
Abstract
Introduction
Shock index (SI) is useful in assessing hemodynamic status and predicting outcomes. Delta shock index (ΔSI), measuring changes in SI over time, highlights its dynamic role in predicting patient deterioration and mortality risk. This study hypothesizes that ΔSI in the rural setting has a predictive value in patient outcomes.
Methods
Study data from January 2017 to July 2023 was obtained from the trauma registry at a rural Level 1 trauma center. This study employed SI (HR/SBP) based on vital signs collected at the transfer facility, scene, and trauma bay (TB). Delta SI, the change seen in SI from TB arrival compared to earlier measurements, was computed, and patients were stratified into two groups based on ΔSI values: those with positive ΔSI (+ΔSI) and those with zero or negative ΔSI. The primary outcome examined was mortality, alongside secondary outcomes such as hospital length of stay (HLOS), ICU length of stay (ILOS), and blood transfusions.
Results
Patients with +ΔSI were older, had longer HLOS and ILOS, and higher injury severity scores. Patients with +ΔSI were more likely to have increased mortality rates (6.8% vs. 3.6%, P < 0.001) and blood transfusions (14.5% vs. 9.7%, P < 0.001). Multivariable logistic regression further validated +ΔSI significantly increasing odds of early mortality (OR 2.061, P = 0.008) and in-hospital death (OR 1.465, P = 0.002).
Discussion
Positive ΔSI is associated with negative patient outcomes, including early and overall mortality. The results show the predictive value of ΔSI in a rural environment.
Introduction
The shock index (SI), calculated as the ratio of heart rate to systolic blood pressure, is a simple yet informative tool used to assess hemodynamic status and predict outcomes in various clinical scenarios. SI was first described by Allgöwer in 1967 as a more effective way to identify impending circulatory collapse. 1 Many studies have since proven the correlation between an SI >0.9 and increased rates of mortality and blood transfusions in trauma patients from both urban and rural environments.2,3 Delta shock index (ΔSI), measuring changes in SI over time, holds the potential to predict patient deterioration and mortality risk more dynamically.
Recent studies have revealed an association between ΔSI and increased mortality and the need for blood transfusion in the urban trauma patient population.4-7 ΔSI can predict increased mortality even in cases where patients appear hemodynamically stable and present with normal vital signs and SI. 8 Elevated ΔSI has been shown to have adverse outcomes for patients across all adult age groups. Asim et al looked at a trauma patient population with an average age of 33 years and noticed increased mortality and resource utilization for elevated ΔSI patients. 4 In another study, older patients (>65 years) with an elevated ΔSI exhibited an increased need for emergency surgery after blunt trauma. 9 Early recognition of changes in SI, particularly in the prehospital setting, may facilitate timely interventions and improve patient outcomes in trauma care. ΔSI holds an emerging role as a dynamic and informative parameter for risk stratification and prognostication in the clinical setting.
Rural trauma care presents unique challenges, such as increased distance to hospital. An estimated 41.9% of rural Americans do not have access to a trauma center within an hour of their home. 10 Vital signs are more likely to change during these long transport times, highlighting the need for a value that communicates these changes. Few studies have evaluated the role ΔSI might play in rural trauma care. This study hypothesizes that ΔSI also has a predictive value in patient outcomes in the rural setting.
Methods
The study protocol was approved by the Institutional Review Board. Data from January 1st, 2017 to July 31st, 2023 was extracted from the trauma registry. All adult (age ≥ 18) trauma activations arriving by ground or air ambulance with complete data were included. This resulted in a study population of 8546 patients.
SI was derived from vital signs recorded at the transfer facility, scene, and in the trauma bay (TB). ΔSI represented the difference between SI at TB arrival and initial SI at the transfer facility for transfer patients and the difference between SI at TB arrival and SI taken by EMS for scene patients. Patients were categorized into 2 groups: those with a positive ΔSI (+ΔSI) and those with zero or negative ΔSI (ΔSI ≤0). The primary endpoint assessed was in-hospital mortality, while secondary outcomes included hospital length of stay (HLOS), ICU length of stay (ILOS), need for blood transfusion, discharge disposition, and early mortality, defined as death within 48 hours of admission.
Data were summarized as mean (standard deviation) for continuous variables and proportions for categorical variables. Student's t-test and Chi-square analysis were employed to identify continuous and categorical variables, respectively, associated with +ΔSI vs ΔSI ≤0. Binary logistic regression models, adjusting for age, Injury Severity Score (ISS), and Glasgow Coma Scale (GCS), were used to evaluate the relationship between clinical outcomes, blood requirement, and ΔSI. Statistical analyses were performed using JASP (Version 0.18.2.0).
Results
Descriptive Statistics of Age, HLOS, ILOS, GCS, ISS, and Ventilator Days Between Patients With a +ΔSI Versus Patients With a ΔSI ≤ 0
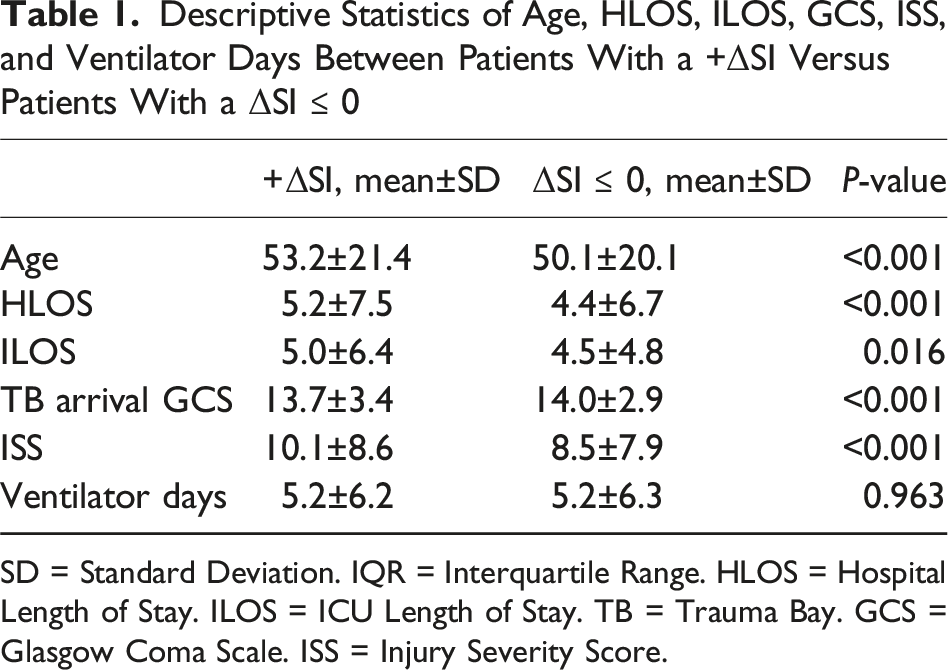
SD = Standard Deviation. IQR = Interquartile Range. HLOS = Hospital Length of Stay. ILOS = ICU Length of Stay. TB = Trauma Bay. GCS = Glasgow Coma Scale. ISS = Injury Severity Score.
Patients with a +ΔSI had a significantly higher mortality rate (6.8% vs 3.6%, P < 0.001). Patients with a +ΔSI also demonstrated a significantly higher need for blood transfusions (14.5% vs 9.7%, P < 0.001) and a higher rate of discharge to a care facility (23.0% vs 18.2%, P < 0.001) (Figure 1). Inferential statistics of outcomes between patients with a +ΔSI versus patients with a ΔSI ≤ 0. *= P < 0.001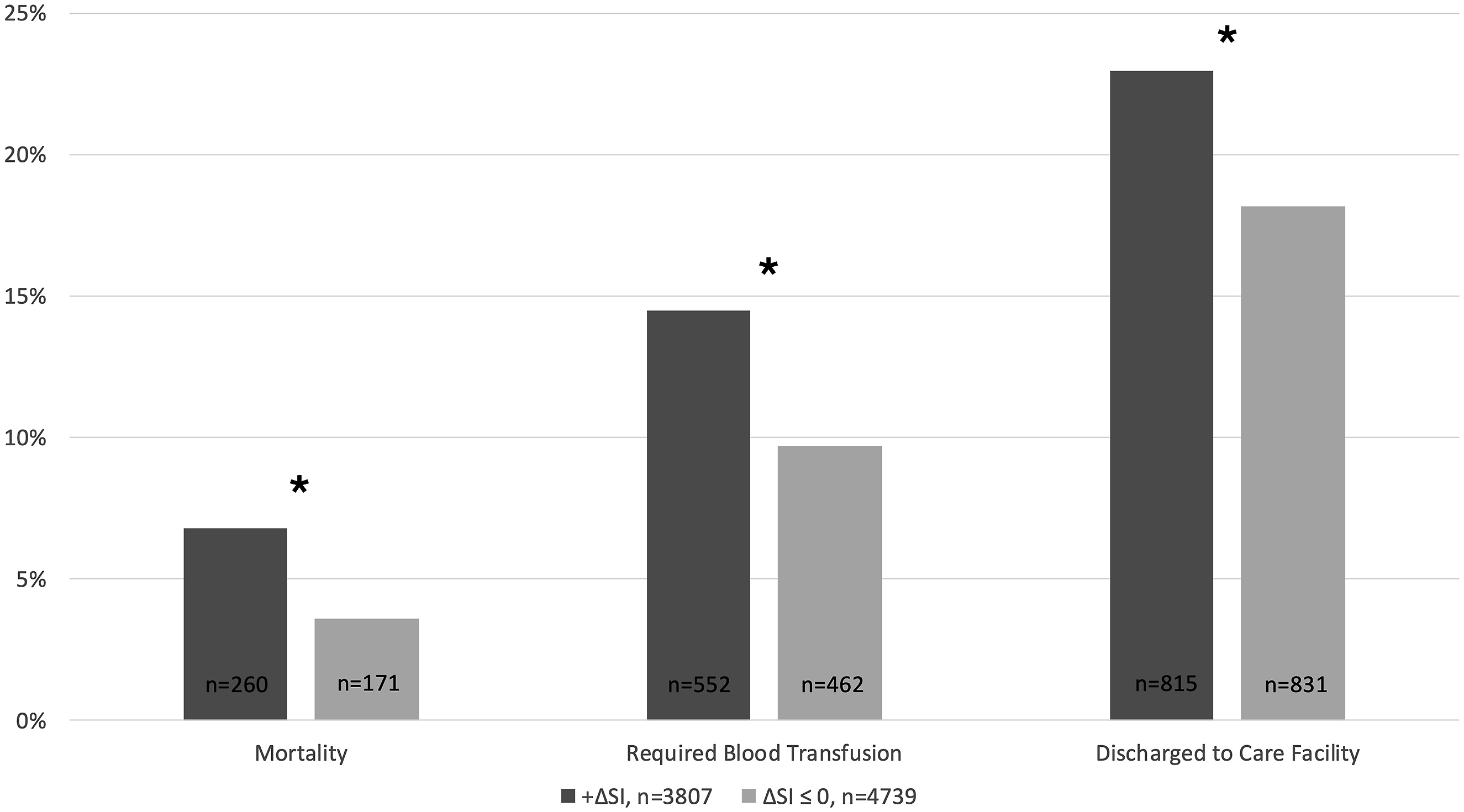
Binary Logistic Regression Showing Odds of Early Mortality
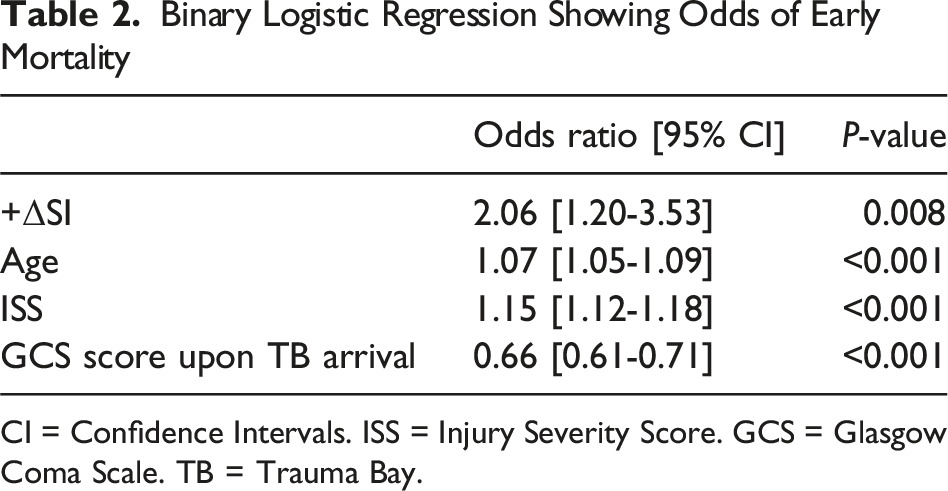
CI = Confidence Intervals. ISS = Injury Severity Score. GCS = Glasgow Coma Scale. TB = Trauma Bay.
Binary Logistic Regression Showing Odds of Overall Mortality
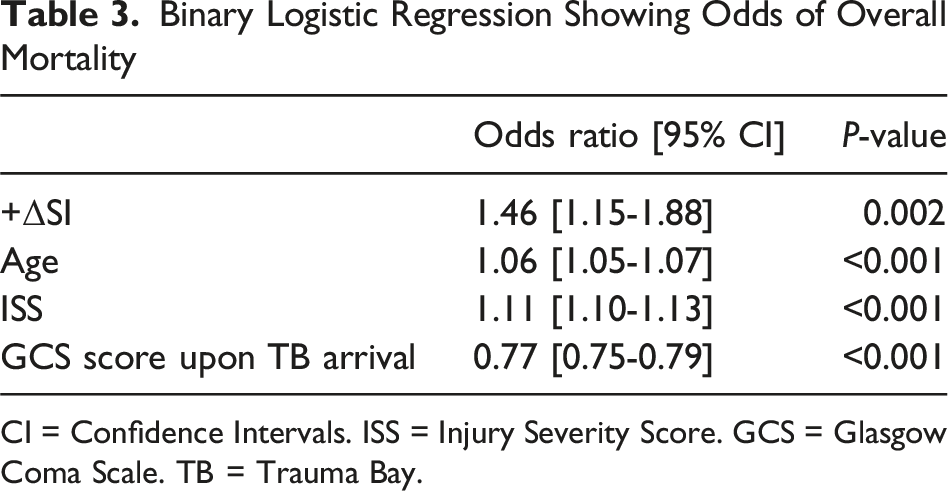
CI = Confidence Intervals. ISS = Injury Severity Score. GCS = Glasgow Coma Scale. TB = Trauma Bay.
Discussion
This study, using data from a rural state-designated level 1 trauma center serving more than 1.2 million people in the South-Central Appalachian region, confirms previous findings regarding ΔSI’s association with clinical outcomes and demonstrates the potential that ΔSI has as a predictive value in the rural setting. We found that +ΔSI is associated with increased HLOS and ILOS, lower GCS on arrival to the TB, higher ISS, increased blood transfusion needs, and increased discharge to care facilities in our patient population. Most notably, +ΔSI is associated with more than twice the odds of early mortality and almost 1.5 times the odds of in-hospital mortality.
A recent urban multicenter, retrospective, observational study observed significantly increased mortality, HLOS, ILOS, and need for blood transfusions among patients with an elevated ΔSI. 7 These results correlate with our study, which was undertaken in a rural environment. In contrast to previous studies that have focused on a ΔSI > 0.1, our study looked at patients with any positive ΔSI value. Despite our study’s lower threshold for ΔSI, we also demonstrated worse mortality and other adverse outcomes.
Though we did not compare the efficacy of ΔSI over SI, the literature demonstrates that ΔSI has superior predictive accuracy for in-hospital mortality, prolonged ICU stay, and major injury over both prehospital SI and ED SI. 11 ΔSI also has the added benefit of predicting outcomes in patients with normal vital signs and SI, who initially appear hemodynamically stable. 8
Older age and higher ISS were consistently linked to a +ΔSI, emphasizing its continued role in identifying patients at a greater risk of adverse outcomes, such as increased mortality and need for blood transfusion. A paper by McNab et al demonstrated that this association between increased SI and poorer outcomes holds for patients up until the 8th decade of life. 12 Funabiki et al highlight a significantly higher need for emergency surgery in blunt trauma patients ≥65 years old with an ΔSI >0.1 compared to those with an ΔSI ≤0.1. 9 These papers support the versatility of ΔSI as a predictive tool, since it can be used across all adult age groups.
This study’s binary logistic regression analysis further substantiates the predictive value of ΔSI. The increased odds of early mortality and in-hospital mortality associated with +ΔSI align with previous findings in critically ill patients. 5 This statistical validation underscores ΔSI’s utility as a dynamic parameter for risk stratification, complementing traditional risk factors like age and ISS. The higher mortality rate and increased need for blood transfusion among patients with +ΔSI mirror the conclusions drawn in previous studies and expand them to include patients served in rural areas, highlighting ΔSI’s consistency in predicting adverse outcomes. 6
Limitations of the study include those of a single-institution, retrospective study. Additionally, this study does not take into account the role of time, distance to hospital, and EMS and referring hospital intervention, all factors that play a major role in rural trauma care, on ΔSI. The literature demonstrates an improvement in ΔSI from scene to hospital when patients receive prehospital blood products.13,14 Though these patients receiving prehospital blood products had lower estimated odds of survival, there were more unexpected survivals and fewer unexpected deaths in this group compared to patients who did not receive prehospital blood products. 13
Future studies should seek to evaluate ΔSI in the rural setting in the context of time, distance, and EMS and referring hospital intervention. Further research is also warranted to elucidate its precise clinical utility and integration into routine practice for optimizing patient care, outcomes, and resource utilization. Prospective studies with larger sample sizes and standardized protocols are needed to validate the findings and further establish ΔSI as a reliable predictor of mortality and clinical outcomes across different patient populations and healthcare settings.
Overall, this study contributes to the growing body of evidence supporting ΔSI as a valuable prognostic indicator in trauma care. More importantly, it demonstrates the utility of ΔSI in the rural environment, which is often complicated by a longer distance to hospital and transport times. ΔSI has the potential to direct early interventions that might improve patient outcomes: if the EMR detects a positive ΔSI, healthcare providers could be alerted and faster administration of treatment could be executed. In addition to the original purpose of real-time assessment of hemodynamic instability, SI and the associated ∆SI have become valuable tools in not only predicting adverse outcomes across rural trauma, critical care, and emergencies but also in providing an adjunct in clinical decision-making. As healthcare continues to evolve, the integration of ΔSI into routine assessments holds the potential to enhance patient outcomes through proactive management strategies tailored to individual risk profiles.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.