
Abstract
Primary osseous sarcoma of the breast (POB) is exceedingly rare and aggressive. Breast sarcomas account for <1% of breast cancers with osteosarcoma accounting for only 12.5% of all breast sarcomas. The rarity of these cases affords for limited published literature and therefore demands a case-by-case examination for treatment. Primary osseous sarcoma of the breast typically presents as a rapidly growing mass that tends to be heavily calcified. Diagnosis should be completed based on current societal guidelines for breast cancer detection. The minimum recommended therapy is early surgical intervention. Osteosarcoma is resistant to radiotherapy; however, there has been some evidence for the use of adjuvant chemotherapy. Due to the scarcity of research to guide treatment, we recommend presentation of individual patients at a multidisciplinary tumor board to create a treatment plan on a case-by-case basis.
Background
Breast cancer is the most common cancer in affecting women apart from skin cancer in the United States. Breast sarcomas account for less than 0.1% of all breast cancers and of those, primary breast osteosarcoma accounts for roughly 12.5%.1-3 Due to the rarity of cases, limited published literature is available and treatment is directed on a case-by-case basis. Extraskeletal osteosarcoma (ESOS) is a malignant mesenchymal tumor that produces neoplastic osseous tissue with no direct correlation to bone or periosteum. 4 Extraskeletal osteosarcomas typically occur in peripheral extremities and affect a younger patient population. However, they have been described in other locations such as the liver, heart, larynx, and in this case the breast, which are more common in older patients. 4 The prognosis for ESOS is poor with the majority of patients progressing and succumbing to metastatic disease within 2-3 years after initial diagnosis.5,6 While some studies suggest tumorigenesis occurs due to neoplastic transformation from a pre-existing breast lesion, there are several case reports describing primary breast ESOS without pre-existing neoplasms.3,7,8
Pathology
Histological analysis is crucial for establishing the diagnosis of POB. Evaluation typically reveals abundant osteoid formation with areas of calcification and moderately pleomorphic, oval- to spindle-shaped stromal cells. 1 Tumors are usually rich in scattered multinucleated osteoclastic giant cells and heteromorphic osteoblast-like cells.1,7 Central necrosis, as well as small cartilaginous foci, are also commonly found. Mitotic figures are frequently observed, though not required for diagnosis. 5
Immunohistochemical testing must demonstrate a lack of epithelial differentiation to rule out a primary osteogenic sarcoma arising from bone and to distinguish from metaplastic carcinoma, malignant phyllodes tumor, or carcinosarcoma containing osteoid and bone. 7 Osteoblastic differentiation can be confirmed with SATB2 testing, as SATB2 is primarily expressed in bone tumors with osteoblastic features. Vimentin is also frequently positive, though it is not essential for diagnosis.1,7
Clinical Presentation
Primary osseous sarcoma typically presents as a rapidly growing mass that tends to be heavily calcified.
1
Defined as a malignant mesenchymal neoplasm that produces osteoid, ESOSs are located in the soft tissue without skeletal or periosteal attachment.
9
Extraskeletal osteosarcomas are most commonly located within the soft tissue of the thigh (46%), followed by the upper extremity (20%) and the retroperitoneum (17%), but can occur in any part of the body.
9
These densely calcified masses can be difficult to delineate based on imaging alone
10
(Figure 1). Radiographic imaging will generally show a variable amount of mineralization and lack of skeletal involvement; however, approximately 50% of masses have no calcifications seen.
9
(A) Diagnostic mammography with area of dystrophic calcification. (B) MRI showing same area of calcifications.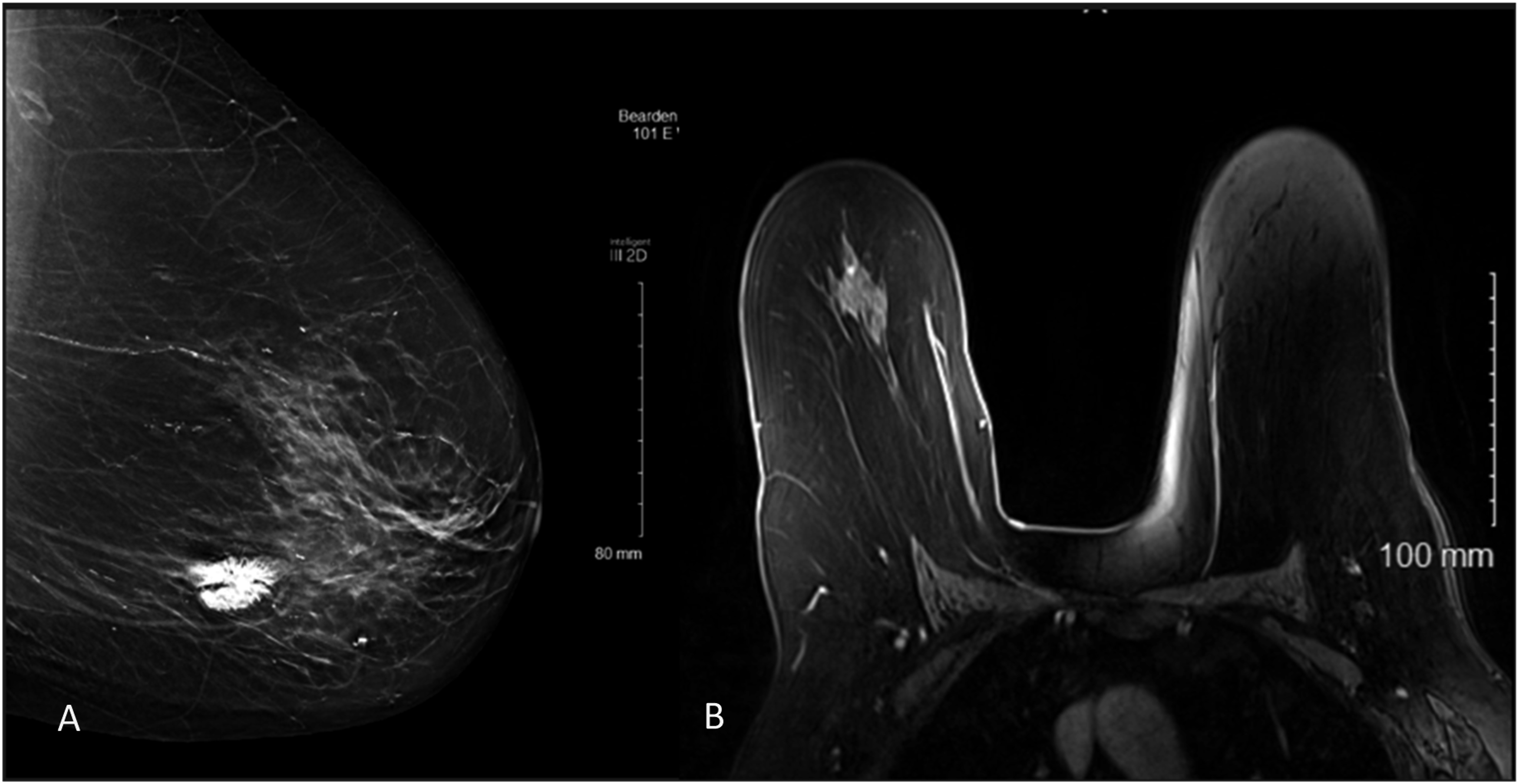
Extraskeletal osteosarcomas maintain a very poor prognosis with more than 80-90% of patients developing local recurrences and/or metastasis. 9 Studies estimate a 5-year survival rate of 38% and a 10-year overall survival rate of 32%.3,7 Primary osseous sarcoma of the breast metastasizes through hematogenous spread, and therefore sentinel lymph node biopsy and/or axillary lymph node dissection are not recommended. 7 Metastases are most common to the lung followed by bone and liver. 1
Therapeutic Approach
Treatment modalities vary and have not been universally agreed upon due to the rarity of POB. The minimum therapy recommended however is early surgical intervention. Lumpectomy with wide margins or simple mastectomy is acceptable. Radiotherapy and chemotherapy have not shown an inherent benefit and therefore should be determined on a case-by-case basis. Osteosarcoma is resistant to radiation therapy and is generally not recommended unless the patient has positive margins or a large mass that cannot be fully excised.7,9,12 Some studies have suggested that adjuvant chemotherapy may be of value for POB treatment strategies, with improved survival rates in those who received perioperative chemotherapy.7,11 However, this study was conducted on ESOS cases as a whole and was not POB specific. 11 With limited research and evidence to guide treatment, it appears the most important intervention is early surgical excision with negative margins.
Diagnostic Workup
Routine screening with ultrasound and/or mammography as well as biopsies should be completed in accordance with guidelines by either the American Cancer Society, ACOG, or USPSTF for all women, beginning with annual screening between 40 and 45 years of age. Interval imaging is recommended for these patients to evaluate for recurrence as well as metastatic disease progression. It is also recommend to continue follow-up for these patients as recurrence and metastasis are common and overall survival at the 5- and 10-year marks remains low.
Conclusion
Primary osteosarcoma of the breast remains an extremely rare disease with poor prognosis. The use of adjuvant chemoradiation remains unclear, and the best treatment is adequate excision with wide margins. Due to the rarity of POB, further research into the use of adjuvant chemoradiation and additional treatment modalities is needed to improve disease progression and survival rate. We recommend routine screening based on current societal recommendations with both radiologic and clinical examination. Finally, presentation of these individual patients at a multidisciplinary tumor board would be of benefit to create a treatment plan on a case-by-case basis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.