
Abstract
Background
Unplanned hospital readmissions within 30 days of discharge for trauma (UR-30) are associated with adverse outcomes but remain underexplored in trauma populations.
Methods
This study retrospectively reviewed 164 trauma patients at a Level I center during 2022-2023, analyzing demographics, comorbidities, injury severity, socioeconomic factors, medications, and hospital events. Propensity matching ensured comparability between 82 UR-30 and 82 patients not readmitted (NoReadmission-30).
Results
Key findings include median hospital length of stay (LOS) of 5 days for UR-30 vs 3 days for NoReadmission-30 (P = .022) and ICU LOS of 2 vs 0 days (P < .001), respectively. Final in-hospital hemoglobin was lower in UR-30 (10.7 vs 12; P = .014). Discharge home rates were lower for UR-30 (51.2% vs 69.5%; P = .017). Transfusion requirements significantly increased readmission risk, with UR-30 patients 6.7 times more likely to be readmitted. Significant comorbidities included smoking (P = .042), hyperlipidemia (P = .012), CHF (P = .013), substance use disorder (P = .043), and ≥3 comorbid diagnoses (P = .001). Most readmissions were for infections, neurological decline, and inadequate pain control. Discharge on anticoagulants (P = .007) or with ≥7 discharge medications (P < .001) increased readmission likelihood, while chronic NSAID use reduced it (P = .046). Family as PoA was more common in UR-30 (83% vs 40%; P < .001). Non-significant factors included discharge vital signs, injury mechanism, insurance, and race.
Discussion
UR-30 occurs predominantly in moderately injured patients and is influenced by ICU and hospital LOS, discharge disposition, comorbidities, and transfusion status, underscoring its value as a trauma quality metric.
Key Takeaways
• Trauma patients with the following characteristics are at significant risk for readmission within 30 days: advanced age (>55 years), prolonged hospital and ICU stays, lower discharge hemoglobin levels, requiring transfusion during the index admission, history of CHF, hyperlipidemia, substance use disorder, smoking, ≥3 comorbidities, discharged on anticoagulation, ≥7 discharge medications, or those discharged to locations other than home. • The most common causes for readmission of trauma patients are infection, neurological decline, and inadequate pain control. • Patients with ≥3 comorbidities and ≥7 discharge medications are at a higher risk for readmission and may benefit from earlier follow-up with trauma services, specialty surgery, and/or their primary care physician.
Introduction
Trauma patient readmission within 30 days (UR-30) is a quality-of-care metric linked to adverse outcomes and increased healthcare costs. 1 In the United States, approximately 10% of trauma patients experience UR-30. Trauma-related readmission costs an average of $8000 per patient, resulting in $300 million annually in potentially preventable expenses. 2
Readmission risk in general medicine and select surgical populations have undergone study, but UR-30 in trauma remains underexplored. Among patients admitted to general medicine geriatric wards, Bortolani identified prolonged hospital stay (>14 days), low albumin (<30 g/L), reduced GFR (<40 mL/min), low systolic blood pressure (<115 mmHg), and cardiovascular diagnoses as predictors of readmission. 3 Sharma found COPD, bleeding disorders, diabetes, steroid use, ESRD, and current smoking status significantly contributed to readmission following ankle fracture repair. 4 Trauma patients face distinct challenges due to injury complexity, comorbidities, variable hospital courses, and social determinants of health, necessitating an improved understanding of why trauma patients return with early and/or preventable readmission.
Harcombe, in a study of index trauma admissions, reported a UR-30 rate of 15%, identified risk factors of age >65 and comorbidities, and found those with a longer initial LOS were less likely to experience UR-30 compared to those admitted for less than one day following major trauma. 5 Copertino reported a UR-30 rate of 6.57% in trauma patients, identifying chronic illness and discharge to SNF as risks. 6 In patients hospitalized following blunt trauma, penetrating trauma, or burns, Lunardi found a UR-30 rate of 11.1%, linking male gender, socioeconomic status, and prolonged LOS to readmission. 7 Olufajo found musculoskeletal complaints, psychiatric conditions, and surgical infections as common reasons, with social and health vulnerabilities amplifying risk in index trauma admissions. 8 Neiman suggested that 22.7% of trauma readmissions within 90 days were preventable and highlighted chronic comorbidities as key contributors. 2 While these studies provide valuable insight, research with a comprehensive set of variables that could help identify additional high-risk indicators, guide strategies to reduce UR-30 rates, and improve outcomes and costs in the trauma population is largely absent.
Our goal was to support previously postulated contributors and define a more comprehensive set of variables associated with UR-30 for trauma treated at Level I centers. We propose to provide actionable insights guiding the development of inpatient and post-discharge strategies to reduce early, potentially preventable readmission.
Methods
This study was approved by the East Tennessee State University and Ballad Health Institutional Review Boards (IRB# 00003204).
Our retrospective, propensity-matched study investigated UR-30 at a Level I trauma center in 2022-2023. UR-30 was defined as any trauma patient experiencing UR-30 following inpatient discharge. Exclusion criteria were age <18 years, lateral transfer, or prearranged readmission. We excluded patients who returned only to the emergency department without readmission. UR-30 patients were compared to propensity-matched controls who did not experience UR-30 (NoReadmission-30). Propensity matching was based on age, gender, Injury Severity Score (ISS), and top two Abbreviated Injury Scale (AIS) scores to promote comparability and minimize confounding variables.
Data collected included demographics, home medications, comorbidities, mechanism of injury, ISS, AIS, and details of hospital course, such as hospital length of stay (LOS), ICU LOS, transfusion requirements, and initial vitals. Additional variables were discharge vitals, discharge hemoglobin level, discharge medications, discharge disposition, and readmission diagnosis. The primary evaluation criteria focused on identifying factors associated with UR-30 compared to NoReadmission-30.
Descriptive statistics for categorical variables were reported in frequency and percentages; continuous variables were reported using mean and standard deviation or medians with interquartile range. Categorical variables were analyzed using the chi-square test, and statistically significant variables were reported with odds ratio (OR) and 95% confidence interval ([95% CI]). Continuous variables were analyzed for homogeneity. Normally distributed variables were further analyzed using an independent sample t-test, and statistically significant variables were reported using mean and standard deviation (mean ± SD). Nonhomogeneous variables were analyzed using the Mann-Whitney U test, and statistically significant variables were reported using the median and interquartile range (median [IQR]). Statistical significance was determined using P < 0.05. Data analysis was performed on SPSS-28 (Armonk, NY: IBM Corp.).
Results
AIS Injury Patterns for UR 30 vs NoReadmission-30 Controls
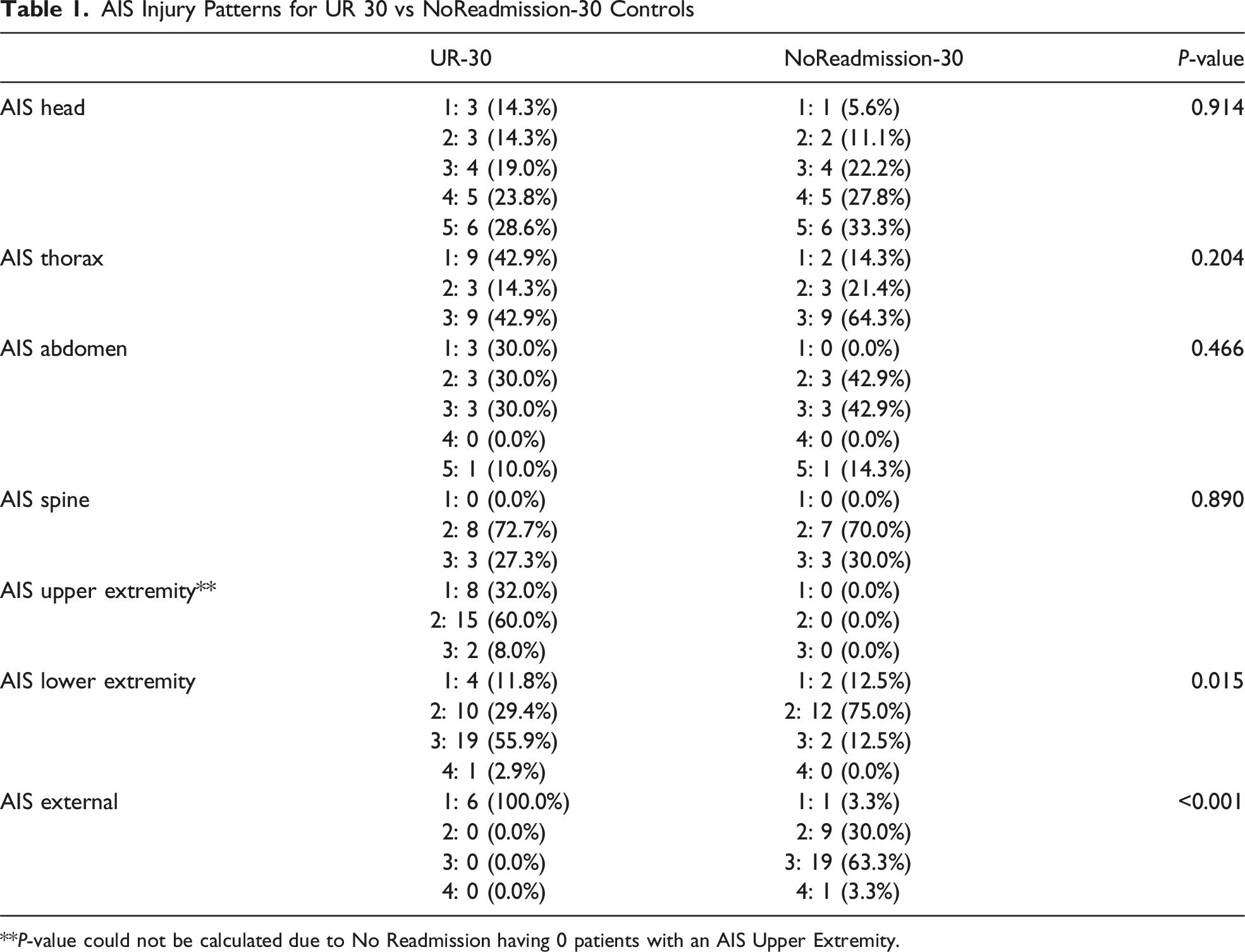
**P-value could not be calculated due to No Readmission having 0 patients with an AIS Upper Extremity.
Comparison of Selected Variables for UR-30 vs NoReadmission-30 Controls
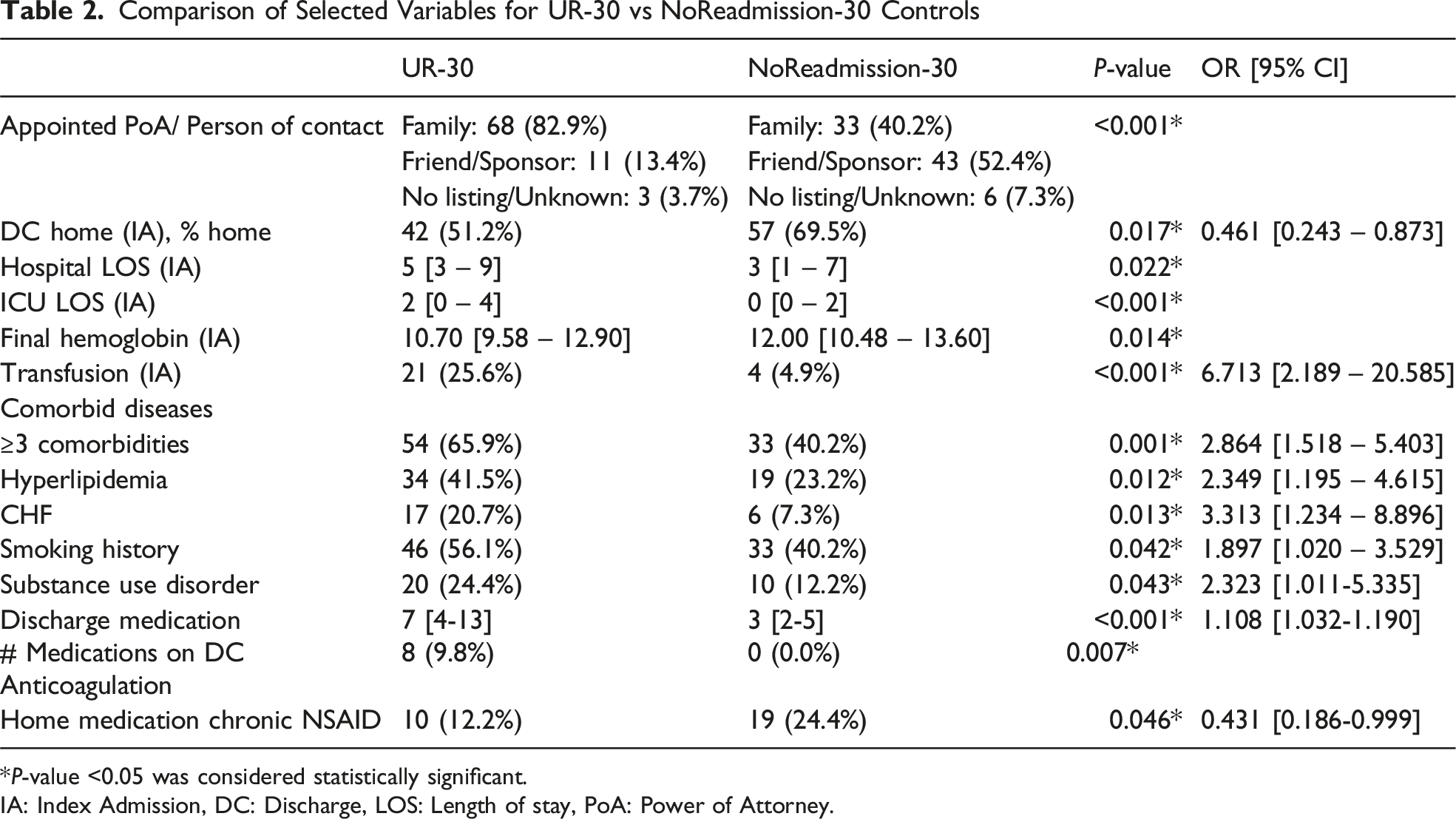
*P-value <0.05 was considered statistically significant.
IA: Index Admission, DC: Discharge, LOS: Length of stay, PoA: Power of Attorney.
The UR-30 group had longer hospital LOS (5 days [3-9] vs 3 days [1-7], P = .022) and ICU LOS (2 days [0-4] vs 0 days [0-2], P < .001). UR-30 patients had lower final hemoglobin levels at discharge (10.7 g/dL [9.58-12.90] vs 12 g/dL [10.48-13.60], P = .014) and had 6.713 [2.189-20.585] times higher odds of having received a transfusion during their admission (P < .001) (Table 2).
Comorbidities associated with an increased risk of UR-30 included a past medical history of CHF (P = .013, OR = 3.313 [1.234-8.896]), hyperlipidemia (P = .012, OR = 2.349 [1.195-4.615]), substance use disorder (P = .043, OR = 2.323 [1.011-5.335]), and smoking history (P = .042, OR = 1.897 [1.020-3.529]). In addition, 3 or more comorbidities conferred an increased risk of UR-30 (P = .001, OR = 2.864 [1.518-5.403]) (Table 2). Comorbidities not achieving statistical significance in this study included PVD (P = .057), non-insulin-dependent diabetes (P = 1.000), insulin-dependent diabetes (P = .292), dementia (P = 1.000), hypertension (P = .160), CKD (P = .200), COPD ( P = .678), distant cancer history (P = .406), active cancer (P = 1.000), liver disease (P = .549), CVA/stroke (P = .807), VTE (P = .292), alcohol abuse (P = .807), history of MI (P = .152), atrial fibrillation/flutter (P = .292), depression (P = .450), anxiety (P = .359), impaired vision (P = .736), and impaired hearing (P = .579).
The UR-30 group was more likely to have a family member listed as their appointed PoA/person of contact compared to the control group (82.9% vs 40.2%, P < .001) (Table 2). Marital status, insurance type, and primary language were not statistically significant (P = .739, P = .734, and P = .12, respectively).
Patients in the UR-30 group had 1.108 [1.032-1.190] times higher odds of being discharged with an oral anticoagulant (P = .007) and being discharged with more total medications (7 [4-13] vs 3 [2-5], P < .001). Of the home medications analyzed, only chronic NSAID use had a 0.431 [0.186-0.999] times lower odds of UR-30 (P = .046). Home medications that were not statistically significant included anticholinergic inhalers (P = .129), inhaled corticosteroids (P = .412), gabapentin (P = .077), benzodiazepines (P = .609), trazodone (P = .723), skeletal muscle relaxants (P = .602), SSRIs/SNRIs (P = .535), beta-blockers (P = .448), ACE inhibitors (P = .267), aspirin (P = .534), subcutaneous heparin (P = 0.812), oral anticoagulants (.543), calcium channel blockers (.328), statins (P = .288), and PPIs (P = .647). Seventy-six (44%) of UR-30 patients were discharged to locations other than home to only 35 (30%) in the NoReadmission-30 group. This translated to a 0.461 [.243-.873] times lower odds of home discharge disposition (P = .017). Of the UR-30 patients, discharge disposition for index admission included skilled nursing facilities (n = 29, 17%), inpatient rehabilitation (n = 25, 14%), and correctional facilities (n = 3, 2%). Seven patients (9%) left against medical advice (AMA); therefore, the ultimate discharge location was indeterminate.
The most common diagnoses for readmission were wound infections (n = 18, 24%), neurological decline (n = 15, 20%), uncontrollable pain (n = 12, 16%), noninfectious wound complications (n = 8, 10%), return after leaving AMA (n = 7, 9%), noninfectious orthopedic care (n = 5, 7%), VTE (n = 4, 5%), hemorrhage (n = 4, 5%), and new injuries (n = 3, 4%).
Twenty (11.9%) patients in the full cohort were admitted to a nonsurgical service on their index admission. The average ISS for these patients was 8 vs 11 for patients admitted to the trauma service. Patients admitted to a nonsurgical service had .212 [.067-.664] times lower odds of UR-30 (P = .007), were less severely injured, and were predominantly composed of isolated geriatric hip fracture patients.
Discussion
UR-30 is an important Trauma Quality Improvement Program (TQIP) metric. While existing research has explored some risk factors for readmission, we sought to identify a more comprehensive set of variables that may predict UR-30 specific to trauma.
UR-30 in our cohort occurred predominantly amongst moderately injured patients (mean ISS = 9.8). We identified numerous significant predictors for UR-30. Our data concurs with previously cited literature across disciplines suggesting that patients at higher risk were more likely to exhibit the following: advanced age, higher comorbidity burden (particularly CHF, hyperlipidemia, and >3 comorbid diagnoses in our trauma population), smoking/ substance abuse history, longer hospital and ICU stays, and anticoagulants prescribed at discharge and discharged locations other than home.2-9
We also identified novel variables increasing risk of UR-30 specific to trauma:
Our patients had lower discharge hemoglobin levels (10 vs 12 gm/dl) and were at 6.7x increased risk of requiring transfusion during their index admission.
We explored potential influences of pharmacological agents and found that patients with UR-30 were discharged with an average of 7 medications vs 3 in NoReadmission-30 patients. This aligns with numerous publications citing polypharmacy, defined as greater than 5 concurrent medications, as an overall risk factor for adverse outcomes.10,11 Home NSAID use was associated with a reduced readmission risk (0.4x), suggesting protective effects, but this is not a modifiable risk factor.
With regard to social determinants, patients with a family member as their PoA had significantly increased readmission risk. Although we were unable to determine why, we postulate family members may detect subtle health changes prompting hospital return. Further social determinants, such as economic factors and access to medical care, are warranted but were not thoroughly investigated in this study.
Our findings beckon us to identify and intervene on any modifiable variable contributing to UR-30. Risk factors of advanced age, multiple and serious comorbidities such as CHF history, and seemingly rampant polypharmacy suggest the once-popular adage, “A surgeon is an internist who operates” does not hold true in today’s complex milieu of medical practice. Inpatient consultation and early post-discharge follow-up with primary care providers, inpatient pharmacologists, and gerontologists, particularly in frail and unwell patients, is a recommended prevention strategy for UR-30. TQIP guidelines now recommend inpatient consultation with teams experienced in geriatrics for all frail patients. 12 Embedding a trauma hospitalist has been shown to reduce mortality and readmission rates. 13
The most common cause of readmission in our investigation was wound complication, followed by neurological decline, and inadequate pain control, underscoring the importance of meticulous inpatient care, comprehensive discharge planning, and better targeted post-discharge follow-up.
Our wound complication findings align with Schipmann, who reported wound infections as a leading cause of unplanned readmission within 30 days for neurosurgery patients. 14 Rigorous attention to perioperative antibiotics, timing, and duration of administration is warranted, as well as intensified wound surveillance at and after discharge. The overall majority of wound infections in our study were orthopedic in nature. Specialty surgery team “sign off” after surgical intervention is completed is not an unusual practice in many trauma centers. This can lead to loss of inpatient follow-up as well as missed and/or unscheduled suggested follow-up appointment dates. This variable is modifiable and could potentially be assisted by coordinating with information technology to form reminders to specialists embedded in an EMR system. Additionally, patients with wounds should benefit from early post-discharge surveillance, either in-person or via video appointment. This could benefit not only those discharged home but also patients discharged to extended care where missed appointments sometimes occur. Saunders examined outpatient follow-up vs UR-30 for general and vascular surgery patients and made the following observation: Current routine follow-up does not occur early enough to detect adverse events and prevent readmission. Early outpatient care may prevent readmission in some patients but often serves as a conduit for readmission among patients already experiencing complications. 15
Readmission for neurological decline, our second most common cause of UR-30, is an area of nearly absent research. We postulate that earlier follow-up may prove beneficial, but there is currently no literature to support this proposition.
Another problematic area was post-discharge pain control. During a national opioid crisis, emphasis has been placed on early cessation of narcotics and multimodal strategies. However, authors such as Østli have emphasized that severely injured patients experience substantial pain in the first 2 weeks after trauma. 16 Inadequate pain control has been cited as a cause for return to the ED without readmission as well. 17 Determining an adequate prescription of pain medication for each individual remains challenging due to individual variability and the absence of definitive guidelines. Even where guidelines exist, such as those developed by the Orthopedic Trauma Association, implementation occurred only two-thirds of the time and did not reduce MEQs prescribed. 18
Our study has limitations related to its retrospective, propensity-matched design in a single center. Expanding the scope to include multicenter cohorts or collective national databases such as TQIP or the National Trauma Data Bank (NTDB) would improve the generalizability of findings across diverse trauma populations, although an inherent lack of granularity in such databases persists. A prospective, multicenter design would address the limitations of the accuracy of EMR and mitigate the impact of missing data.
Our chosen matching strategy to avoid confounding data eliminated age, gender, and overall ISS values as variables. Importantly, although we matched the two highest AIS scores, the contribution of lower-scoring extremity and external injuries, even when not the highest AIS, was likely undervalued as a predictor of readmission, represented an unintended bias, and certainly deserves a more careful analysis as to its contribution to UR-30.
We recommend future research investigate the variability in primary care and surgical follow-up practices and explore variables not fully evaluated in our work, including the role of social support systems.
Studies estimate that a quarter of readmissions are preventable. 2 Prevention is important for overall outcome, reduced morbidity, mortality, and healthcare savings. The findings of this study underscore the need for a multidisciplinary and early follow-up approach to inpatient care and discharge planning for all patients with known increased risk for UR-30. Suggested targeted interventions include implementing discharge navigator programs to enhance care coordination, scheduling earlier follow-ups, closer wound monitoring, better inpatient and outpatient comorbidity management, and ensuring comprehensive pain control, and availability of medications prior to discharge. Identifying high-risk trauma patients during hospitalization also allows for tailored predischarge education to patients and families. These strategies have the potential to improve patient outcomes, reduce readmission, and optimize resource utilization.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.