
Abstract
Surgical site infections (SSIs) remain a significant concern in high-risk patients undergoing abdominal surgeries with class 3 and class 4 wounds. This study examines the efficacy of Intact Fish Skin Grafts (IFSGs) in reducing SSIs. Conducted at two urban hospitals from July 2021 to November 2023, the study included 31 patients who underwent emergency abdominal procedures. IFSG was applied at the fascia level, and patients were monitored for 40 days postoperatively. The results demonstrated SSI rates of 5.9% in class 3 wounds and 7.1% in class 4 wounds, which is significantly lower than historical averages. The median hospital length of stay was reduced to 4 days for class 3 and 6 days for class 4 wounds. These findings suggest that IFSG presents a promising alternative to standard closure techniques, offering improved clinical outcomes and potential cost savings.
Keywords
Key Takeaways
This prospective cohort study evaluated the use of Intact Fish Skin Grafts (IFSGs) in reducing surgical site infections (SSIs) and improving outcomes in high-risk patients with class 3 and class 4 wounds during urgent/emergent abdominal surgeries. Thirty-one patients were followed, with SSI rates of 5.9% for class 3 and 7.1% for class 4, significantly lower than reported in existing literature. The study concludes that IFSG is effective in lowering SSI rates and hospital length of stay, suggesting potential cost savings for health care systems.
Introduction
Surgical site infections (SSIs) account for a substantial burden on health care systems, contributing to increased morbidity, mortality, and financial costs. Patients with class 3 (contaminated) and class 4 (dirty/infected) wounds are particularly susceptible to SSIs.1-3 Traditional management approaches, such as negative pressure wound therapy (NPWT), are costly and may not always be effective in reducing infection rates. Intact Fish Skin Grafts (IFSGs) have emerged as a novel alternative due to their antimicrobial properties and biocompatibility. This study evaluates the impact of IFSG on SSI rates, hospital length of stay (LOS), and overall patient outcomes in high-risk surgical patients.
We aim to examine the impact of Intact Fish Skin Grafts (IFSG) (“Kerecis” LLC, Reykjavik, Iceland) on reducing SSI rates and expediting healing in high-risk patients with class 3 and class 4 wounds in urgent and emergent abdominal surgeries. In order to achieve this goal, we used a single component minimally processed IFSG from wild caught Atlantic cod (Gadus Morhua) fish skin, which contains polyunsaturated fatty acids that have antimicrobial properties. 4 We used “SurgiBind,” a product developed with fat, elastin, glycans, and protein scaffolds, designed for soft tissue reinforcement in areas of weakness, such as the abdominal wall.
Methods
A prospective observational study was conducted at two urban hospitals from July 2021 to November 2023. Patients presenting with class 3 or class 4 wounds requiring emergency abdominal surgery were enrolled. IFSG was applied at the fascia level, and all wounds were closed with staples. Patients were followed for 40 days postoperatively. None of the patients received NPWT. Data on SSI rates, mortality, and hospital LOS were collected and analyzed using Jeffreys’s Amazing Statistics Program (JASP) 0.18.3 software.
Results
Patient Demographics (N = 31).
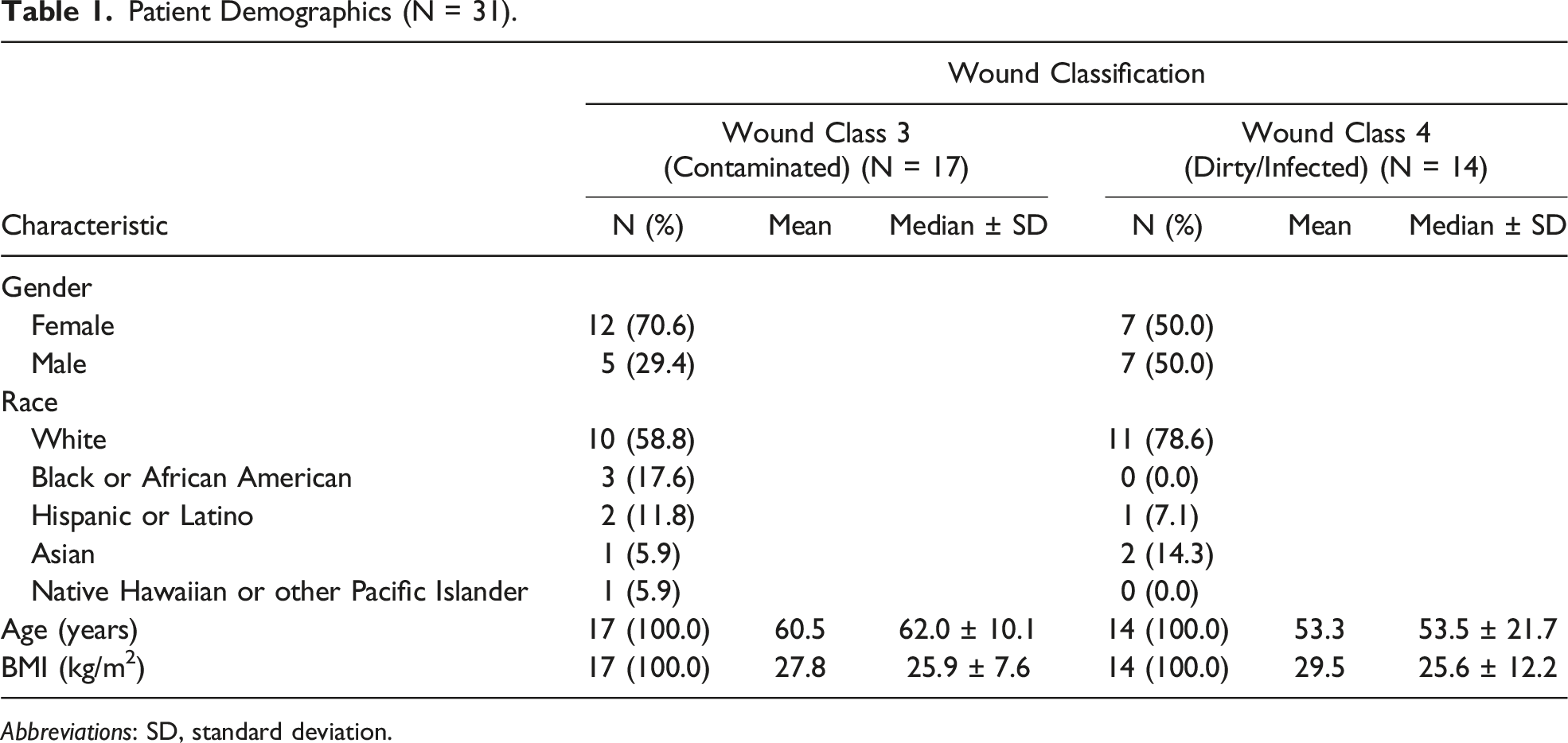
Abbreviations: SD, standard deviation.
Comorbidities, medical history, and key laboratory data were reviewed for each surgical wound classification. It is worth pointing out that the top comorbidities in both groups were anemia, hypertension, and diabetes. BMI, hemoglobin, hematocrit, maximum perioperative blood sugar, transferrin, and prealbumin were very similar between the groups. It must be mentioned that HbA1c, transferrin, and prealbumin were not always ordered, and some patients are missing those data points.
Facility, Procedure Category, and Treatment Outcomes (N = 31).
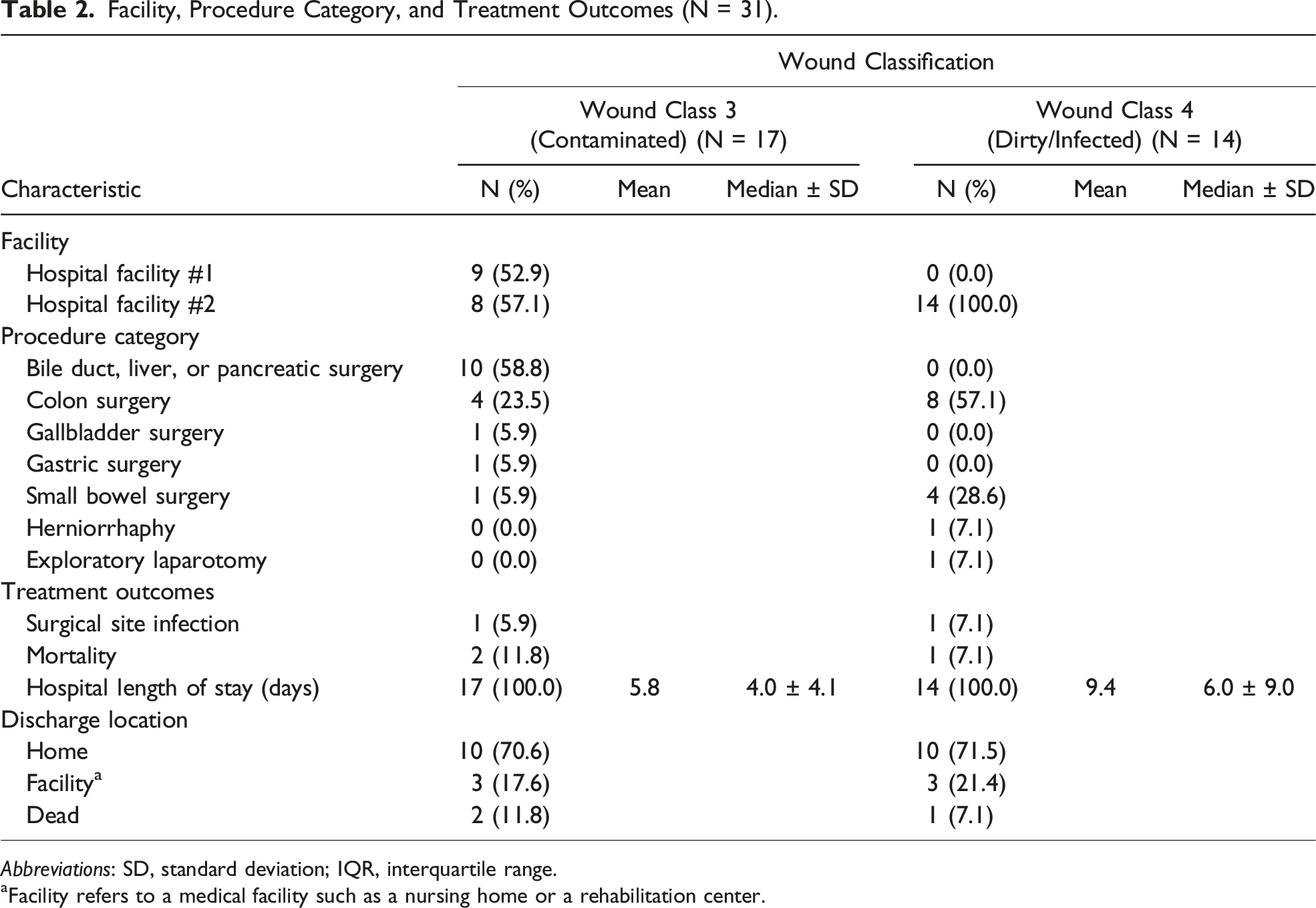
Abbreviations: SD, standard deviation; IQR, interquartile range.
aFacility refers to a medical facility such as a nursing home or a rehabilitation center.
We suggest that there are immediate cost savings resulting from a shorter LOS and reduced use of NPWT, which is the current standard. Although the goal of this study was not to compare costs between IFSG and NPWT in contaminated wounds, we found that IFSG reduces SSIs and did not require a patient to have home health care needs. Furthermore, this patient group could experience significant long-term cost savings from a reduced incidence of abdominal hernia formation.
Discussion
The application of IFSG demonstrated a notable reduction in SSI rates and hospital LOS compared to conventional methods. These findings suggest that IFSG may serve as an effective adjunct for managing high-risk wounds in emergency surgical settings. The cost-effectiveness of IFSG, given its potential to reduce extended hospitalization and additional wound care expenses, warrants further investigation.
Conclusion
This study supports the use of IFSG in class 3 and class 4 wounds to lower SSI rates and hospital LOS. Larger, multicenter randomized trials are necessary to confirm these findings and establish IFSG as a standard adjunct in contaminated wound management.
Footnotes
Acknowledgments
We are willing to make data, analytic methods, and study materials available to other researchers. Please contact corresponding author for information. Conducted research was not preregistered with an analysis plan in an independent, institutional registry. The authors have no additional acknowledgments.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Lantis, Dr Ellis, and Dr Joseph have received a speaking fee from IFSG manufacturer that was used in this study “Kerecis” LLC.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection was funded by the manufacturer of the product that was used in this study “Kerecis” LLC. “Kerecis” LLC was not involved in study design, data collection, data analysis, manuscript preparation, and publication decisions. Authors confirm that they had complete access to the study data that support the publication.