
Abstract
Purpose
In order to investigate whether colorectal cancer (CRC) patients with endoscopic obstruction benefited from a planned stoma before neoadjuvant chemoradiation (nCRT).
Methods
Patients who were diagnosed with CRC with endoscopic obstruction at a single clinical center from January 2017 to April 2022 were retrospectively collected. Baseline characteristics and short-term and long-term outcomes were compared between the stoma group and the no stoma group. Statistical analysis was performed using SPSS (version 22.0) software.
Results
A total of 51 CRC patients with endoscopic obstruction were included in this study. Eleven (21.6%) patients received a planned stoma before nCRT, and 40 (78.4%) patients were treated with immediate nCRT. The mean time from diagnosis to nCRT was 30.6 days for the stoma group and 11.9 days for the no stoma group. There was a significant delay in the initiation of nCRT in the stoma group (P < 0.05). In terms of complications, there was a statistical difference between the stoma group and the no stoma group (P < 0.05). Planned stoma before nCRT did not affect survival for patients with endoscopically obstructing CRC (P > 0.05).
Conclusion
A planned stoma caused delay in nCRT; the no stoma group was more likely to develop perforation or obstruction of the tumor during nCRT. A comprehensive assessment might be needed to determine whether a planned stoma was necessary in CRC patients with endoscopic obstruction.
Introduction
Colorectal cancer (CRC) was the third most common cancer and the second leading cause of cancer-related deaths in the world.1-5 Radical CRC surgery was still the main treatment at present.6-8 In addition, radiation therapy and chemotherapy were often applied.9,10 A significant proportion of CRC patients presented locally advanced tumor. 11 Upfront nCRT could reduce tumor burden before resection surgery. 12 At present, radical resection surgery after nCRT was the preferred treatment option for patients with locally advanced CRC.13,14 However, tumor progression may occur during nCRT, leading to acute intestinal obstruction, intestinal perforation, bleeding, and other tumor-related complications.
Colonoscopy was the method of choice for diagnosing colorectal cancer. 15 When a CRC grew into the intestinal lumen and caused a stenosis of the intestinal lumen, making it unable to perform a complete colonoscopy, this would be described as endoscopic obstruction.16,17 Endoscopic obstruction may be complete or incomplete. If a patient suffered from acute intestinal obstruction, a temporary stoma, stent implantation, or tumor resection surgery would be performed. 18 As for patients without clinical obstruction who needed nCRT, they were still at risk of developing bowel obstruction and perforation, so a temporary stoma might be performed prior to nCRT for patients with high-risk factors of intestinal obstruction. 19
The planned stoma was obviously performed in patients with complete bowel obstruction. 20 However, there were few studies on the planned stoma before nCRT for patients with asymptomatic endoscopic obstruction. Planned stoma before nCRT might reduce the incidence of subsequent obstruction and perforation, or patients might suffer more damage due to the stoma, causing adverse effects. Therefore, the aim of our study was to investigate the effects of planned stomas before nCRT in CRC patients with endoscopically obstructing CRC.
Materials and methods
Patients
The Clinical Research Ethics Committee of the First Affiliated Hospital of Chongqing Medical University reviewed and approved this study (K2024-077-01), and all patients signed an informed consent form. All patient information was strictly confidential and used solely for this study. Patients who were diagnosed with CRC and were observed endoscopic obstruction at a single clinical center from January 2017 to April 2022 were retrospectively collected.
Inclusion and Exclusion Criteria
Colorectal cancer patients with endoscopic obstruction at a single clinical center were included (n = 560). The exclusion criteria were as follows: 1, patients with complete endoscopic obstruction or symptoms of acute intestinal obstruction such as abdominal pain, abdominal distension, vomiting, and no gas or stool excreted from the anus (n = 192); 2, patients not requiring nCRT before resection surgery (n = 295); 3, patients with incomplete medical record (n = 22). Finally, a total of 51 eligible CRC patients were enrolled for final analysis. There were 11 patients in the stoma group.
Clinical Decision Making for Ostomy
For patients with endoscopic obstruction and no clinical symptoms, there were no clinical guidelines that had a clear statement about whether to stoma or not. In this study, whether a patient would undergo stoma mainly depended on the doctor’s judgment and the patient’s own will.
Data Collection
Patient information was collected from the inpatient medical system, outpatient service system, and telephone interviews. Endoscopic obstruction was recognized in every patient. Baseline characteristics included age, sex, body mass index (BMI), smoking, drinking, hypertension, type 2 diabetes mellitus (T2DM), previous abdominal surgery (PAS), tumor location, time from diagnosis to initiation of nCRT, and resection surgery. Outcomes included major complications and overall survival (OS).
Definition
Complications were graded according to the extended Clavien-Dindo classification of surgical complications, 21 and ≥ III classification complications were defined as major complications that were recorded in this study. Overall survival was defined as the time from diagnosis to death or last follow-up.
Statistical Analysis
Categorical variables were evaluated using Chi-square tests and were expressed as n (%). Continuous variables were evaluated using t-tests and were expressed as mean ± standard deviation (SD). The Kaplan-Meier method was used for survival curves. Statistical analyses were performed by SPSS (version 22.0) software.
Results
Patients
Based on inclusion and exclusion criteria, a total of 51 eligible patients were enrolled in the study. Eleven (21.6%) patients received a planned stoma before nCRT. The remaining 40 (78.4%) patients received immediate nCRT without stoma preformation after diagnosis (Figure 1). Baseline characteristics included age, sex, body mass index (BMI), smoking, drinking, hypertension, type 2 diabetes mellitus (T2DM), previous abdominal surgery (PAS), tumor location, time from diagnosis to initiation of nCRT, and resection surgery. Age was statistically different between the two groups (P < 0.05). There was a significant delay in the time from diagnosis to initiation of nCRT in the stoma group (P < 0.05). Other characteristics were well matched, and there was no statistical significance. Outcomes included major complications and overall survival (OS). The incidence of complications during nCRT in the no stoma group was significantly higher than that in the stoma group (P < 0.05). Flow chart of patient selection.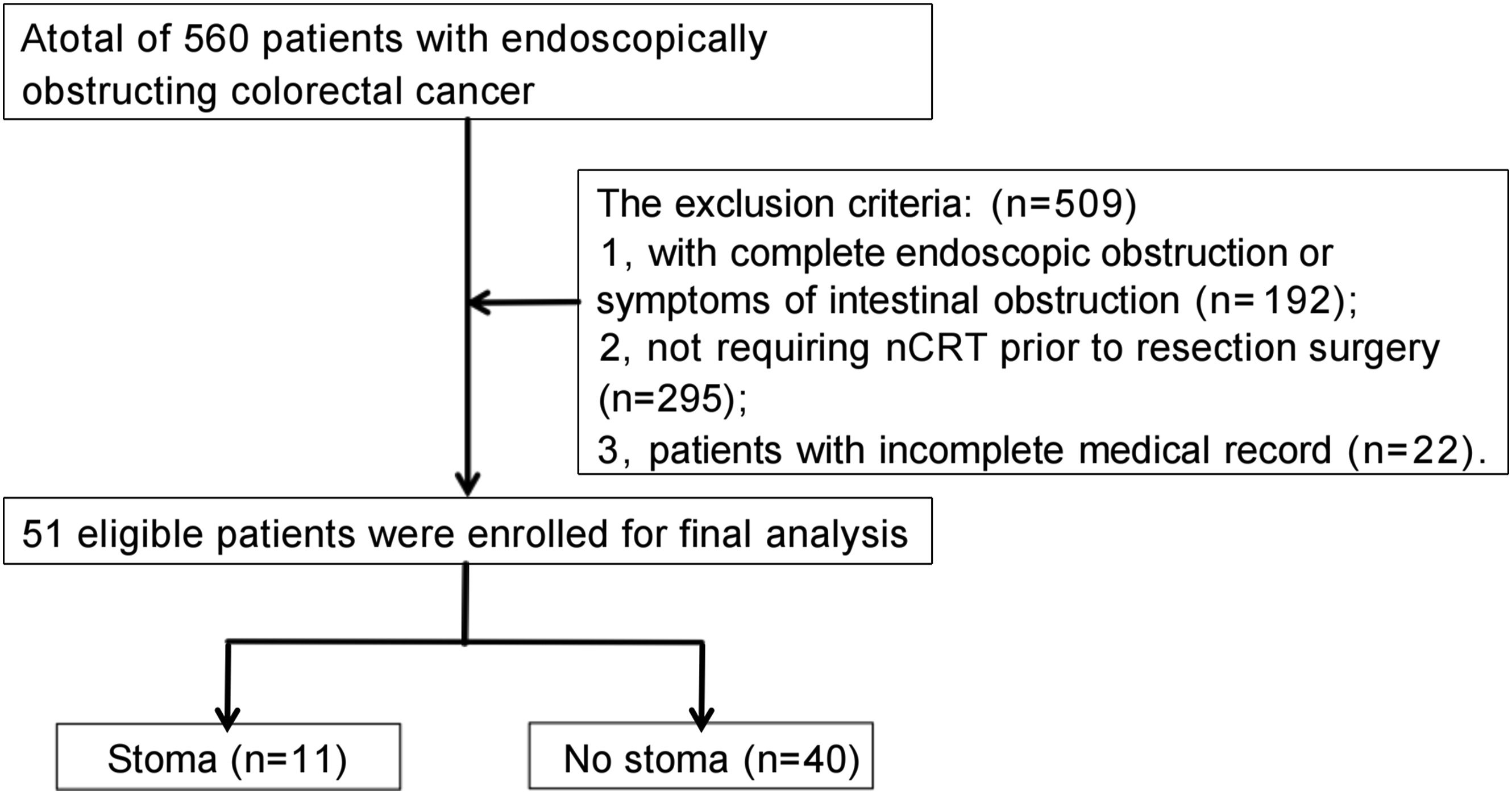
Time to Treatment
Information Between Two Groups.
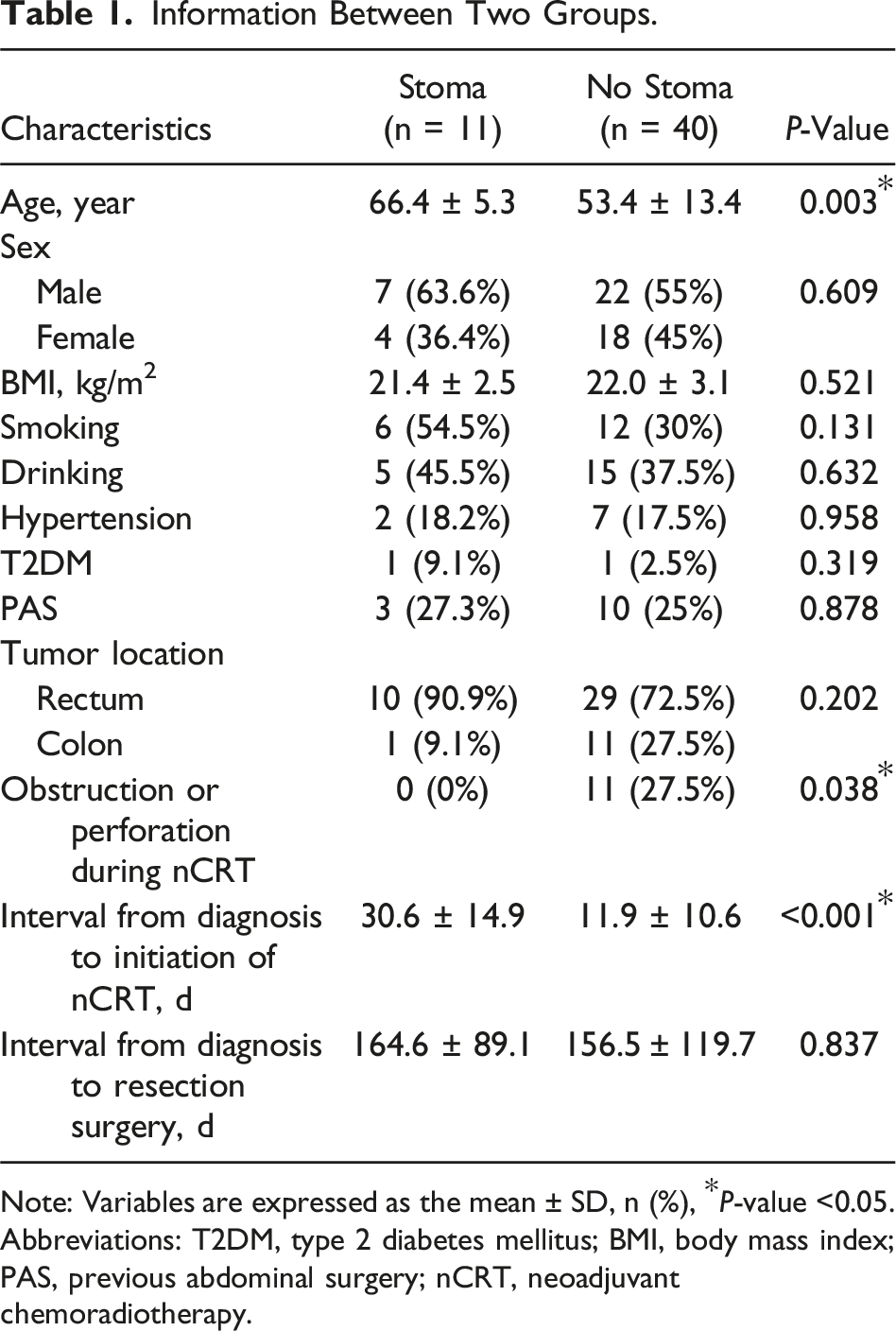
Note: Variables are expressed as the mean ± SD, n (%), *P-value <0.05.
Abbreviations: T2DM, type 2 diabetes mellitus; BMI, body mass index; PAS, previous abdominal surgery; nCRT, neoadjuvant chemoradiotherapy.
Major Complications
In the no stoma group, eleven patients developed intestinal obstruction during the period of nCRT. One of them recovered with conservative treatment. The other ten underwent colostomy surgery. There was no major complication in the planned stoma group. Moreover, there was a statistically significant difference in complications between the two groups.
Survival
Overall survival was compared between the two groups to evaluate the long-term outcomes. The results showed no significant difference in OS between the two groups (P > 0.05) (Figure 2). OS between the stoma group and the no stoma group. Note: OS, overall survival.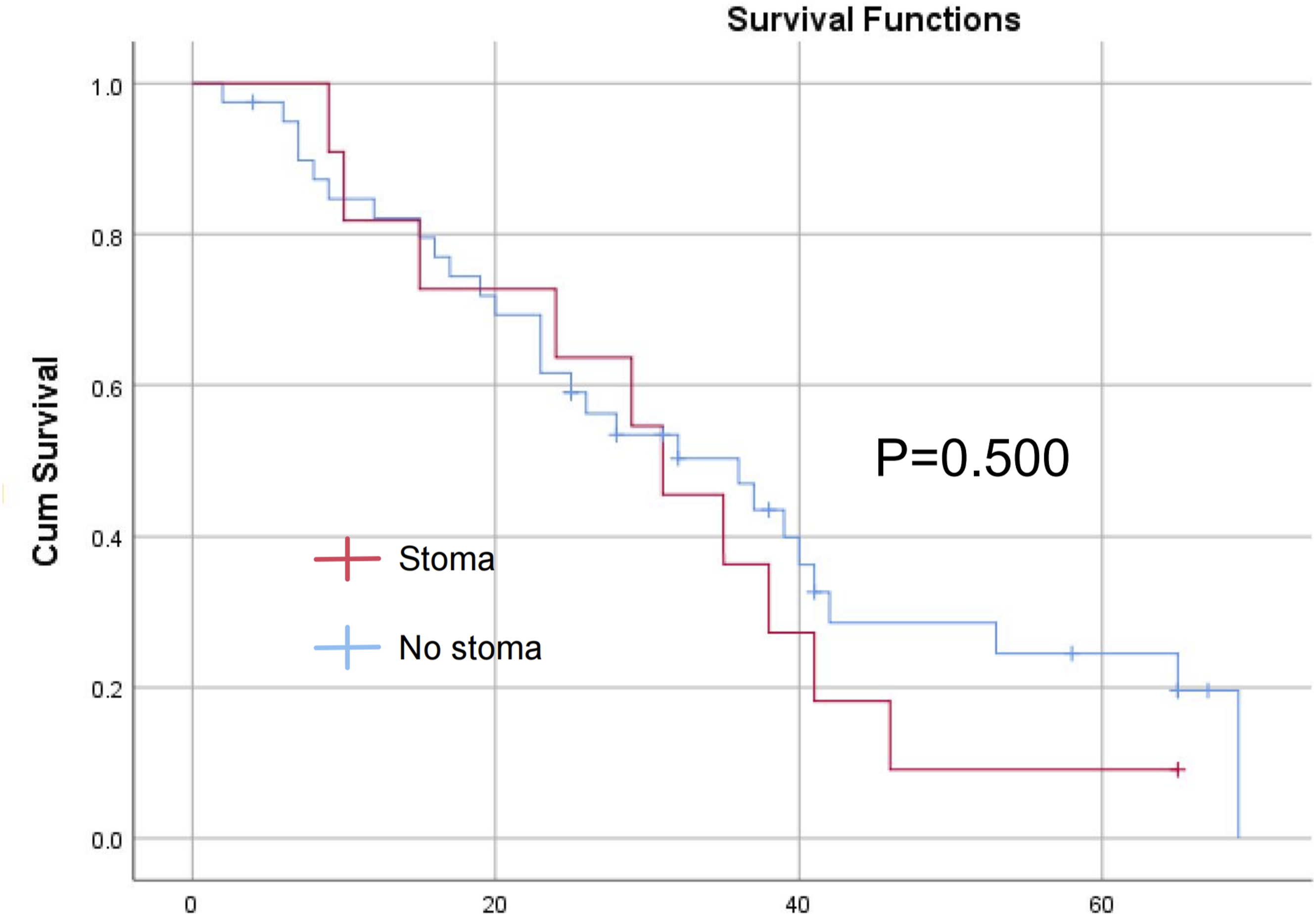
Univariate and Multivariate Logistic Regression Analyses of the OS
Univariate and Multivariate Analyses of Overall Survival.
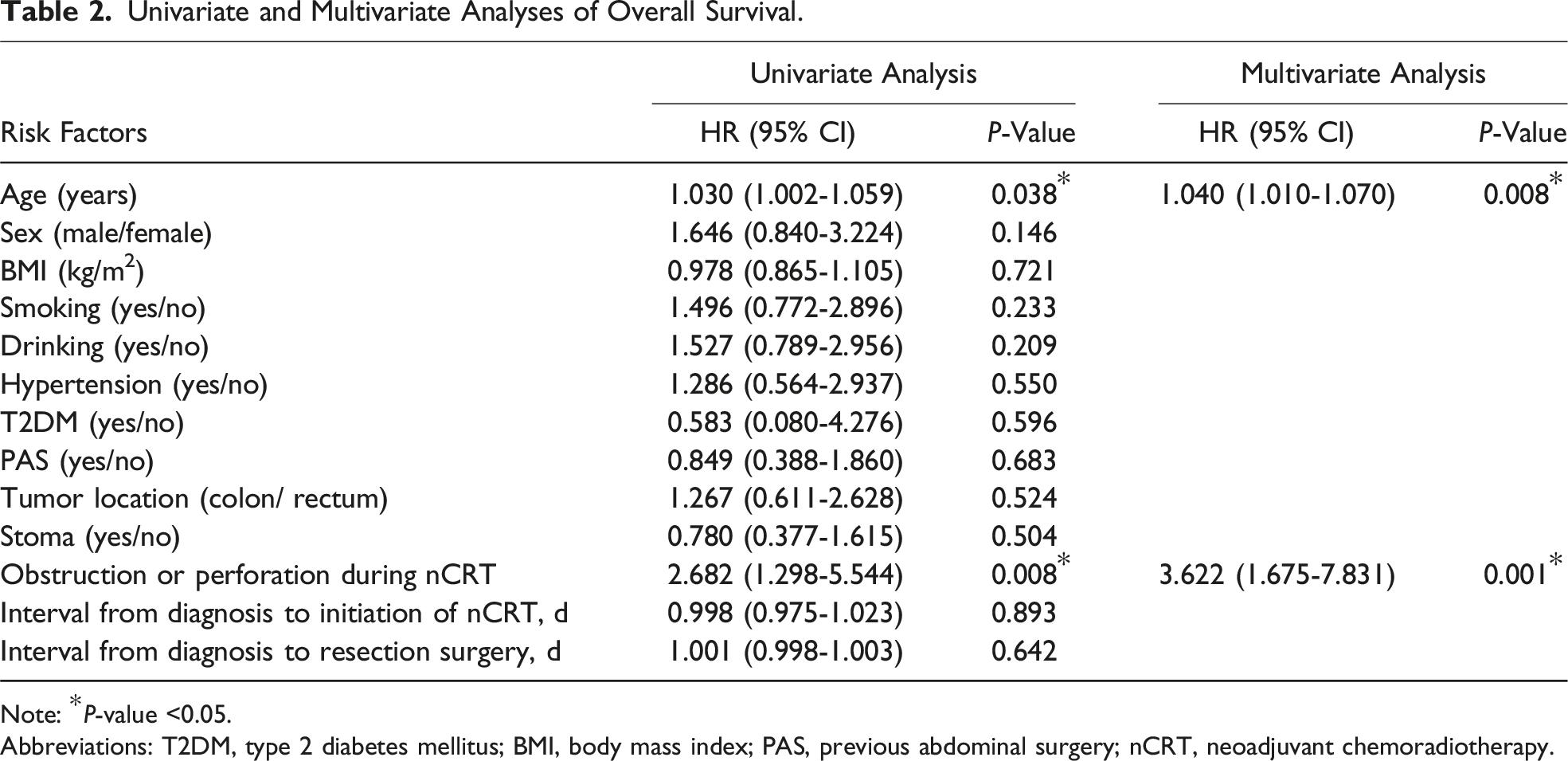
Note: *P-value <0.05.
Abbreviations: T2DM, type 2 diabetes mellitus; BMI, body mass index; PAS, previous abdominal surgery; nCRT, neoadjuvant chemoradiotherapy.
Discussion
The study was performed with 51 CRC patients who had endoscopic obstruction and underwent nCRT. The results showed that patients in the planned stoma group had a significantly delayed time to nCRT. The incidence of complications during nCRT in the no stoma group was significantly higher than that in the stoma group. However, there were no significant differences between the two groups in the time from diagnosis to resection surgery and OS.
Patients with locally advanced CRC were not candidates for immediate resection surgery, and they needed to receive nCRT first. 22 And nCRT was the standard treatment for locally advanced CRC.23,24 Approximately 20% of CRC patients undergoing nCRT achieved pathologic complete response, and 25 nCRT improved tumor resection rates and decreased tumor recurrence rates. 26 In patients with endoscopic obstruction, timely initiation of therapy might be necessary. These tumors were often advanced and might require timely local control. 27 However, the main problem triggered by immediate nCRT was that tumor progression might lead to complete obstruction or perforation during the period of nCRT. 28 It could lead to interruptions and emergency surgery in nCRT.
Performing a planned stoma could effectively prevent complications caused by tumor progression. 29 There were few studies on the need for planned stoma before nCRT in CRC patients with only endoscopic obstruction. A study suggested that selective planned stoma might be beneficial for patients with T3/T4 rectal adenocarcinoma. 30 However, there was no evidence that this applied to all patients with locally advanced endoscopic obstruction. Patel et al 29 also showed that endoscopic obstructive rectal cancer cannot be used alone to assess a patient’s risk of intestinal perforation. Current research preferred to consider a planned stoma before treatment for CRC patients with locally advanced with symptoms of obstruction. Another related study showed that patients who received a planned stoma were more likely to receive a permanent stoma after resection surgery. Notably, this was related to the location of the tumor as well as the surgical approach chosen by the surgeon. 28
In this study, we analyzed the impact of planned stoma before nCRT in terms of interval from diagnosis to treatment, occurrence of major complications during nCRT, and overall survival. Stoma surgery and postoperative rehabilitation could be time-consuming. If complications occurred after the operation, the time would be much longer. Although a planned stoma could prevent possible complete obstruction or perforation, this resulted in a significantly longer time to nCRT initiation and a delay in subsequent treatment in the planned stoma group. Absolutely, we observed some patients suffer from intestinal obstruction or perforation during nCRT in this study, which all occurred in the no stoma group. Moreover, there was a statistically significant difference in complications between the two groups. The delay in treatment and the occurrence of complications during treatment might affect the overall survival of patients. A stoma might increase the difficulty of subsequent resection procedure. Therefore, whether to perform stoma might require clinicians to conduct a holistic assessment of the patient to develop a more appropriate treatment.
For patients with endoscopically obstructing colorectal cancer, the study could provide a reference for surgeons to develop appropriate plans for patients. It might further improve the survival of patients. However, our study had some limitations: inadequate sample size, differences in treatment options for patients, and unrecorded adverse events after stoma surgery which might bias the results. Studies with a larger sample size were needed for further exploration.
In conclusion, in patients without clinical signs of intestinal obstruction, there was no clear result on the need for ostomy before nCRT. It was necessary for clinicians to evaluate the patients’ conditions and make choices according to the patients' demands. Subsequent studies and evidence were still needed to investigate this clinical question.
Footnotes
Acknowledgments
We acknowledge all the authors whose publications are referred in our article.
Authors’ Contributions
All authors contributed to data collection and analysis, drafting, or revising the manuscript, have agreed on the journal to which the manuscript will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data sets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.