
Abstract
Objective
Traumatic pseudoaneurysms are a serious complication following blunt and penetrating trauma, carrying a significant risk of morbidity and mortality if ruptured. However, there is a lack of specific guidelines for their detection and surveillance. This study aimed to evaluate the detection and management of posttraumatic solid organ pseudoaneurysms.
Materials and Methods
A prospectively maintained database was created at a Level 1 trauma center from January 2023 to June 2024. All patients aged 15 years and older who presented with a high-grade liver, kidney, or spleen injury were included in the study. Univariate data analyses was utilized with P < 0.05 considered statistically significant.
Results
Two hundred and five patients were included in the study. Pseudoaneurysms were identified in 10.7% of patients (n = 22/205). Gunshot wounds (n = 8/22, 36.4%) and motor vehicle collisions (n = 7/22, 31.8%) were the most common mechanisms of injury. Pseudoaneurysms were identified in the liver (n = 10/22, 45.5%), spleen (n = 9/22, 40.9%), and kidney (n = 3/22, 13.6%). 90.9% (n = 20/22) of pseudoaneurysms were identified within 5 days of initial injury. Seventeen (n = 17/22, 77.3%) patients underwent endovascular embolization for pseudoaneurysm repair with an 88.2% success rate. Five (n = 5/22, 22.7%) patients with pseudoaneurysms were managed by observation alone with no intervention. Overall, 48.3% (n = 99/205) of patients had a follow-up abdominal CTA prior to discharge.
Conclusion
Abdominal CTAs provide adequate surveillance for post-traumatic abdominal pseudoaneurysms, allowing for timely repair to decrease the risk of mortality from pseudoaneurysm rupture. Future prospective multi-center studies are needed to establish evidence-based guidelines for pseudoaneurysm detection and management.
Introduction
Solid organ injuries of the liver, kidney, and spleen are common sequelae of both blunt and penetrating abdominal trauma that are associated with significant morbidity and mortality. 1 Pseudoaneurysms result from injury to an arterial wall, forming a hematoma that communicates with the arterial lumen and is contained by the vessel media or adventitia. 2 Solid organ pseudoaneurysms occur in up to 10% of patients treated for blunt or penetrating trauma, 3 and the incidence of solid organ pseudoaneurysm formation has been shown to increase with increasing organ injury grade. 4
Depending on their location, symptoms associated with these arterial injuries can be highly variable. 5 However, pseudoaneurysms are often asymptomatic and may go undetected unless found incidentally on imaging. 5 If undetected and left untreated, pseudoaneurysms have the potential to rupture and cause life-threatening hemorrhage.2,6 Mortality from pseudoaneurysm hemorrhage has been cited to be as high as 12.5%-50% depending on their diameter and location.7-9 For this reason, pseudoaneurysms pose a unique challenge in the treatment of patients with traumatic injuries. If correctly identified, pseudoaneurysms can undergo endovascular repair with success rates cited at 85.7%, thus preventing life threatening complications from untreated pseudoaneurysms.7,8
Pseudoaneurysms are commonly identified by computed tomography (CT) due to its high diagnostic accuracy, detailed anatomic information, and precise localization.2,10,11 These arterial injuries may be identified on initial imaging but are often noted to have a delayed presentation requiring follow-up imaging for identification. 12 This delayed presentation and risk of high morbidity if ruptured has increased consideration for the use of follow-up imaging to help detect pseudoaneurysm formation in high-risk patients.3,13,14 Standardized surveillance imaging guidelines for pseudoaneurysm detection in high-risk patients could help decrease the number of untreated pseudoaneurysms and minimize the risk of delayed complications. 3 Existing literature on posttraumatic pseudoaneurysms is lacking and largely comprised of case reports. Currently, there are no consensus guidelines in place regarding the use of a surveillance protocol for posttraumatic pseudoaneurysms. To expand upon the current literature and promote value-based care, this prospective study aimed to evaluate the detection and treatment of posttraumatic solid organ pseudoaneurysms. We hypothesize that abdominal CT angiography (CTA) can be utilized as an effective screening modality for the detection of pseudoaneurysms formation in high-grade solid organ injuries following blunt or penetrating trauma.
Methods
Patient Population
This study was approved by the Louisiana State University Health Sciences Center Institutional Review Board (LSUHSC IRB) and a waiver of consent was obtained. A prospectively maintained database was created at a single Level 1 trauma center to identify and follow pseudoaneurysm development after blunt or penetrating abdominal trauma. The study included all patients aged 15 years and older who presented to the study site between January 2023 and June 2024 with a high-grade (III, IV, or V) liver, kidney, or spleen injury noted on initial CT. Children under the age of 15 years old, pregnant women, and prisoners were excluded from the study. All liver, kidney, and spleen injuries were graded using the 2018 American Association for the Surgery of Trauma Organ Injury Scale (AAST-OIS). 15 The injury severity score (ISS) was used to standardize the severity of traumatic injury. 16 Medical record review included patient demographics, clinical outcomes, and injury data. Injury data collected included mechanism of injury, organ injury grade, and pseudoaneurysm identification and treatment. Patient charts were reviewed for an additional 30 days following their discharge to identify any complications or the need for additional intervention. Clinical outcomes of interest included hospital length of stay (HLOS), intensive care unit length of stay (ICULOS), in-hospital mortality, and re-admission within 30 days of discharge.
Pseudoaneurysm Identification and Management
All patients included in the study presented to the study site following a traumatic injury and were evaluated using CT imaging on the day of presentation. All pseudoaneurysms were initially identified on contrast enhanced CT imaging either on the day of presentation or on subsequent CT scans. On contrasted CT imaging, pseudoaneurysms were identified as well-defined, rounded areas with contrast enhancement equal in attenuation to surrounding arterial structures
5
(Figure 1A). On delayed imaging, pseudoaneurysms demonstrated washout similar to surrounding arterial structures.
5
Imaging findings concerning for suspected pseudoaneurysm were considered for additional evaluation using either repeat CT or procedural angiography at the discretion of the provider (Figure 1B). Pseudoaneurysms identified on either initial or follow-up CT imaging or angiography were evaluated for endovascular repair. Endovascular repair was performed by fellowship trained interventional radiologists using stents or coils (Figure 1B). Patients with small pseudoaneurysms, typically described as less than 10 mm in diameter, were considered for conservative management by observation alone at the discretion of the provider.
17
34 year Old Man Presented to the Hospital Following a Motor Vehicle Collision. CT on Admission Showed a Benign Spleen With No Active Bleeding. (A) Follow-Up Imaging Obtained 4 days after Admission Showed Multiple Splenic Artery Pseudoaneurysms. (B) Procedural Angiography Confirmed the Presence of Multiple Splenic Artery Pseudoaneurysms. (C) Endovascular Pseudoaneurysm Repair was Performed Using Superselective Embolization With Coils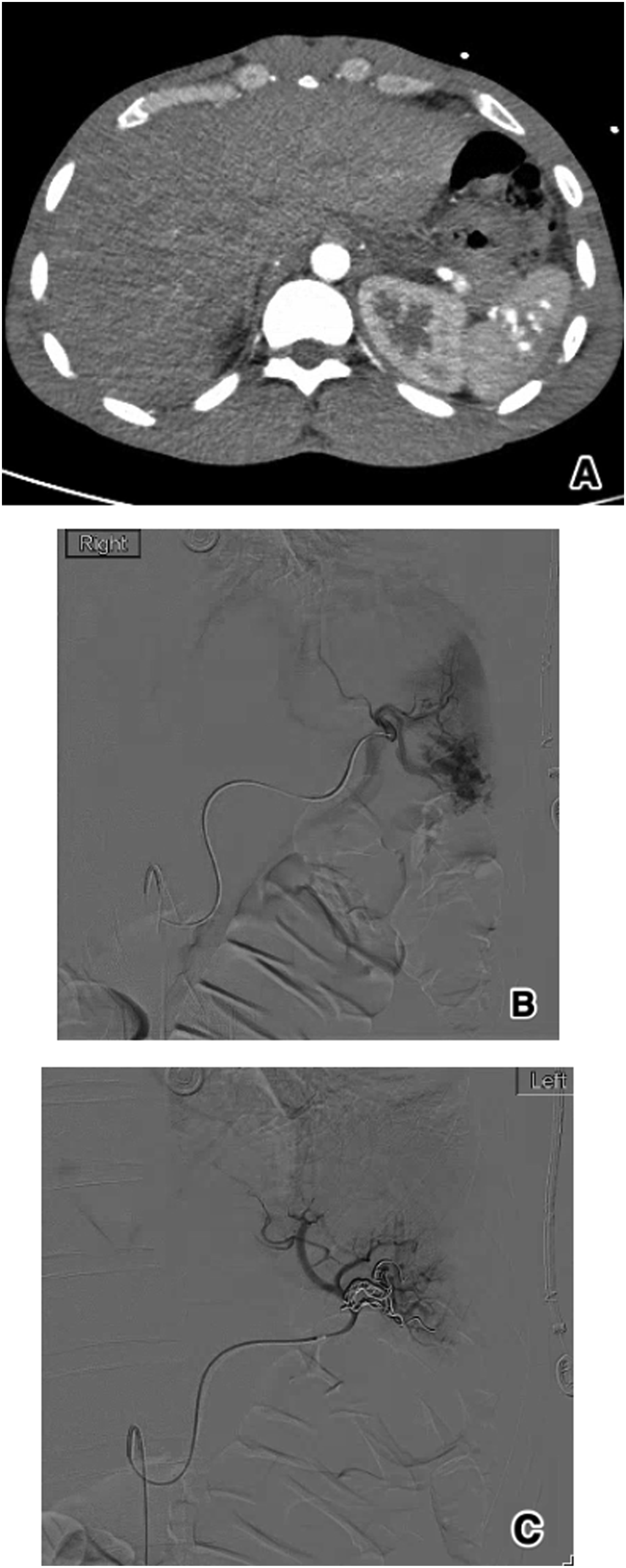
Statistical Analysis
Data was analyzed using the SAS/STAT software, version 9.4 of the SAS System for PC (SAS Institute Inc, Cary, NC, USA). Demographic and clinical characteristics and outcomes were compared between patients without (NO-PSA) and with Pseudoaneurysm (PSA). Categorical variables were compared using either the Exact test for cell counts less than 5 or the Chi-Square test for cell counts of 5 or more. Continuous variables were compared using either the t test, if assumptions were met, or the Mann-Whitney U-test. For parametric analysis, continuous variables are summarized using means and standard deviation, and for non-parametric analysis, they are presented as the median (interquartile range, IQR). Statistical significance was defined as P < 0.05.
Results
Patient Population
Demographical and Clinical Characteristics in Patients Without (NO-PSA) and With Pseudoaneurysm (PSA)
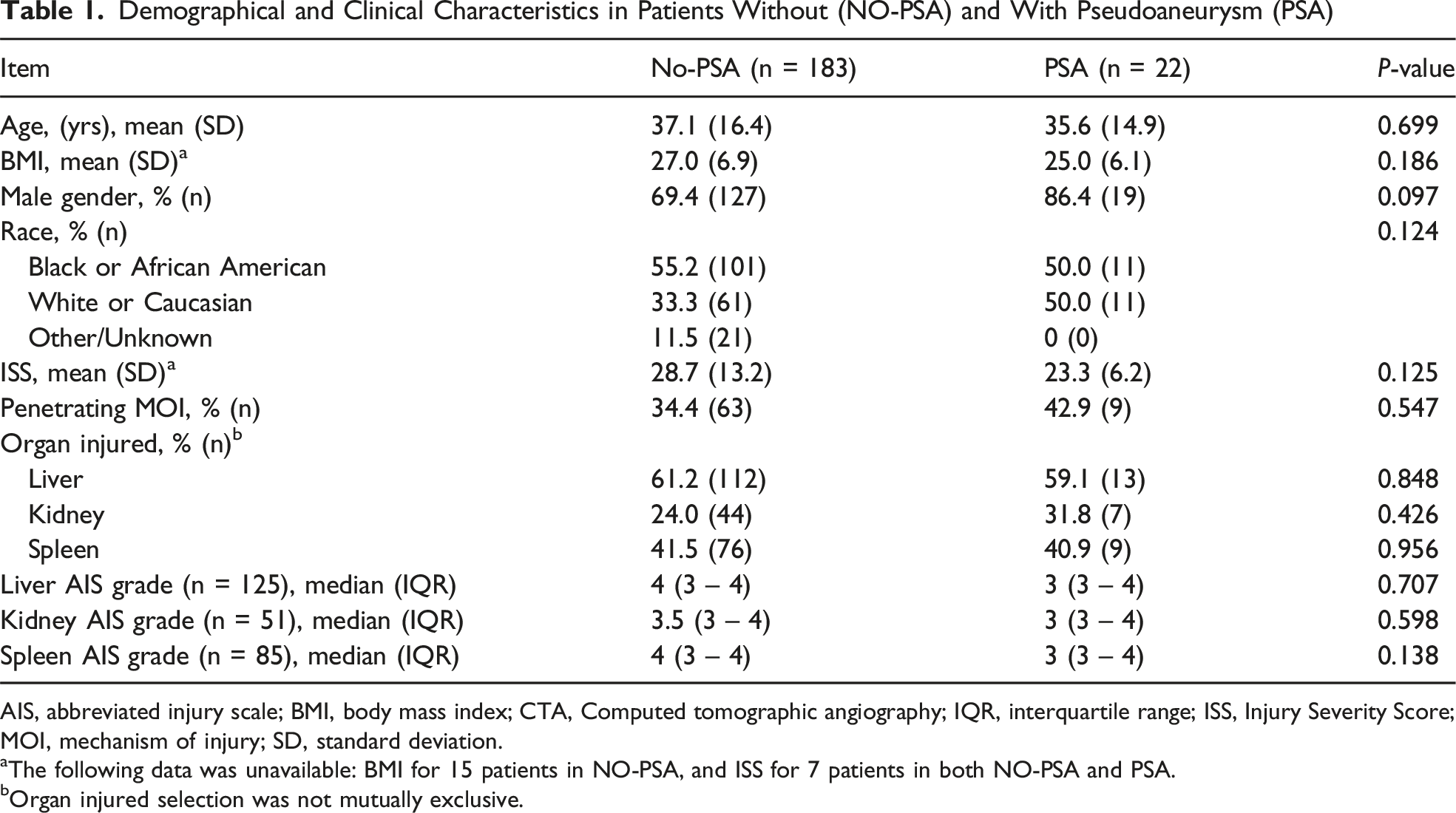
AIS, abbreviated injury scale; BMI, body mass index; CTA, Computed tomographic angiography; IQR, interquartile range; ISS, Injury Severity Score; MOI, mechanism of injury; SD, standard deviation.
aThe following data was unavailable: BMI for 15 patients in NO-PSA, and ISS for 7 patients in both NO-PSA and PSA.
bOrgan injured selection was not mutually exclusive.
Outcomes
Univariable Comparison of Clinical Outcomes in Patients Without (NO-PSA) and With Pseudoaneurysm (PSA)
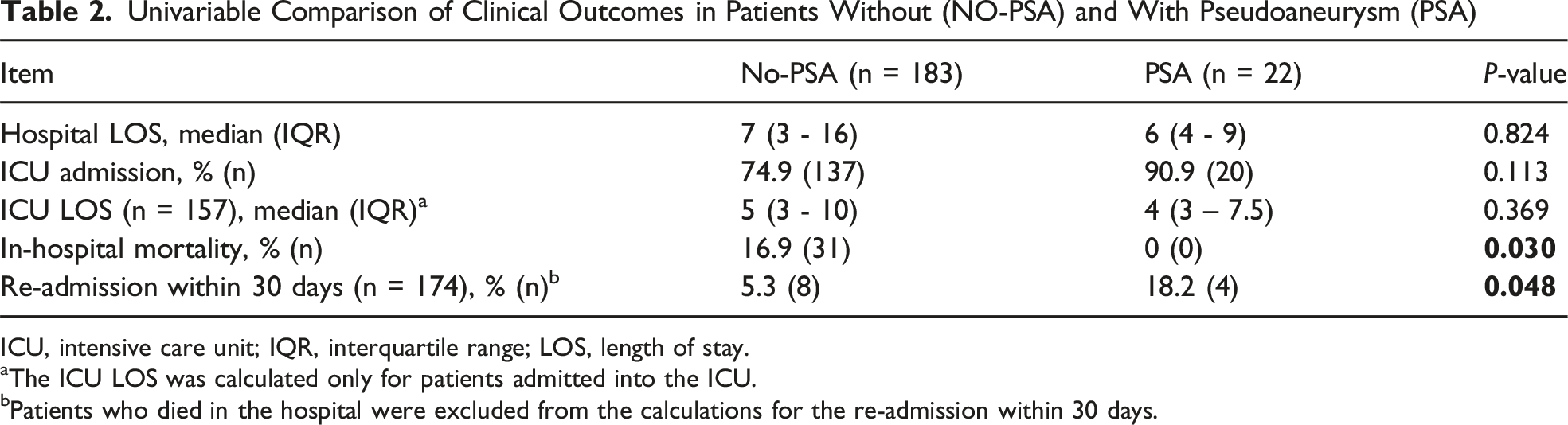
ICU, intensive care unit; IQR, interquartile range; LOS, length of stay.
aThe ICU LOS was calculated only for patients admitted into the ICU.
bPatients who died in the hospital were excluded from the calculations for the re-admission within 30 days.
Pseudoaneurysm Development
Pseudoaneurysms were identified in 10.7% of patients (22/205). Pseudoaneurysms were identified in the liver (45.4%, 10/22), spleen (40.9%, 9/22), and kidney (13.6%, 3/22). Multiple pseudoaneurysms were identified within one organ in 8 patients (36.4%, 8/22), with no patients having pseudoaneurysms in more than one organ. Five patients (22.7%) had pseudoaneurysms identified on initial CT. Patients with identified pseudoaneurysms had a significantly greater percentage of patients with follow-up abdominal CTAs performed prior to discharge compared to patients who had no identified pseudoaneurysm (90.9% vs 43.1%, P < 0.0001).
Pseudoaneurysm (PSA) Identification, Intervention, and Injury Mechanism
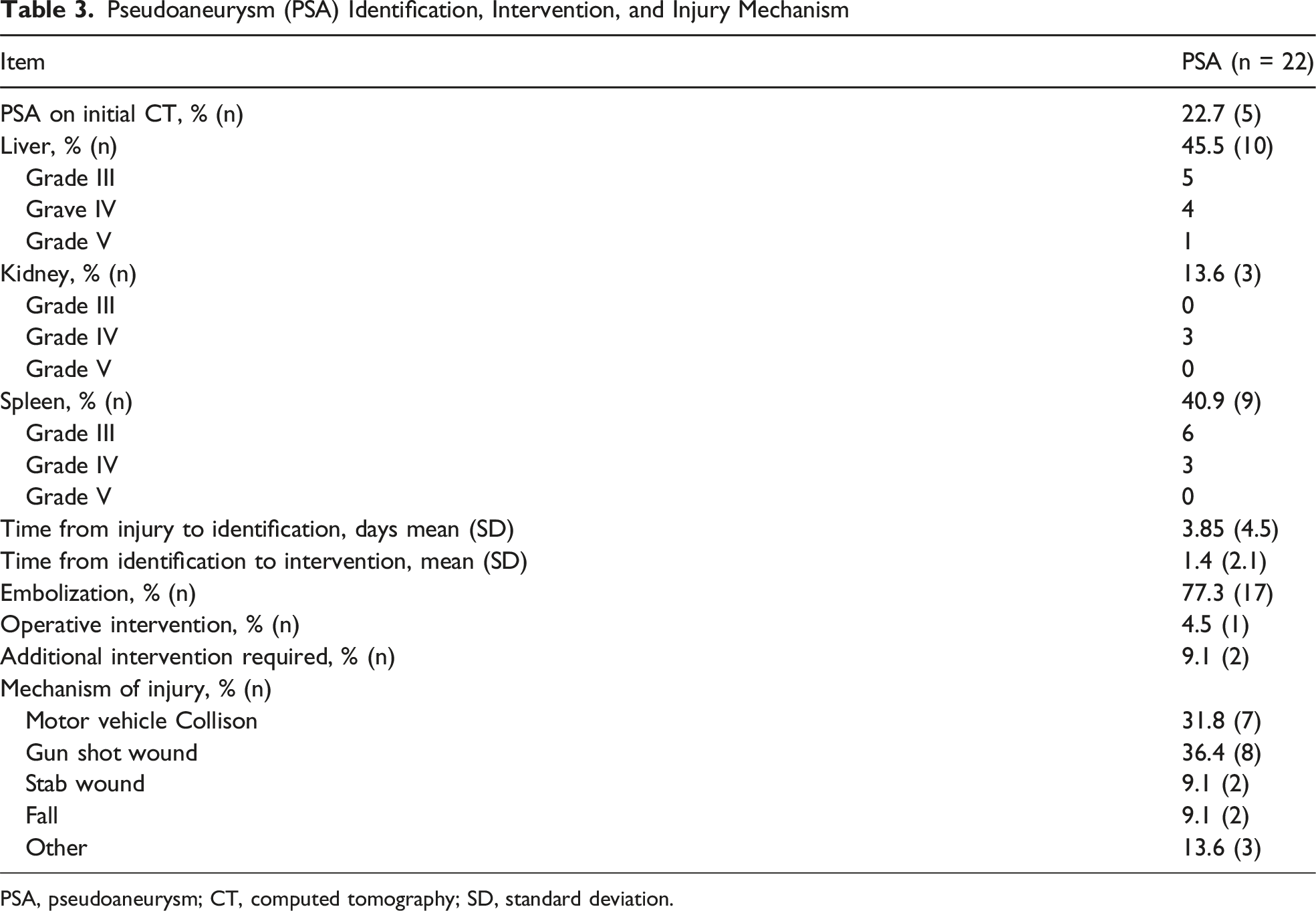
PSA, pseudoaneurysm; CT, computed tomography; SD, standard deviation.
Discussion
In this study we observed a pseudoaneurysm formation rate of 10.7% among patients with high-grade solid organ injuries (grade III-V) resulting from both blunt and penetrating trauma. This is slightly higher than the 3.7%–10% rate of pseudoaneurysm detection reported in the literature which we believe to likely be a result of increased follow up imaging.3,4,14 At our institution, increased attention to pseudoaneurysm formation and detection resulted from a patient who presented with life-threatening hemorrhage from the rupture of an undetected pseudoaneurysm. In our study, 48.3% of patients underwent a follow-up CTA prior to discharge. In a similar study that reported a pseudoaneurysm formation rate of 3.7% only 25.5% of patients had a follow-up CTA prior to discharge. 14 Consequently, the thought that pseudoaneurysms are a rare sequelae of traumatic injury may be influenced by lack of detection.
In multiple ways, the findings of our study differed from what has been previously identified in the small amount of literature currently available on post-traumatic pseudoaneurysm formation, likely representing a lack of awareness of pseudoaneurysm development and disease course. Our study identified the liver as the most commonly involved organ (45.4%), followed by the spleen (40.9%) and kidney (13.6%). This differs from the currently available literature which reports splenic pseudoaneurysm formation as the most prevalent.14,18 One study has noted a predominance of liver pseudoaneurysm formation over the kidney or spleen in patients with penetrating trauma. 19 The incidence of pseudoaneurysm formation has been noted to increase in parallel to increased injury grade. 4 This was not consistent with the findings of our study. Our study found a similar incidence of pseudoaneurysm formation in grade III (50%) and grade IV (45.5%) injuries, with grade V injuries representing only 4.5% of pseudoaneurysm formation. These findings may indicate a need for surveillance imaging in all high-grade solid organ injuries, as pseudoaneurysm formation has not been shown to consistently correlate with injury grade, location, or mechanism of injury. Our study did find that in-hospital mortality was significantly higher in patients who did not develop pseudoaneurysms. This finding is believed to be due to mortality occurring from polytrauma or other complications prior to pseudoaneurysm formation or follow-up imaging. Re-admission within 30 days was higher in patients who developed pseudoaneurysms, although no patients were re-admitted due to complications from pseudoaneurysm formation. Pseudoaneurysm complication or rupture was not identified as a cause of mortality or re-admission in any patient in our study.
Delayed pseudoaneurysm formation has been well document in the literature through numerous case-reports detailing this finding in vessels throughout the body. Although the exact pathophysiology behind delayed pseudoaneurysm presentation has yet to be identified, theories have been described in the literature. One explanation being that continued arterial pressure on an initially small defect causes an expanding vascular injury that eventually becomes large enough to be visible on repeat imaging. 12 Interval clot lysis at the site of vessel wall injury between scans may also allow for better visualization of contrast blush on repeat imaging. 12 Additionally, delayed identification may be a result of imaging techniques missing already present pseudoaneurysms due to contrast timing, smaller size on initial imaging, or other technical considerations rather than true delayed pseudoaneurysm formation. 12 Although delayed formation of pseudoaneurysm has been identified as far as 6 weeks from the inciting incident, 20 our study identified 90.9% of pseudoaneurysms within 5 days of the traumatic injury. Based on this finding, follow-up imaging for pseudoaneurysm surveillance could be obtained before discharge allowing patients to undergo pseudoaneurysm repair within the same hospital stay. This approach may help to reduce the number of patients lost to follow-up, decrease the rate of re-admission for symptomatic pseudoaneurysms, and decrease costs for patients and hospitals.
Endovascular repair was completed in 77.3% of patients with pseudoaneurysm formation with an overall success rate of 88.2% which is similar to the current literature. 7 Endovascular repair is evolving as the best treatment option for posttraumatic solid organ pseudoaneurysms, although the conventional method of open surgical repair may still be considered in the setting of emergent pseudoaneurysm rupture. 21 In addition, 22.7% of patients with pseudoaneurysm development were managed conservatively with observation alone without any complication. This coincides with a growing body of evidence that small pseudoaneurysms (<10 mm) may regress spontaneously and can be managed conservatively with observation alone.3,17 However, the outcome of conservative management remains unpredictable as delayed rupture has not been shown to correlate with the initial CT findings. 22 Although the current understanding of posttraumatic pseudoaneurysm remains limited, our study builds upon the existing literature by adding clinical insight into the detection, management, and outcomes of posttraumatic abdominal pseudoaneurysms.
This study is not without limitations, including the single-center design and relatively small sample size. Further research with larger sample sizes and multi-center data are needed to validate the effectiveness of routine surveillance imaging in improving clinical outcomes and reducing morbidity and mortality. Establishing consensus guidelines for surveillance imaging in high-risk patients could help optimize the detection and management of pseudoaneurysms.
Conclusion
This study demonstrates that abdominal CTA is an effective tool for the early detection and management of posttraumatic solid organ pseudoaneurysms. Our findings suggest that increased surveillance with abdominal CTA may lead to increased detection of pseudoaneurysm formation, allowing for timely intervention to reduce the risk of life-threatening rupture. Further multi-center prospective studies are needed to establish evidence-based guidelines for the detection and management of posttraumatic pseudoaneurysms.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AAS is a paid consultant for Aroa Biologics and on the advisory board for Prytime Medical. The remaining authors declare no potential conflicts of interest with respect to the research, authorship, and/ or publication of this article.