
Abstract
Background
Social determinants of health are associated with differences in care and outcomes for pancreatic ductal adenocarcinoma (PDAC) patients. This study evaluates the impact of race and socioeconomic status (SES) on the presentation, management, and survival of patients with potentially resectable PDAC within a metropolitan hospital system in the Southeast United States.
Methods
A retrospective analysis of PDAC patients (2014-2020) across a multi-hospital system was performed. Associations between race as well as socioeconomic and clinicopathologic data with presentation, treatment, and survival were analyzed.
Results
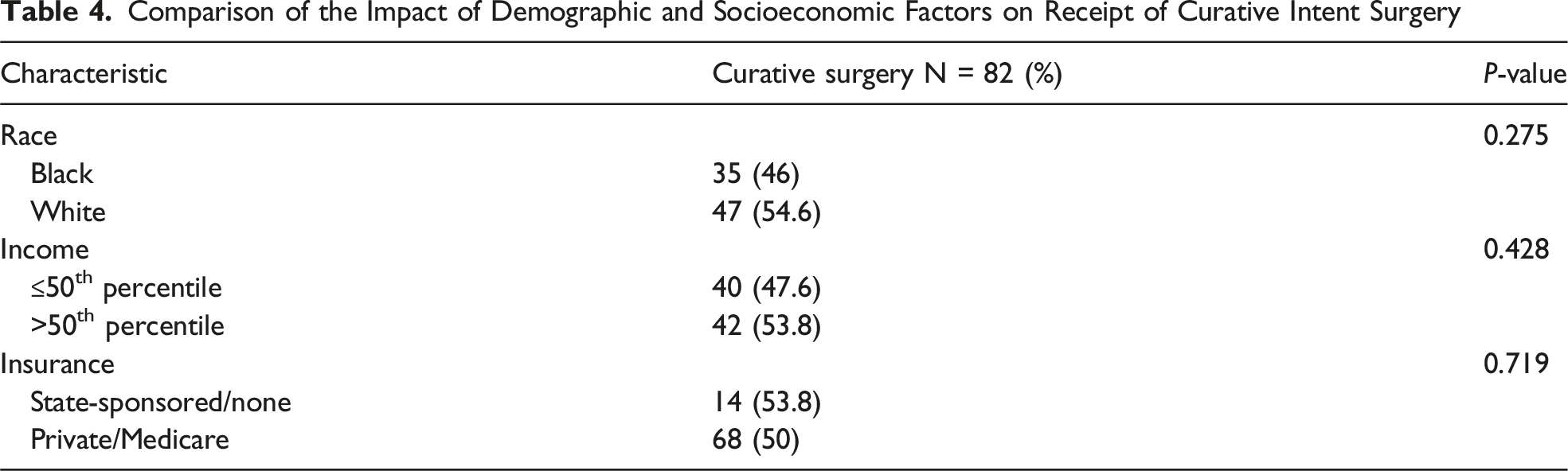
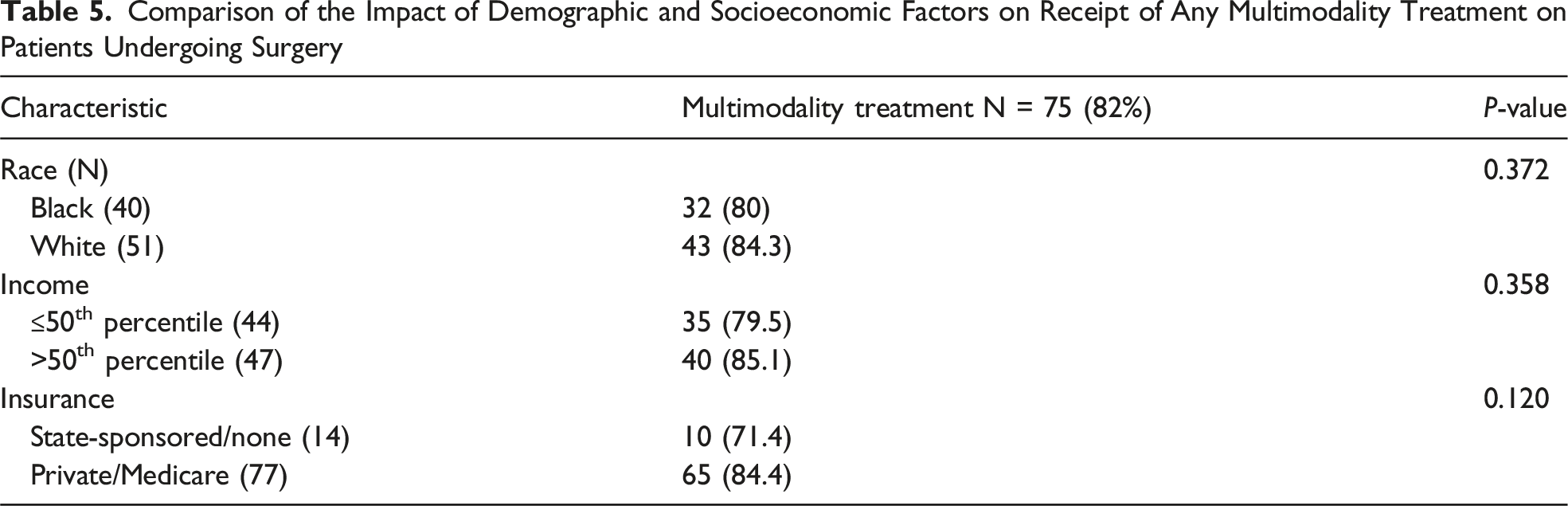
Among 222 patients, 104 (46.9%) were Black and 118 (53.1%) were White. Black patients presented at a significantly younger age (61 vs 66, P = 0.007) and resided within the lowest 2 quintiles for median income (68.2% vs 42.4%, P < 0.0001). Compared with White patients, Black patients were more likely to have Medicaid/no insurance (22.1% vs 11.9%, P = 0.040). Receipt of multimodal therapy and curative intent resection was not significantly different between Black and White patients (80% vs 84.3%, P = 0.372; 46% vs 54.6%, P = 0.275), ≤50th percentile vs > 50th percentile income (79.5% vs 85.1%, P = 0.358; 47.6% vs 53.8%, P = 0.428), or Medicare/private vs Medicaid/no insurance (84.4% vs 71.4% P = 0.120; 50% vs 53.8%, P = 0.719). On survival analysis, outcomes were determined by receipt of multimodal treatment and histopathological factors but did not differ based on race or SES.
Discussion
This analysis demonstrates that patients with PDAC can receive similar treatment despite differences in race and SES. Interestingly, Black patients presented at a significantly younger age, warranting further evaluation of risk factors and tumor biology.
Key Takeaways
• Treatment of patients with pancreatic ductal adenocarcinoma can be equivalent despite differences in race and socioeconomic status • Black patients present at a significantly younger age which could be due to race specific risk factors and/or tumor biology • Future investigation of the impact of social determinants of health on the outcomes of cancer patients should be performed at the local level to gain actionable insights into these patterns
Introduction
Although there is a rising incidence of pancreatic ductal adenocarcinoma (PDAC), survival rates remain poor. As seen in other malignancies, there is population-based data demonstrating an association between social determinants of health and differences in the presentation of PDAC patients and inequalities in the delivery of optimal cancer therapy. At a national level, Black patients are reported to have a 40%-90% higher incidence of being diagnosed with PDAC, often at a younger age and with more advanced disease when compared to other racial groups.1-3 Studies using large administrative databases have shown lower rates of multimodal therapy and curative intent surgery among Black patients, those without insurance, and patients considered to have lower socioeconomic status (SES).1-7
While these studies demonstrate overarching trends in PDAC disparities at a national level, the observed outcomes stem from multiple factors and are expected to differ among institutions, communities, and regions. Without investigation at a more granular, local level, these disparities cannot be fully understood or effectively addressed. The current study examines the presentation, management, and survival of patients with potentially resectable PDAC in a hospital system that services a community with a large, socioeconomically disparate, Black population in the Southeast United States. We hypothesized that Black patients would present with more advanced disease, be less likely to receive optimal oncologic management, and have inferior outcomes compared to White patients. This evaluation was intended to identify differences in disease presentation and delivery of therapy to better understand how potential disparities might be addressed at the local level.
Methods
A retrospective analysis of patients diagnosed with PDAC from 2014-2020 across a multi-hospital system affiliated with the University of Tennessee Heath Science Center (UTHSC) in Memphis, TN, was performed. Institutional Review Board review at UTHSC was performed and approval was granted. Cases were identified based on an institutional tumor registry utilizing ICD-10 codes for PDAC. Patients were excluded if race was other than Black or White (these patients made up a small portion of the database: 1.2% Hispanic). The patient cohort was divided into 2 racial groups: Black and White. Patient demographics including age, gender, race, income status (based on median income by zip code), insurance status, and Charlson comorbidity index (CCI) were collected. Patients were stratified into income quintiles based on reported state percentiles from the 2022 United States Census Bureau 8 with the fifth quintile indicating the highest median income. Clinical, operative, and pathologic features were captured including tumor location, resectability status at presentation, type of resection performed, pathologic stage based on the American Joint Committee on Cancer (AJCC) eighth edition schema, and histologic features including lymphovasular invasion (LVI), perineural invasion (PNI), tumor grade, and resection margin. Patients were deemed resectable, borderline resectable, or locally advanced based on anatomic criteria as defined by the National Comprehensive Cancer Network. 9 Patients were also classified as borderline resectable based on poor performance status at the time of diagnosis. Disease specific survival (DSS) was calculated in months and analyzed.
Descriptive statistics (reported as medians with interquartile range) were used to characterize the patient population where applicable. χ2 analysis was performed for categorical variables while continuous variables were analyzed using Student’s t-test or the Wilcoxon rank sum test where appropriate. Primary outcomes were evaluated using survival analysis. Patients without the primary outcome of death or loss to follow‐up were considered censored. Kaplan-Meier curves and median survival were calculated for both groups and compared in a univariable manner using the log‐rank test. Variables exhibiting significance less than 0.2 were considered for inclusion in the full multiple regression model. Multivariable regression analysis was performed to determine significant predictors for DSS using a Cox‐Proportional Hazards model. All clinically relevant interaction terms were examined. Statistical significance was set at P < 0.05 and derived from two-tailed tests. The 95% confidence intervals were provided where applicable. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Comparison of Demographics and Presenting Characteristics Between African American and White Patients With Pancreatic Cancer (N = 222)
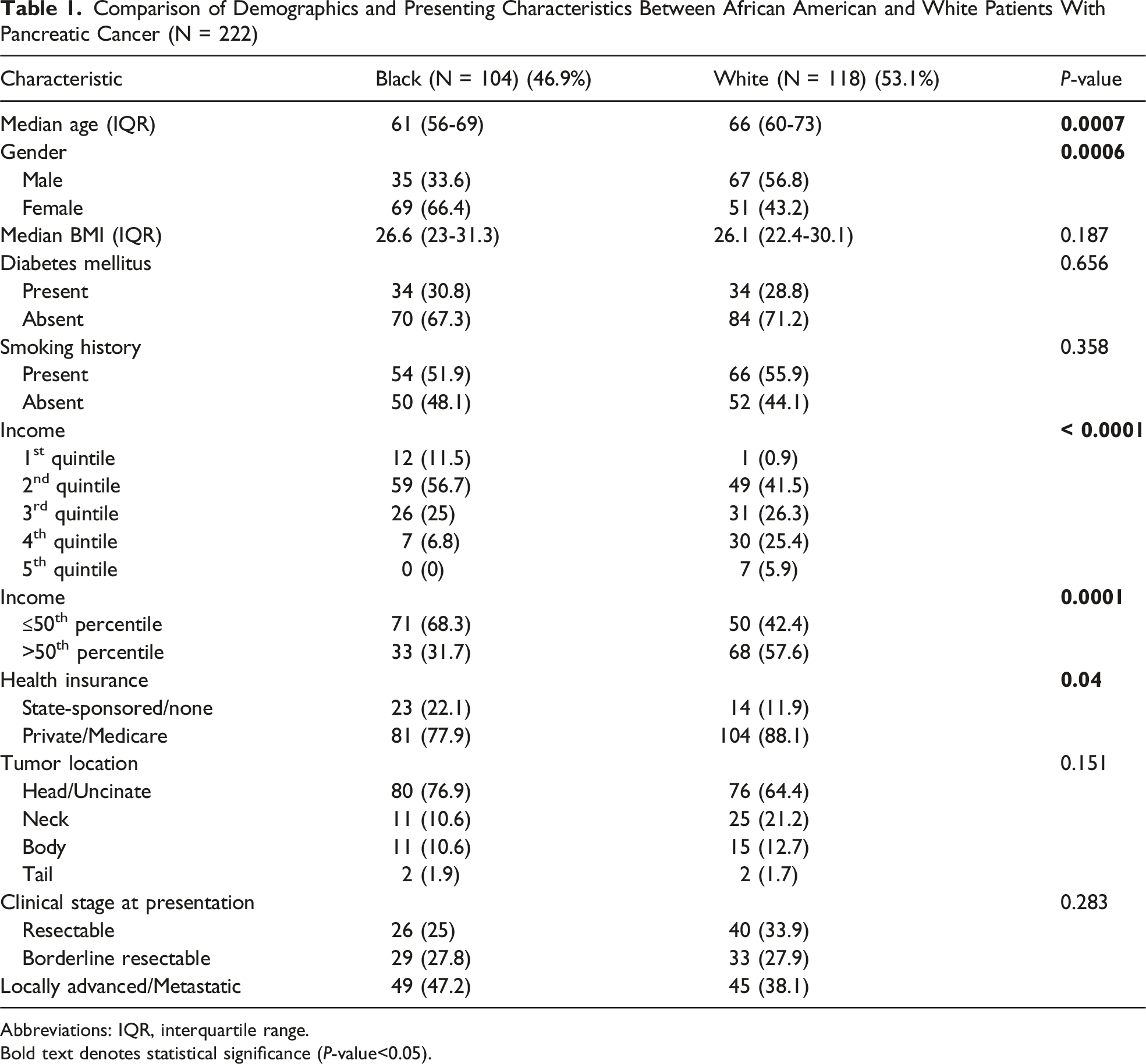
Abbreviations: IQR, interquartile range.
Bold text denotes statistical significance (P-value<0.05).
Comparison of Demographics and Presenting Characteristics Between African American and White Patients With Potentially Resectable Pancreatic Cancer Undergoing Surgery (N = 91)
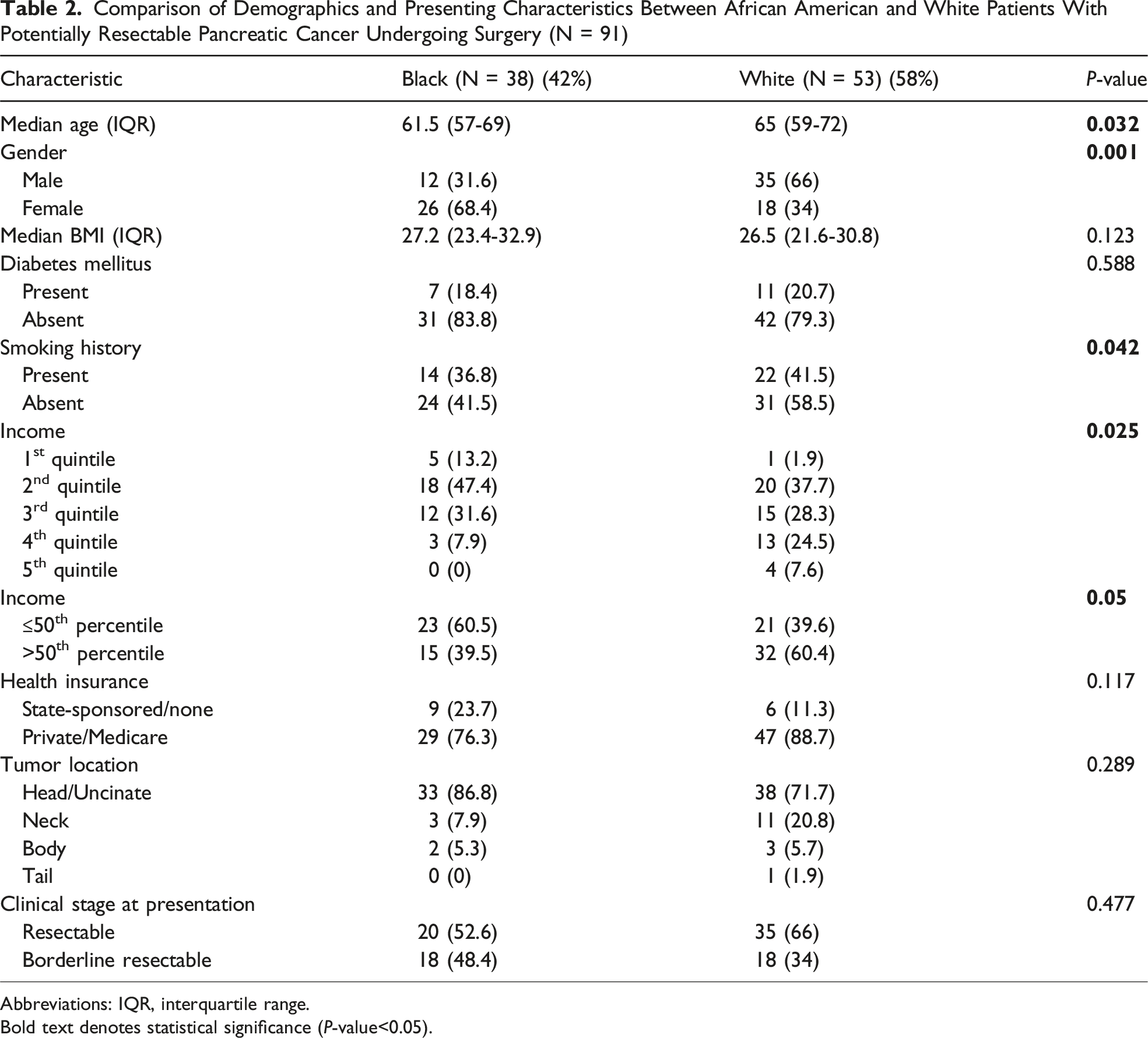
Abbreviations: IQR, interquartile range.
Bold text denotes statistical significance (P-value<0.05).
Comparison of Treatment and Clinicopathologic Characteristics Between Black and White Patients Completing Curative Intent Surgery (N = 82)
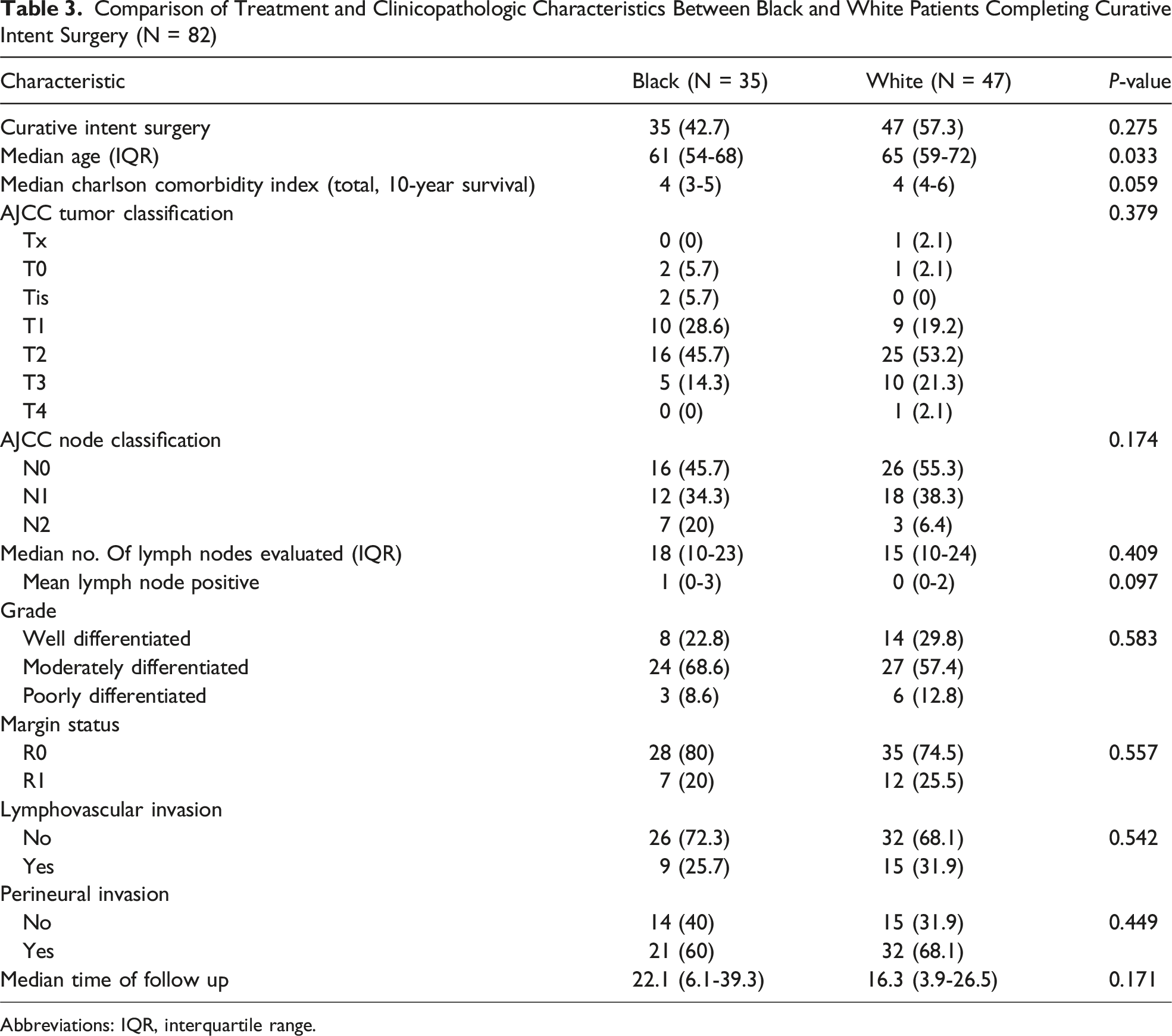
Abbreviations: IQR, interquartile range.
Comparison of the Impact of Demographic and Socioeconomic Factors on Receipt of Curative Intent Surgery
Comparison of the Impact of Demographic and Socioeconomic Factors on Receipt of Any Multimodality Treatment on Patients Undergoing Surgery
Comparison of the Impact of Demographic and Socioeconomic Factors on Patients Undergoing Upfront Resection Receiving Adjuvant Treatment
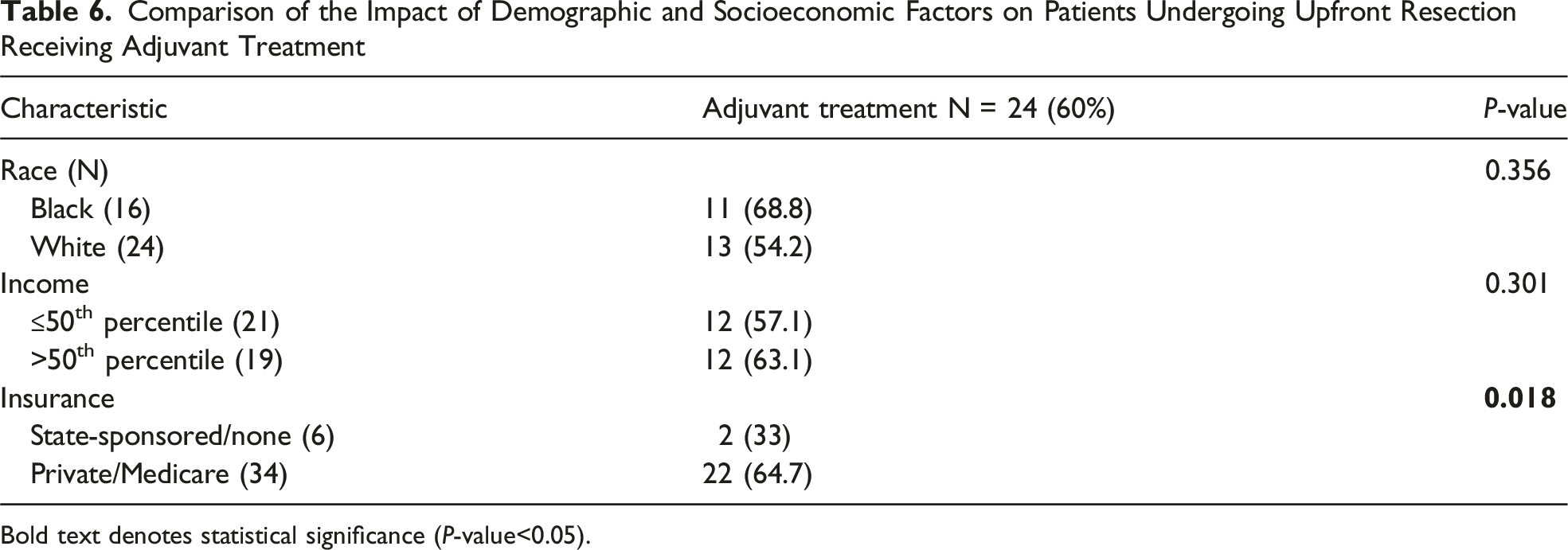
Bold text denotes statistical significance (P-value<0.05).
Univariable Analysis of Predictors of Disease Specific Survival for Patients Undergoing Curative Intent Surgery
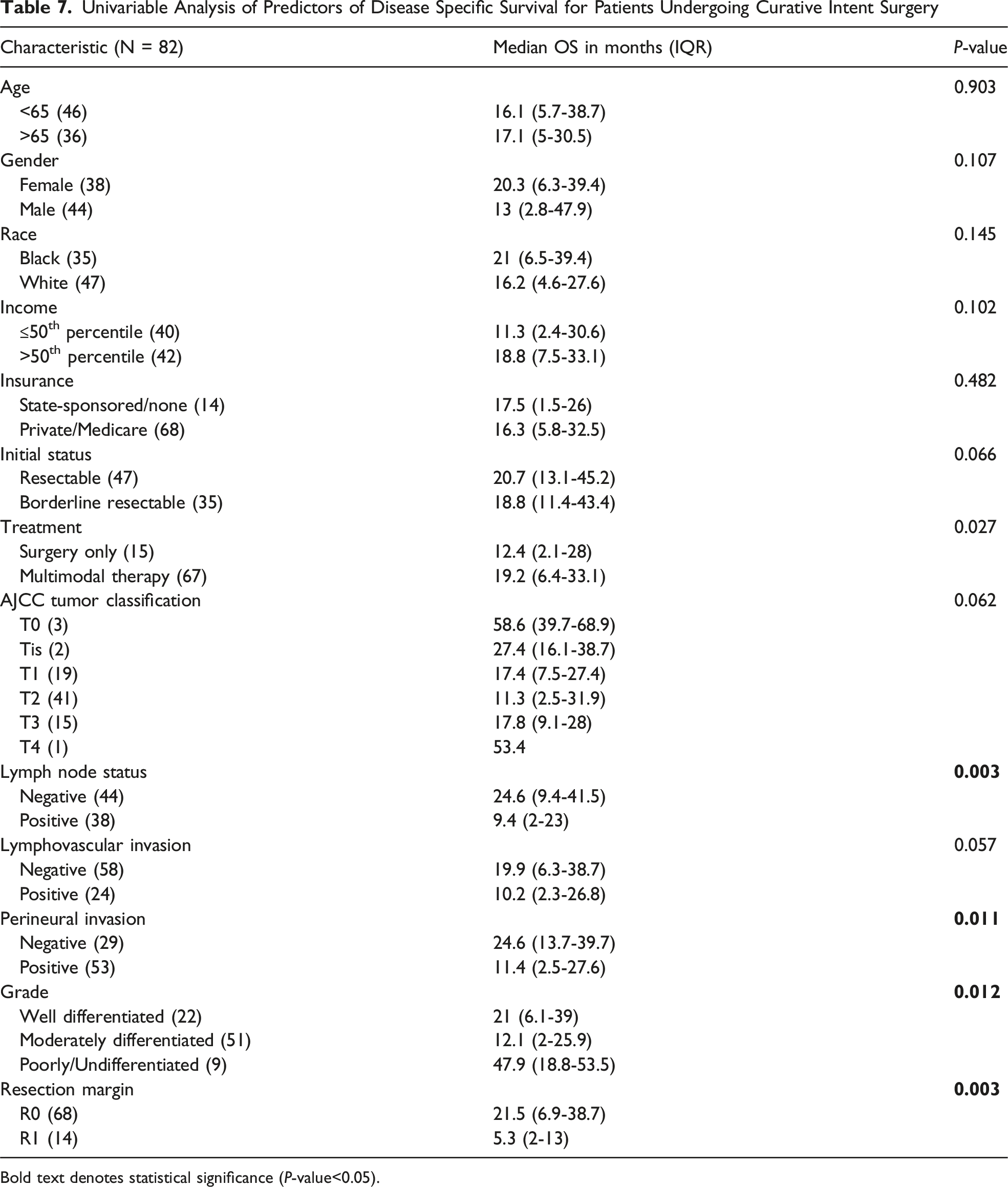
Bold text denotes statistical significance (P-value<0.05).
Multivariable Analysis of Predictors of Disease-specific Survival for Patients Who Completed Curative Intent Surgery
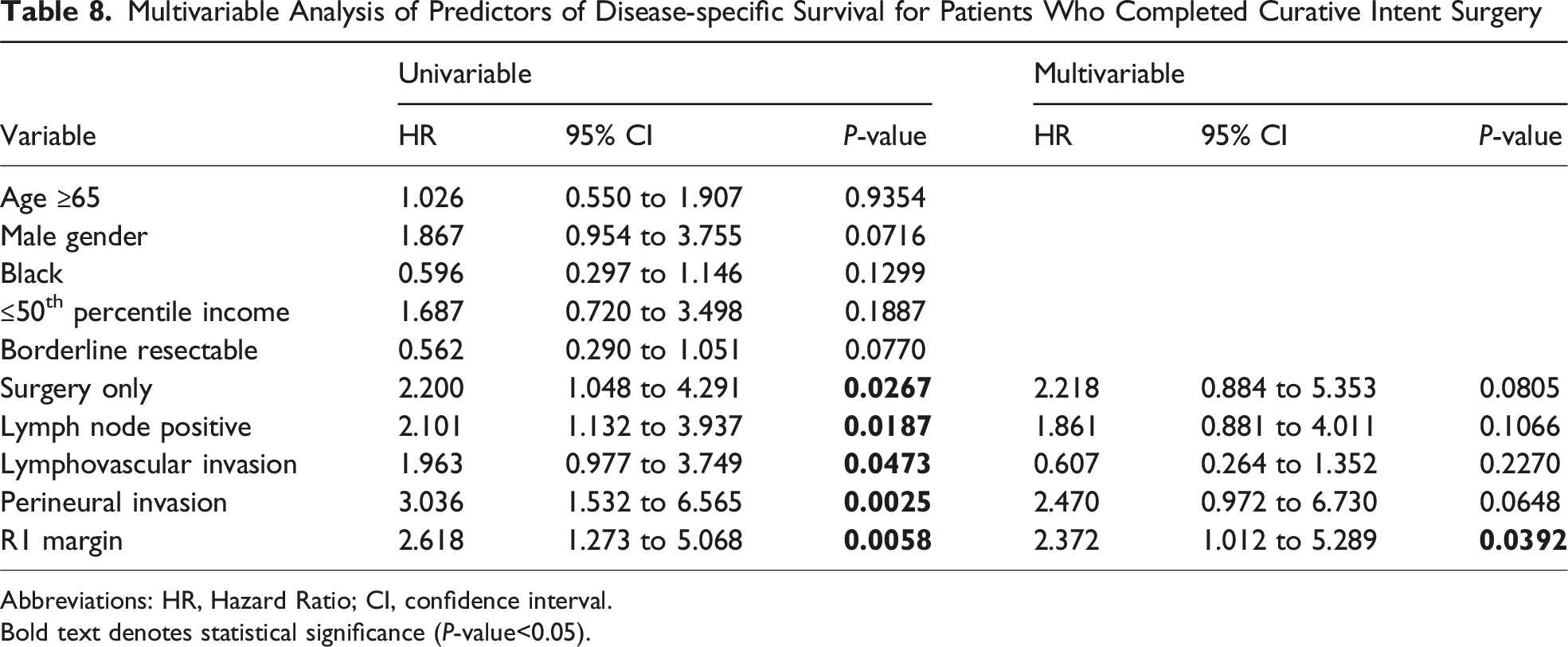
Abbreviations: HR, Hazard Ratio; CI, confidence interval.
Bold text denotes statistical significance (P-value<0.05).
Discussion
The current study evaluates the presentation, treatment, and DSS of PDAC patients within a hospital system in Memphis, TN, that services a predominantly Black population with socioeconomic disparities. The analysis found that Black patients were more likely to present at younger age but had similar clinical stage at presentation and histopathological features compared to White patients. Importantly, despite socioeconomic disparities between Black and White patients in this study, there was no significant difference in the completion of curative intent surgery, receipt of multimodal therapy, or DSS.
Previous studies have reported a higher incidence of PDAC among Black patients compared to other racial groups.3,5,10,11 However, the demographic pattern within these studies mirrors that of the national population with Black patients representing a minority (<15%). In contrast, Black patients account for 65% of the population in Memphis, TN. 8 The distribution of cases in this analysis suggests that within this community the incidence of PDAC cases is not higher among Black patients. Notably, the median age at diagnosis among Black patients was 61, which is significantly lower than White patients within the community and much lower than the national average of 70. 12 Although prior studies have also identified a younger age at diagnosis among Black patients with PDAC, 13 the median age of 61 in the current study is much lower than Black patients within national cohorts. When examining known modifiable risk factors for PDAC such as smoking, obesity, and diabetes as potential explanations for this age discrepancy, we did not identify a difference between Black and White patients. However, the true impact of these risk factors accounting for racial disparities in PDAC is unclear. 14 Moreover, these observed differences are likely related to the interaction between known risk factors as well as diet, 15 genetics, 16 and the intestinal/pancreatic microbiome.17,18 Ultimately, understanding differences in the incidence and age at diagnosis between racial and socioeconomic groups will require deeper translational investigation.
Although survival rates remain low for all stages of PDAC, resection offers the only opportunity for cure and can significantly prolong life in appropriately selected patients. Several studies have demonstrated that curative intent resection is performed less often in Black compared to White patients.11,19-23 Some of these studies have reported that Black patients were less likely to be offered resection,6,20,24 while others demonstrated equal rates of being offered resection between racial groups with Black patients less likely to undergo pancreatectomy.11,21 In addition to Black race, lower rates of resection have been reported among patients with lower SES assessed by insurance, income, and education.3,5,25
While resection is critical to potential cure and improving outcomes, multimodal therapy undoubtedly enhances these goals for patients with PDAC. Specifically, systemic chemotherapy is known to increase overall survival.1,26-28 Unfortunately, similar to lower rates of resection, Black patients and those with lower SES have repeatedly been found less likely to receive multimodal care.1,6,13,18,26,27,29 A study using the Surveillance, Epidemiology, and End Results Registry and Medicare databases reported that Black patients were significantly less likely to have consultations with cancer specialists including medical oncology, radiation oncology, and surgery. 22 Black patients in that study were more likely to reside in lower income areas. 22 On multivariable analysis of patients with locoregional disease, even after seeing a specialist, Black patients remained significantly less likely to receive chemotherapy and resection compared to White patients. 22 A similar study using a Florida cancer registry and inpatient hospital data found that patients of low SES were less likely to receive surgery, chemotherapy, or radiation and had significantly higher morbidity and mortality rates. 29 Factors such as inability to pay or having non-private insurance, lack of transportation, and limited social support are inherent obstacles to access and delivery of cancer directed therapy.
Given the above findings from national studies, we were encouraged by the results of the current analysis, as this work was initiated to identify potential gaps in care within the system and community that could be targeted for improvement. There are several factors that influenced the observed findings. First, many patients likely entered the system via emergency department admissions with provisions made by the hospital system and affiliated providers to deliver subsequent care regardless of insurance status. Second, although the patient cohort is from a community hospital system, it is affiliated with an academic medical center, and the surgeons involved in this study are academic surgical oncologists with expertise in pancreatic cancer care. Third, over the last decade, there has been an increased effort to review patients who are potential surgical candidates in a non-hospital based, community-wide, multidisciplinary hepato-pancreato-biliary tumor board led by academic surgeons with participation from both academic and non-academic medical oncology, radiation oncology, genetics, gastroenterology, radiology, and advanced-practice providers. This community-inclusive approach has greatly facilitated treatment planning and coordination of care between physicians working in different specialty groups. Finally, there are multiple sites for chemotherapy infusion and radiation therapy within the community, which may have limited the need to travel distances that might otherwise preclude these treatments in patients with low SES. While these factors likely helped achieve similar care between the 2 groups in this analysis, it is appreciated that this does not apply to every community or health care system.
That equivalent care and outcomes can be delivered to Black and socioeconomically disparate populations with PDAC has been demonstrated previously. A National Cancer Database analysis by Dhar et al 30 found that patients treated in “safety net hospitals,” defined as those having the highest quartile of Medicaid and uninsured patients, achieved similar rates of resection, chemotherapy, chemoradiation, and overall survival. However, the authors of that study highlight the potential negative impact of federal programs, such as the Hospital Readmissions Reduction Program and Hospital Acquired Condition Reduction Program, resulting in financial penalties for these safety net hospitals. While these policies seem well intended, safety net hospitals are inherently at higher risk of patients having longer hospital stays and unplanned readmissions given the patient populations they serve. It would seem appropriate that in the future policymakers consider metrics such as providing equal cancer care to disparate populations when designing federal reimbursement incentives for hospitals and health care systems.
Limitations of the current study include its retrospective nature and relatively small sample size. The patients studied were identified through the tumor registry of 1 of 4 major hospital systems in the community; therefore, it is possible that the findings might vary if patients from the other hospitals were included. However, the makeup of patients within the study likely reflects the overall population within the region secondary to location and referral patterns. Some patients were lost to follow-up following initial resection and thus were unable to contribute to survival data, leading to a possibility for loss to follow-up bias. In addition, the current study does not address other important factors that should be considered in PDAC patients, such as quality-of-life assessments and palliative care and hospice transitions when necessary. In future evaluations, it will be important to assess the impact of timing between diagnosis and specialty referral and initiation of treatment.
In conclusion, the current study demonstrates that equal care can be provided to Black and White patients with PDAC despite socioeconomic disparities. Notably, the median age at diagnosis among Black patients was much lower than the national average as well as Black cohorts in prior studies. Efforts into better understanding the potential interplay between race, modifiable habits, diet, and socioeconomic factors with molecular drivers of disease are needed to better understand this finding. While previous studies have relied on large national databases to analyze the effects of race and SES among PDAC patients, we encourage other groups to examine these factors within their own hospital system and community to identify ways to close local gaps in cancer care disparities.
Footnotes
Author Note
DP, SB, AF, EG, GA, PD: conceptualization, methodology, investigation, data curation, writing and editing of the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.