
Abstract
Pneumatosis and portal venous gas are radiological findings that have been historically associated with 70% mortality, and usually trigger surgical intervention. This is due to their association with acute mesenteric ischemia. As cross-sectional imaging usage has increased in recent years, these findings have also been observed in patients with indolent symptoms, the true mortality among patients with pneumatosis or portal venous gas is now theorized to be significantly lower than previously stated. This systematic review was designed to assess the mortality rate among patients with pneumatosis and portal venous gas on initial imaging. We systematically searched Embase, Web of Science, PubMed, and Scopus. Eleven articles were included for final analysis. Ten articles assessed mortality, and included a total of 308 patients, with an overall mortality rate of 31%. Eight articles reported on both ischemia and mortality (n = 233). Of the patients with confirmed ischemia (n = 74), a mortality rate of 69% (n = 51) was noted. Of those without ischemia (n = 159), a mortality rate of 14% (n = 22) was seen. Four studies reported pneumatosis and ischemia (n = 45), in which 64% (n = 29) had ischemia. Four articles reported on portal venous air and ischemia (n = 78). Ischemia was confirmed in 44% of these patients (n = 34). Given an overall mortality of 31% vs prior estimates of 70% for patients with these findings, the decision for surgery on patients with these imaging findings should be made utilizing the overall clinical picture of the patient.
Introduction
Pneumatosis and portal venous gas are radiological findings that have historically been associated with a mortality of 70% or higher. 8 The high mortality rate is due, in part, to their association with acute mesenteric ischemia, which can lead to bowel ischemia and necrosis. Acute mesenteric ischemia occurs when the blood flow through the mesenteric vessels is suddenly compromised and alone this condition has a reported mortality rate of 60%–80%. 10 The mainstream treatment for findings of pneumatosis and/or portal venous gas is emergency surgery to assess the integrity of the bowel and its blood supply; and to restore blood flow when appropriate. However, in recent years, more patients have presented with imaging findings of pneumatosis or portal venous gas whose abdominal symptoms have been mild or nonsignificant. When taken for surgery, some of these patients have had negative surgical exploration; additionally, some of these patient’s symptoms resolved with medical treatment alone with no further increase in morbidity or mortality. Numerous case reports have surfaced in the last decade demonstrating that pneumatosis or portal venous gas is associated with less indolent etiologies than mesenteric ischemia. Pneumatosis and portal venous gas are now associated with a variety of etiologies, with a spectrum from asymptomatic to deadly. 7
This systematic review aimed to review the published data on the incidence of bowel ischemia and the mortality rate among patients with pneumatosis and portal venous air on initial imaging.
Methods
Embase, Web of Science, PubMed, and Scopus were systematically searched using the key words ‘pneumatosis’ and ‘portal vein gas’. For inclusion in this systematic review studies must have been written in English, were comprised of a sample of more than five adult (age ≥18) patients and contain reports of pneumatosis or portal venous gas. The search was completed on September 6th, 2023, no dates were limited. Collectively, the search yielded 515 articles of which 191 were removed as duplicates leaving 324 for consideration for inclusion into this systematic review. Articles were title and abstract screened by this paper’s authors and at least two authors had to concur for inclusion; any disagreements were adjudicated as a group. Of those 324 remaining articles, 196 were eliminated as they did not meet inclusion criteria based on abstract review, leaving 128 for full text review. After full text review another 117 articles were excluded, as they were irrelevant to the current study or were found to not meet the inclusion criteria, a complete list of reasons for article exclusion can be found in the PRISMA Diagram (Figure 1). Eleven articles were included for final analysis, all these studies were retrospective in nature and evaluated the presence of pneumatosis, portal venous gas, or both. PRISMA diagram.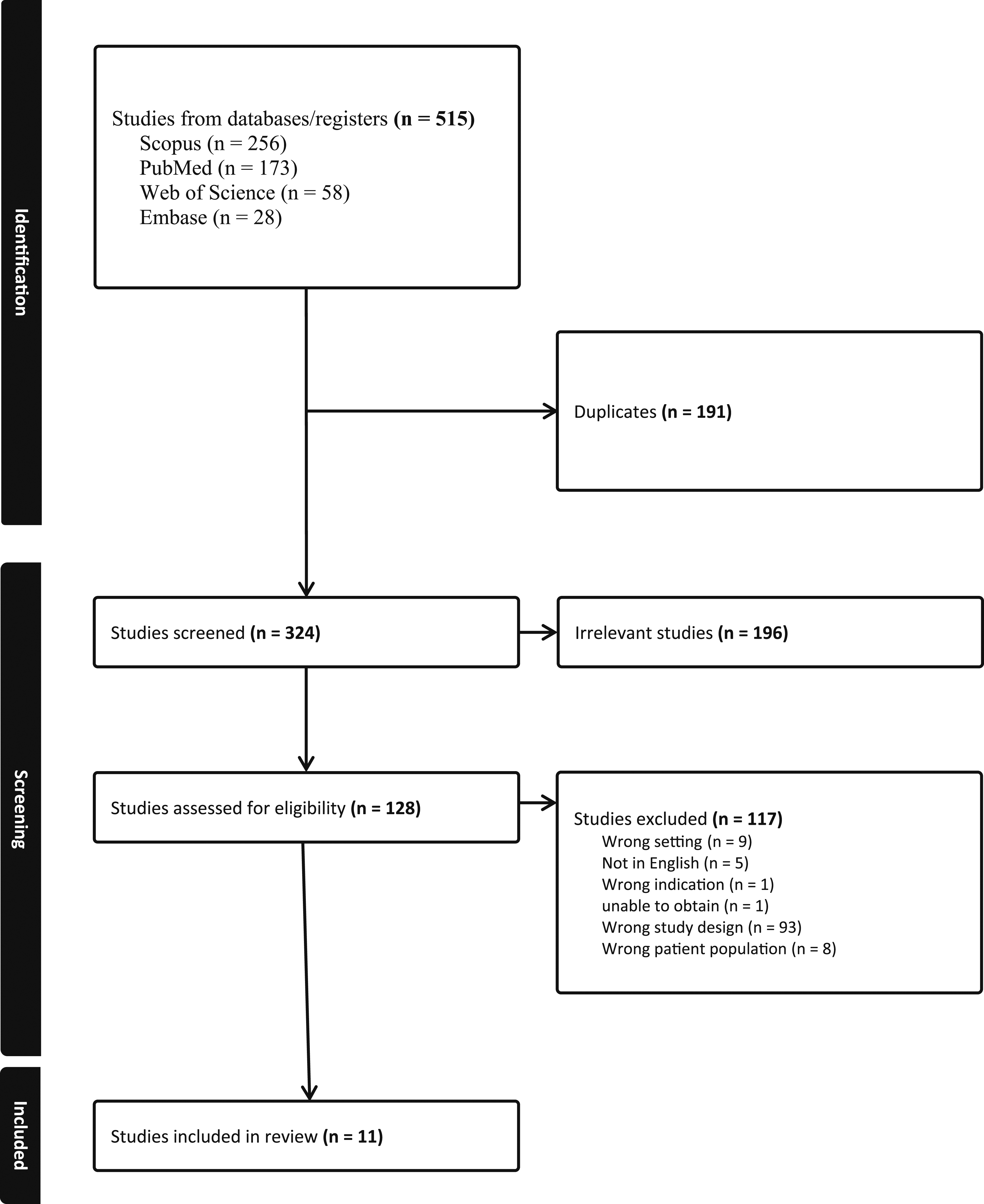
A data extraction spreadsheet was created and administered using CovidenceTM, which is an online platform that streamlines data extraction for systematic reviews. Additionally, a full-text quality assessment was conducted using criteria identified in the revised Downs and Black checklist. 2 The revised checklist includes 10 items on reporting, three items on external validity, 13 items on internal validity, and one item on power. The power item was assessed using modified criteria as reported in previous studies and determined by whether the study included a power analysis (0 = not included, 1 = included). The checklist yields a final numerical score ranging from 0-28 for randomized controlled trials and 0-25 for non-randomized controlled trials. Quality was evaluated using the previously described scoring ranges of strong (21-28), moderate (14-20), limited (7-13), and poor (<7). 2
Results
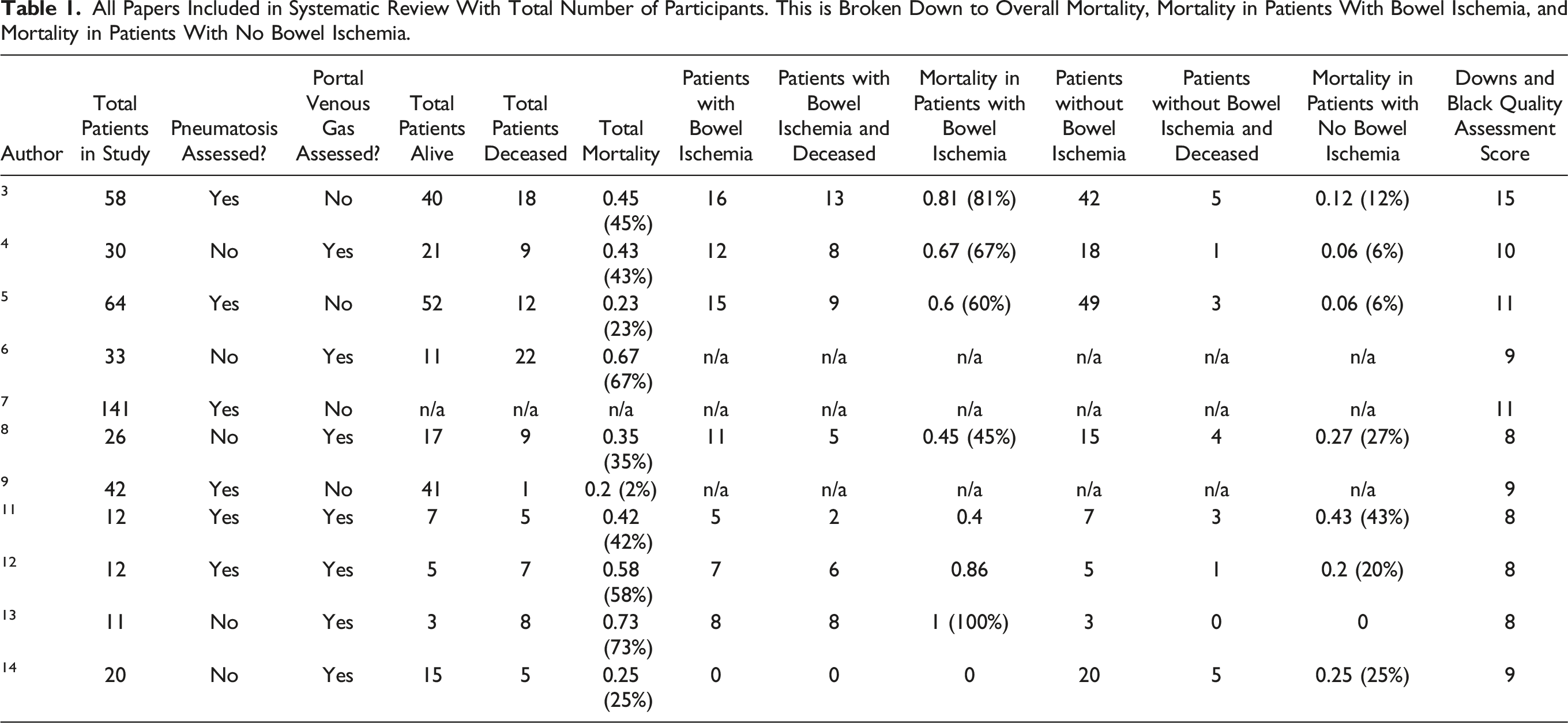
All Papers Included in Systematic Review With Total Number of Participants. This is Broken Down to Overall Mortality, Mortality in Patients With Bowel Ischemia, and Mortality in Patients With No Bowel Ischemia.
Overall Mortality
Ten of the eleven articles provided overall mortality information, while one correlated imaging to pathology. The 10 articles assessing mortality in the presence of pneumatosis or portal venous gas on imaging studies included a pool of 308 patients. In these 10 papers, the overall mortality for patients with radiological findings of pneumatosis or portal venous gas was 31% (Table 1).
Pneumatosis or Portal Venous Gas and Mortality in the Setting of Ischemia vs No Ischemia
Eight out of the eleven articles compared mortality as an outcome of 233 patients with pneumatosis or portal venous gas and bowel ischemia or no bowel ischemia. Out of the 233 patients, 74 had ischemia and 51 of these patients died representing a mortality of 70%. Of the 159 patients who did not have ischemia, 22 died resulting in a mortality of 14% (Table 1).
Pneumatosis with Ischemia
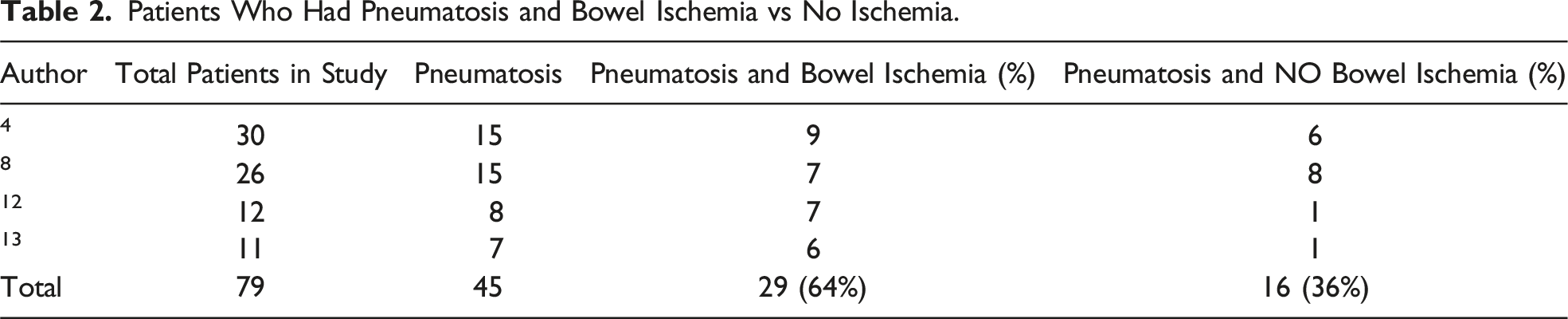
Patients Who Had Pneumatosis and Bowel Ischemia vs No Ischemia.
Portal Venous Gas with Bowel Ischemia
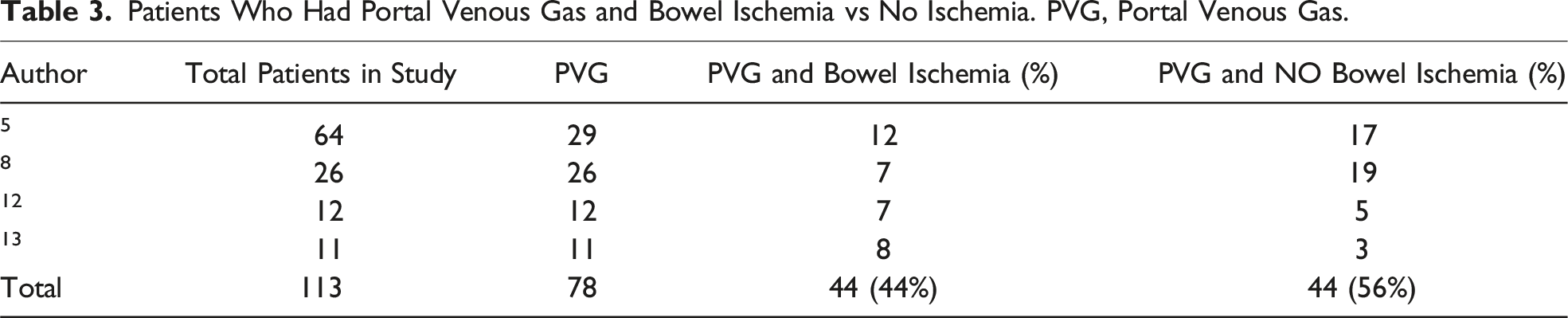
Patients Who Had Portal Venous Gas and Bowel Ischemia vs No Ischemia. PVG, Portal Venous Gas.
Discussion
Bowel ischemia occurs when blood flow to the intestines is compromised. If blood flow is not restored, necrosis and bowel death may occur. Bowel ischemia can be acute or chronic. Causes of acute bowel ischemia can include mesenteric ischemia, volvulus, or incarcerated hernias.
Mesenteric ischemia can be caused by arterial occlusion, thrombosis of the venous system, and non-occlusive ischemia. Arterial occlusion is the most common cause of mesenteric ischemia and can be due to thrombosis, embolus, or dissection of the mesenteric arteries. Mesenteric venous thrombosis can be due to thrombophilia, trauma, or local inflammatory changes. Patients with mesenteric ischemia due to venous occlusion often respond to anticoagulation and reversal of the inciting event. Non-occlusive mesenteric ischemia is caused by vasospasm of the mesenteric vessels rather than a mechanical obstruction of inflow or outflow; it is commonly seen after hypovolemic states and patients who develop profound hypotension. 1
In this systematic review, bowel ischemia in patients was confirmed at time of surgical exploration. For those patients that did not undergo surgical intervention the diagnosis was made clinically. Unfortunately, clinical signs mentioned by authors varied from paper to paper, and in some instances, this was not discussed. Clinical signs of bowel ischemia include diffuse peritonitis, metabolic acidosis, lactate level >4 mmol/L, hemodynamic instability, endoscopy demonstrating necrosis or perforation, imaging demonstrating occluded mesenteric arteries, and as discussed above, pneumatosis or portal venous gas on imaging.
Three main theories for the development of pneumatosis intestinalis and portal venous gas include: (1) the mechanical theory where there is mucosal disruption from increased intraluminal pressure or ischemia; (2) the bacterial theory where gas-forming bacteria translocate into the submucosa of the GI system; and (3) the pulmonary theory, in which air from the lungs escapes the chest cavity and dissolves into the GI and portal venous systems. 5 An increase of incidentally discovered pneumatosis or portal venous gas can be attributed to the increased usage of imaging adjuncts in emergency departments. Especially the increased usage of cross-sectional imaging such as CT scans, which is more sensitive for detection of pneumatosis or portal venous gas than plain radiographs or ultrasound. 8 Additionally, multiple retrospective studies, included in our systematic review, have evaluated the presence of pneumatosis or portal venous gas in the setting of mesenteric ischemia. These studies demonstrate that the association of pneumatosis and portal venous gas with mortality is less than previously reported. The mortality rate in the papers we reviewed ranged from 2% to 73%.
As the usage of cross-sectional imaging has increased, patients with subtle abdominal symptoms have been found to have pneumatosis and portal venous gas, while in the past, imaging was reserved for patients whose symptoms were more critical. In our systematic review, the reported overall mortality for a patient with pneumatosis or portal venous gas was 31%, which is significantly lower than the previously quoted by, 8 of a mortality rate >70%. Furthermore, our systematic review found patients with bowel ischemia are more likely to have pneumatosis than patients with no bowel ischemia, 64% vs 36% respectively. While patients with bowel ischemia are less likely to show portal venous gas in their imaging studies than patients with no bowel ischemia, 44% and 56% respectively.
This systematic review found the presence of pneumatosis, or portal venous gas has an overall mortality of 31%. This is high, however, in the presence of ischemia, the mortality was found to be 69%. Surgical intervention for patients in the bowel ischemia group seems justifiable. When patients with these findings present without ischemia, the mortality rate is 14%, therefore, a selective approach in patients without ischemia and portal venous air or pneumatosis may be used in the proper clinical setting, as suggested in our algorithm (Figure 2). Proposed algorithm for patients who are found to have pneumatosis or portal venous gas.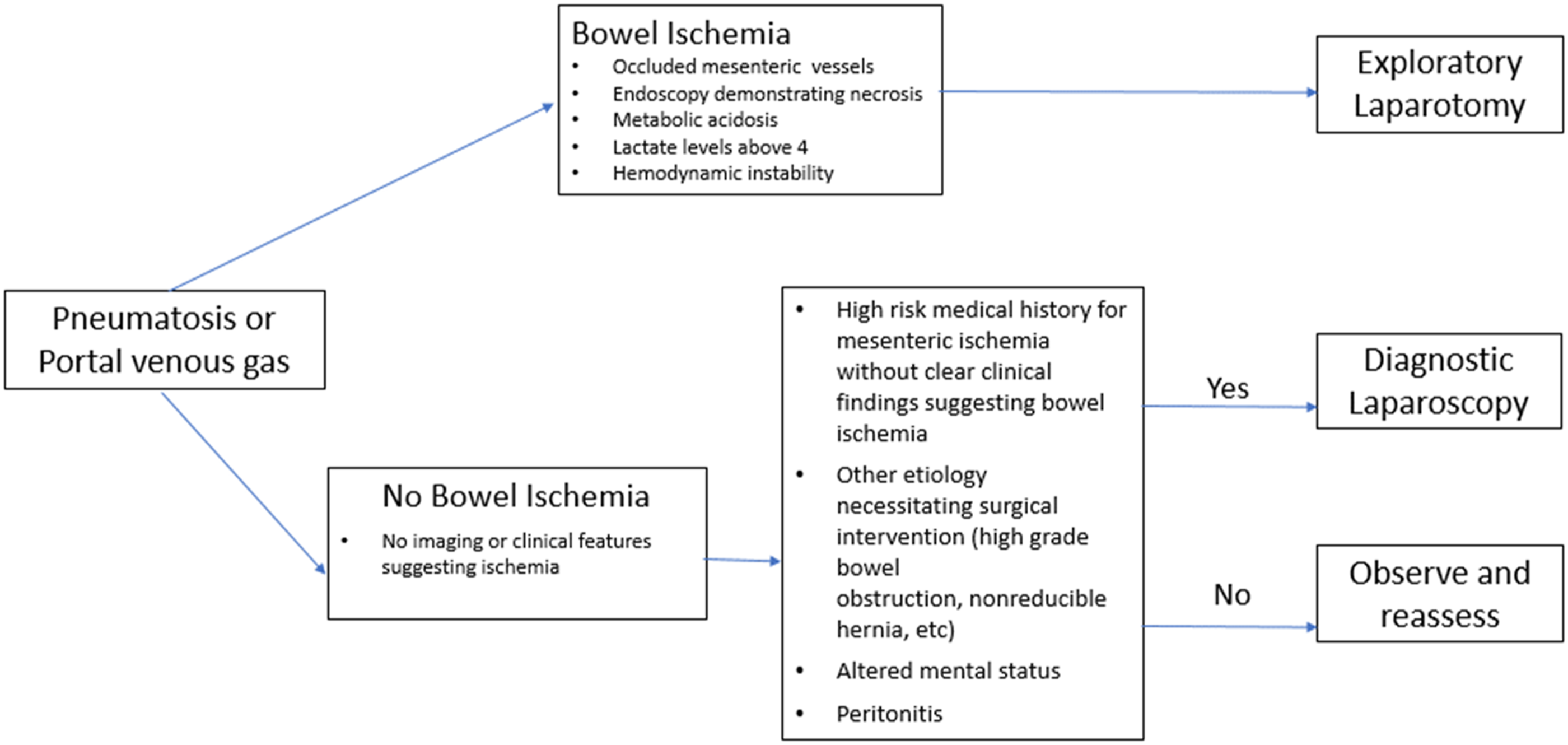
Limitations
This study has several limitations. The major limitation of our study was the quality of the studies identified. All studies reviewed were retrospective in nature. Additionally, only English language literature in was assessed. Finally, the literature search could have been limited by the keywords searched and the databases used.
Conclusion
The findings of our study suggest that pneumatosis and portal venous gas are not absolute indications for surgical exploration with an overall mortality of 31%. The key is to identify those patients who have possibilities of bowel ischemia in this group and to immediately offer these patients surgical exploration. With the surge of cross-sectional imaging, these findings will be expected to become more prevalent and having an appropriate algorithm for these patients is prudent.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.