzed by chi-square test for independence. For all statistical tests in this study, P < 0.05 is deemed to be significant.
Results
General Population Demographics and Characteristics
A total of 212,275 patients underwent an open LER procedure from 2016-2020, while 1544 patients had a concurrent abdominal stoma (Table 1 and Figure 1). The concurrent stoma group (1544 patients) was matched to a group of patients without a stoma (1,544) using propensity scores. No statistically significant differences were found between the 2 groups for any of the demographic categories: age, biological sex, CCI, income, bed size of hospital, or ownership of hospital (Table 2).
Index Surgical Complications Between the Two Groups
Following open LER procedures, those with stomas had higher rates of sepsis (10.2%, P < 0.001), and SSI (3.2%, P < 0.001). They also had higher rates of acute post-hemorrhagic anemia (29.1%, P < 0.01), acute kidney injury (AKI) (21.4%, P < 0.001), and acute respiratory failure (13.7%, P < 0.001). There were no significant statistical differences between the 2 groups for acute myocardial infarction, and acute post-procedural respiratory failure (Table 2).
Surgical Outcomes Between the Two Groups
Index admission mortality (4.7%, P < 0.05) and 30-day readmission mortality (6.1%, P < 0.01) were statistically significantly different as patients with a concurrent stoma had mortality rates. Those with stomas also had greater 30-day readmission rates (23.2%, P < 0.01), greater index LOS (median 7 days, P < 0.001), and index total charges (median 108,037 dollars, P < 0.001). Those with stomas had higher index rates of transfer to long-term care facilities (30.8%, P < 0.001) and higher rates of discharge to their own homes needing home health care (30.1%, P < 0.001), while those without stomas had higher rates of discharge to their own homes without the need for home health care (46.3%, P < 0.001) (Table 2).
Comorbidities between the Two groups
Those without stomas had a higher rate of certain key comorbidities than those with stomas. Those without stomas had higher rates of DM (44.7%, P < 0.001), obesity (12.8%, P < 0.001), HTN (81.7%, P < 0.01), peripheral vascular disease (PVD) (80.9%, P < 0.05), myocardial infarction (MI) (18.0%, P < 0.01), and congestive heart failure (CHF) (26.8%, P < 0.05). Those with stomas had higher rates of primary malignancy (9.6%, P < 0.001), metastatic solid tumor (4.1, P < 0.001), and liver disease (5.4%, P < 0.01). There were no significant statistical differences between the 2 groups for chronic obstructive pulmonary disease (COPD), and renal disease (CKD) (Table 2).
Discussion
The results of this study demonstrate that patients undergoing open LER procedures with concurrent abdominal stomas have more significant surgical complications and worse outcomes in comparison to patients without stomas. The evidence provided in this study demonstrates that patients with concurrent stomas had higher rates of index admission sepsis, SSI, AKI, acute post-hemorrhagic anemia, and acute respiratory failure. Those with stomas also had higher rates of index and 30-day readmission mortality, 30-day readmissions, index dispositions to long-term care facilities, index greater LOS, and index total charges in comparison to those without stomas.
To the best of our knowledge, there has not been a prior study that directly compares outcomes dependent on abdominal stoma status in patients being treated with open LER. Liang et al 22 authored the most recent retrospective analysis (2011-2015) of the American College of Surgeons’ (ACS) National Surgical Quality Improvement Program (NSQIP) database pertaining to open LER, which found that the index SSI and mortality rates for patients undergoing open LER for claudication are 1.5% and 0.3%, respectively, while they are 3.2% and 1.4% for patients with chronic limb threatening ischemia (CLTI), respectively. These rates differ from our index SSI and mortality rates for patients with stomas (2.8% and 4.7%). The rate of index sepsis for the stoma group was 10.3%, which likely contributed to this increased mortality. We are not able to compare the index sepsis rate of our study participants to Liang et al’s participants as they did not separately report index sepsis rates.
One possible explanation for the increased index SSI and mortality rates in our stoma cohort is that the bacteria associated with the abdominal cavity (predominantly gram-negatives and anaerobes) 23 differ from that of the skin (predominantly gram-positives). 24 While the incision sites of those being treated with open LER may typically be subjected to mostly gram-positive bacteria, those with synchronous stomas may be subjected to gram-positives and gram-negatives. Infections resulting from gram-negatives are typically more difficult to treat as the outer membrane layer of their cell wall confers resistance to a wide range of antibiotics that are effective for gram-positives (given their lack of an outer membrane layer), most notably the beta-lactams and vancomycin. 25 Carbapenem-resistant gram-negatives, including the Enterobacteriaceae family, are recognized by the World Health Organization (WHO) as a global health problem, and they are currently priority 1 (critical) pathogens for research and development of new antibiotics. 26 Physicians treating open LER patients with SSIs and synchronous stomas should consider both gram-positive and gram-negative coverage pending susceptibility testing.
One unexpected finding that we came across was that several of the comorbidities we examined were more frequent in patients without stomas in comparison to patients with stomas. We believe our matching methodology (and thus our study) is valid given that there were no statistically significant differences between our stoma and non-stoma cohorts for demographic categories (age, gender, income, CCI, hospital bed size, and hospital ownership) following matching analysis (Table 2). The CCI 27 predicts 10-year mortality using age and several comorbidities: MI, CHF, PVD, cerebrovascular accident/transient ischemic attack (CVA/TIA), dementia, COPD, connective tissue disease, peptic ulcer disease (PUD), liver disease, DM, hemiplegia, severe to moderate CKD, primary solid malignancy, leukemia, lymphoma, metastatic solid tumor, and AIDS. All of the comorbidities in Table 2 are found within the CCI excluding HTN and obesity. Patients were matched according to their index totals, and no comparison between the 2 cohorts for index total (0, 1-2, 3-4, and >5) was found to be statistically significant. The most common conditions leading to stoma formation include cancer, inflammatory bowel disease (IBD), and diverticular disease. 28 Given the CCI, cancer was factored into matching.
This study has a few notable limitations. First, the study is retrospective and is subject to selection bias. Second, patient selection is dependent on procedural and diagnostic codes, which are subject to coding and reporting biases. Third, the NRD does not include race or clinical information regarding medications, laboratory values, and imaging findings, which are important considerations in patient outcomes. Fourth, the use of the CCI also has its limitations. While it does aid in matching patients with several common comorbidities, it does not match for HTN and specific cancer types (such as colorectal) other than hematogenous. Fifth, anatomical variations that may have led to the development of conditions being investigated in this study are not reported in the database. Given this, it is not possible to report them in this study. While the study does have its limitations, it is worth noting its strengths as well. The NRD has a large sample size, which provides data for sufficient power analysis. For the years recorded in this study, over 64 million patient encounters were captured by the NRD. Our matching analysis (Table 2) was a strength as well.
Conclusion
Concurrent abdominal stoma is associated with increased postoperative morbidity and mortality after open surgical lower extremity revascularization. Reversing stoma, when possible, may improve post revascularization outcomes. Further prospective studies are needed to validate these results.
Supplemental Material
Supplemental Material - Mortality and Morbidity After Open Surgical Lower Extremity Revascularization in Patients With Peripheral Artery Disease and Concurrent Abdominal Stoma
Supplemental Material for Mortality and Morbidity After Open Surgical Lower Extremity Revascularization in Patients With Peripheral Artery Disease and Concurrent Abdominal Stoma by Matthew Leverich, Ahmed M. Afifi, Gang Ren, Munier Nazzal, and Mohamed Osman in The American Surgeon™
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.