
Abstract
Background
Emergency general surgery (EGS) patients require surgical intervention and often critical care. Current literature suggests that interfacility transfer potentially face worse outcomes including increased mortality and complications. This study aims to evaluate patient transfers on mortality and the utilization of damage control laparotomy (DCL) in EGS.
Methods
Retrospective cohort study of patients undergoing emergent exploratory laparotomy at an academic institution from 2013 to 2023. Patients were included if they were ≥18 years old and underwent emergent nontraumatic laparotomy. Or primary outcome was mortality. Secondary outcomes included the usage of DCL, complications, intensive care unit admission, postoperative ventilation, and hospital length of stay.
Results
A total of 1249 patients were included with 745 (59.6%) direct admissions and 504 (40.4%) transfers. Transferred patients had higher PESAS scores (5 vs 3, P < 0.0001) and ASA classifications (ASA 4: 31% vs 22%, P = 0.0004). They also had higher rates of DCL (52% vs 42%, P = 0.0008), ICU admissions (52% vs 40%, P < 0.0001), and increased ventilation in transfers (47% vs 37%, P = 0.0004). While overall complications were higher in transferred patients (50% vs 39%, P = 0.0002), mortality rates were not significantly different (18% vs 14%, P = 0.1479).
Conclusions
Transferred EGS patients presented with greater preoperative severity and required DCL at higher rates. Transferred patients had increased complications, ICU, and ventilation needs. They also had an increase in complications however no difference in mortality. This suggests that while transferred patients are at increased preoperative acuity effective transfer systems and utilization of DCL may mitigate mortality risk in these patients.
Introduction
Emergency general surgery (EGS) encompasses a patient population with high-acuity pathologic conditions arising from a wide range of etiologies. Compared to patients undergoing elective procedures, those requiring EGS experience significantly higher morbidity and mortality.1,2 With at least 11% of all surgical patients requiring emergent operations, EGS represents a substantial portion of the surgical population.3-5 Similar to trauma patients, damage control laparotomy (DCL) has become a widely utilized strategy in EGS, allowing for rapid surgical intervention followed by expedited transfer to the intensive care unit for resuscitation before definitive treatment.6,7
A range of factors influence the outcomes of patients undergoing EGS.8-11 Among these, patient transfer has been associated with worse surgical outcomes, particularly increased mortality.12-14 Given that a significant portion of the U.S. population resides in rural areas, understanding the impact of patient transfer is of particular importance. While rural regions often have critical access hospitals, they frequently lack surgeons with regular EGS experience, surgical ICUs, and other specialty care services.15-19 The primary reasons for transfer include the need for specialty care or access to an available surgeon. 20 Of patients that require EGS up to 20% will need a transfer to higher level of care.14,21
This study aims to evaluate the impact of patient transfers on mortality rates and the utilization of damage control laparotomy in EGS patients. Based on prior literature, we hypothesize that transferred patients will demonstrate increased mortality and higher rates of damage control laparotomy compared to those who present as direct admissions.
Methods
Patient Population
This retrospective cohort study included all patients who underwent emergent exploratory laparotomy under the Acute Care Surgery service at our academic institution from 2013 to 2023. Patients were identified using the Current Procedural Terminology (CPT) code 49 000. Patients were included if they were 18 years old or older and underwent an emergent exploratory laparotomy. Patients were excluded if they were age under 18 years, received laparotomy for traumatic indication or underwent initial operative intervention at another facility. This project received approval from our institutional review board (IRB: STUDY00001882).
Data Collection
Data was collected through manual chart reviews of the electronic medical record (EMR) system and stored in REDCap. 22 Patient demographics included age, race, and gender. Preoperative variables collected for analysis included ASA (American Society of Anesthesiologists) classification, Charlson comorbidity index (CCI), and physiological emergency surgery acuity score (PESAS). Patient transfer information included if they initially presented to our facility or an outside facility, the initial time our facility was contacted for transfer and time of arrival out our institution.
Operative variables included whether fascial closure was achieved with a definitive laparotomy (DEF) as compared to damage control laparotomy (DCL) with temporary abdominal closure. Intensive care unit (ICU) data collected included the prevalence and duration of ICU admission as well as the prevalence and duration of postoperative treatment with ventilation. The primary study outcome was all-cause mortality. Secondary study outcomes included prevalence of DCL, postoperative complications, and hospital length of stay (LOS). Specific complications considered in analysis included atrial fibrillation, NSTEMI/MI, cardiac arrest, anemia requiring transfusions, postoperative pneumonia, pulmonary embolism, acute kidney injury, surgical site infection, multi system organ failure, urinary tract infection, delirium, anastomotic leak, or urinary retention.
Statistical Analysis
For statistical analysis, all patients were divided into either those who were transferred or patients who directly presented to our facility (direct admission). All continuous variables were checked for normal distribution using D’Agostino & Pearson test. Continuous variables were analyzed as mean or median with either ANOVA or Kruskal-Wallis tests being performed, depending on the normality of the data. All categorical data was analyzed using Fisher exact test and represented as n (% of total).
Results
Demographics
Demographic Information
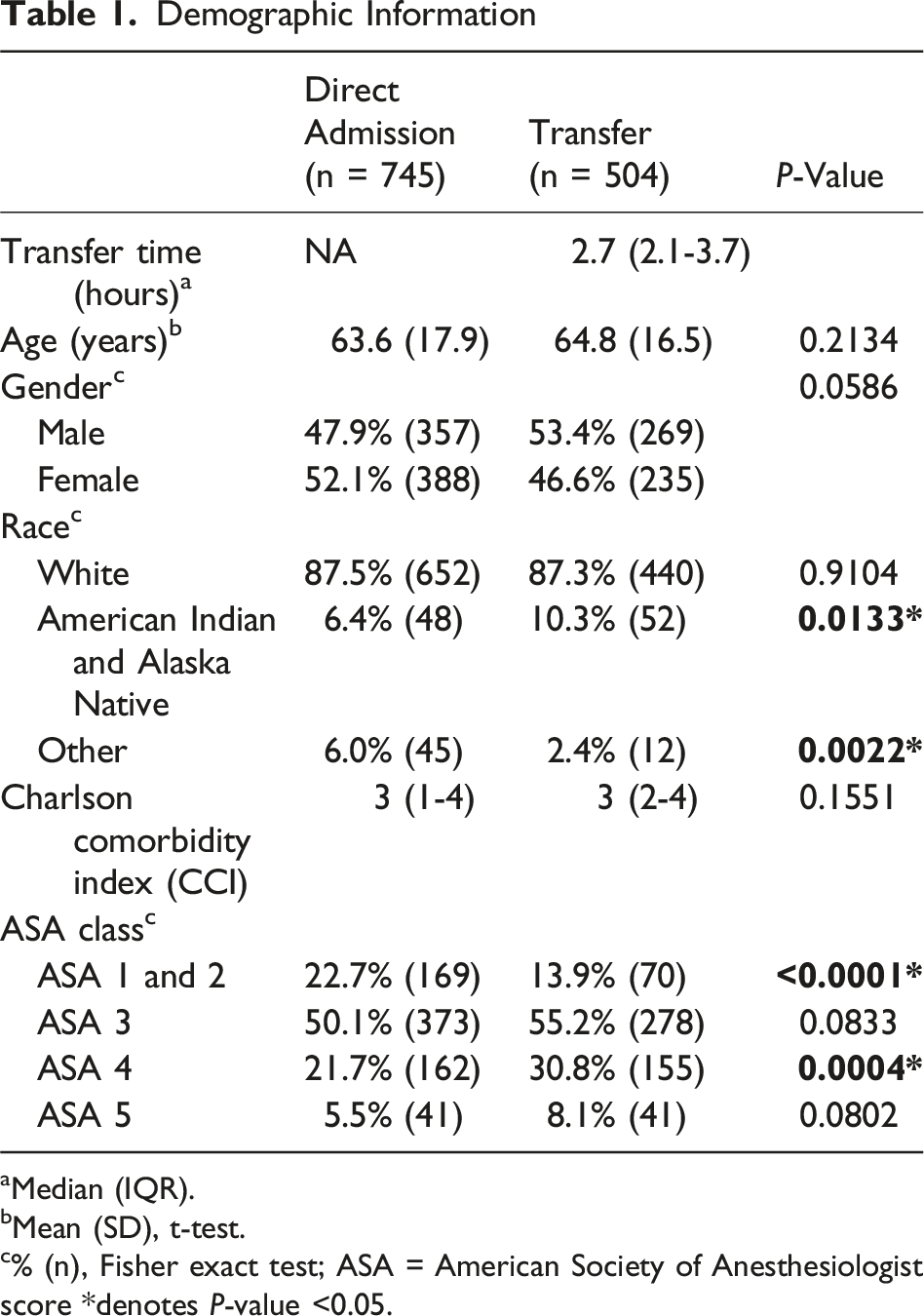
aMedian (IQR).
bMean (SD), t-test.
c% (n), Fisher exact test; ASA = American Society of Anesthesiologist score *denotes P-value <0.05.
Operative Characteristics
Operative Features and Outcomes
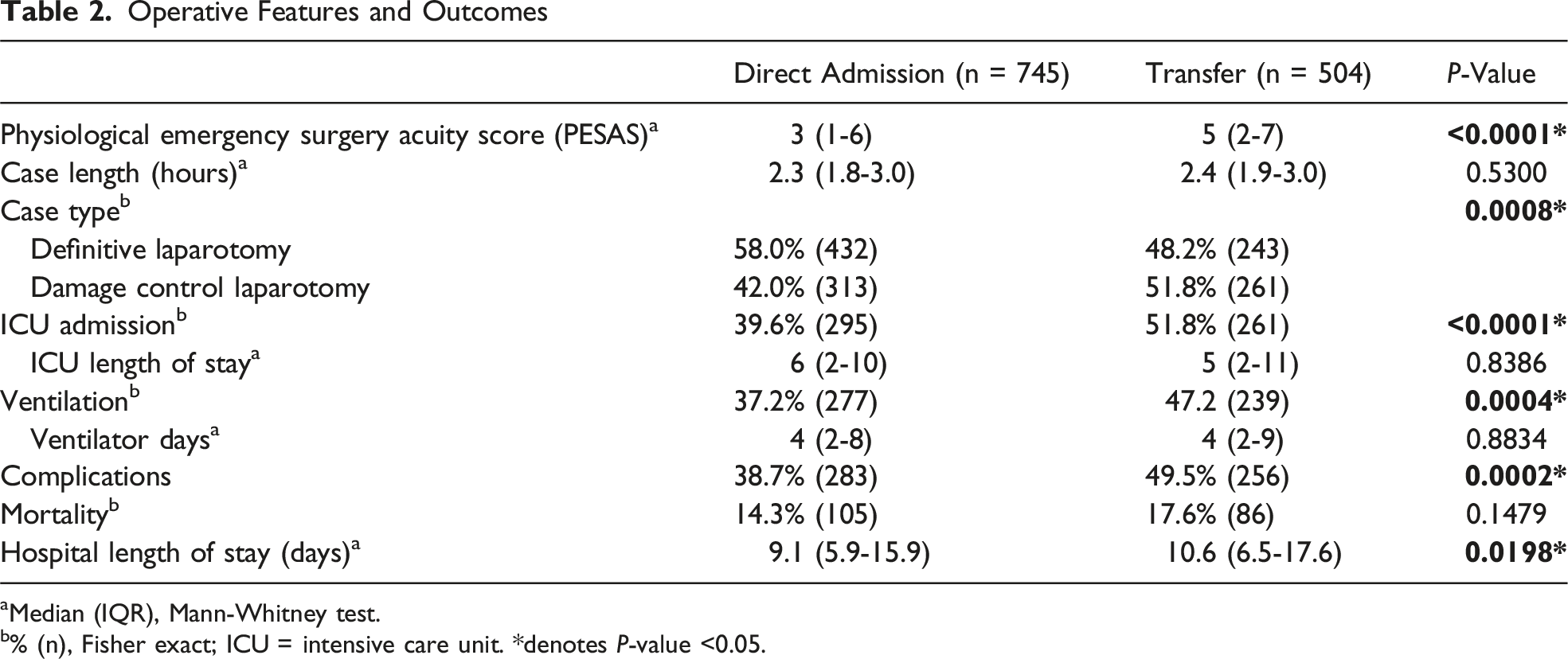
aMedian (IQR), Mann-Whitney test.
b% (n), Fisher exact; ICU = intensive care unit. *denotes P-value <0.05.
Our primary outcome of mortality was similar between groups with patients who were transferred having a mortality of 18% (n = 86) and direct admission mortality being 14% (n = 105). ICU admission was higher in transfer group at 52% (n = 261) compared to direct admission at 37% (n = 295, P < 0.0001). Similarly, the need for postoperative ventilation was more frequent in transfers at 47% (n = 239) compared to 37% (n = 277) in direct admission (P = 0.0004). Of the patients that were admitted to the ICU and those that required mechanical ventilation saw no difference in ICU length of stay of ventilation days between groups. In regard to complication rates, we did find a higher percentage in transferred compared to direct admissions 50% (n = 256) vs 39% (n = 283) vs 50% (256) respectively (P = 0.0002). We also saw a slightly longer hospital length of stay in transferred patient with a median of 11 days compared to direct admission with a median of 9 days (P = 0.0198) (Table 2).
Discussion
With prior studies showing worse outcomes for emergency general surgery (EGS) patients undergoing interfacility transfers, we aimed to evaluate this within our patient population.11,13,20 Given the existing literature, we hypothesized that transferred patients would have higher mortality rates and require more damage control laparotomies (DCL). While we did observe higher rates of DCL among transferred patients, interestingly, mortality was similar between the groups. This was despite higher proportions of ASA classes 3, 4, and 5 patients in the transfer group, as well as higher PESAS scores. So, while our data did indicate that transferred patients had an increase in preoperative risk factors and they also required DCL at a higher rate, they did not experience mortality at a higher rate.
We reported mortality rates of 14.3% for directly admitted patients and 17.6% for transferred patients, and for reference, a 2015 study which drew from National Surgery Quality Improvement Project (NSQIP) showed an EGS mortality rate of 12.5%. 1 While our reported mortality rates are slightly higher than some reported literature, this is likely secondary to our inclusion criteria of patients needing to both have an emergent operation and the index operation to be a laparotomy in contrast to including all EGS operations.1,2
Other studies report a wide range of transfer rates among patients, with some studies showing up to 30%.12,14,21 In contrast, our study found that 40% of our EGS patients were transfers, which may explain differences in our findings compared to other centers. Our transferred patients also had a relatively short transfer time of 2.7 hours from initial contact by transferring institution to arrival at our institution. This is not unexpected given our facilities located within North Dakota which has 37 critical access hospitals with limited surgical capability. 23 The findings from this work, then, are most generalizable to facilities where transferred patients represent a larger part of the overall case mix. Interfacility patient transfer occurs in around 2% of EGS patients and is not strongly influenced by patient factors but does correlate strongly with hospital size and rurality. 24 The ability of tertiary hospitals to care for transferred patients is related to the strength of the local transfer network. As well accepted that delay in surgical care for acuity ill patients can independently increase mortality and complications; thus, an intact efficient transfer network that expedites transfer and inherently time to operative time can aid in improving surgical outcomes for patients.
A study by Allen et al. of EGS transfers within Canada. 13 They found that transfer patient had higher operative acuity, number of comorbidities, and need of a second operation. 13 They also found that transfer status was independent predictor of complication status and need for ICU admission but not mortality. 13 We did find increased ICU admission and increased of postoperative ventilation within our transferred patients. However, this is less likely due to the transfer status and more likely secondary to the acute illness of the patient as echoed by the increased ASA class, PESAS, and utilization of DCL. Similarly, we found a rate of complications about 11% higher in transferred patients vs those directly admitted, and this aligns with existing literature. 24
Evaluation of transfer outcomes is of particular importance in settings with a high transfer ratio. A recent study showed that operative delay after presentation increased morbidity and mortality. 25 This has also been echoed in other studies showing that increase in operative intervention negatively impacts patient outcomes.26,27 The need and ability of facilities to arrange effective transfers can independently increase the time from presentation to operation significantly. This is notable in a healthcare system that is often at max capacity.
Limitations
As our study is retrospective, it is limited by inherent bias within the study design including accuracy of information within the charts. Our center also receives a high amount of transfer patients and this limits the study’s external validity to center who have a low percentage of transfers. We did not report nonoperative transfers attempted transfers as our outcomes were focused on surgical outcomes. Finally, our study did not evaluate the reason of transfers for patients which would further shed light on limitations of facilities in more rural settings.
Conclusions
In our study, patients who presented as transfers comprised a significant portion of the emergency general surgery population. These patients were more acutely ill, with higher ASA classifications and PESAS scores compared to those admitted directly. Transfers also required damage control laparotomies at higher rates. Additionally, they experienced higher complication rates, increased ICU admissions, greater need for postoperative ventilation, and longer hospital stays. However, mortality rates were similar between transfer and direct admission patients. This is likely secondary to expeditious transfer times and a well-established transfer network within our service area.
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.