
Abstract

Opioids, while effective in the treatment of pain, have been the source of an overdose epidemic in the US for more than two decades. It is well accepted that, in addition to short-term side effects, prolonged opioid use can lead to tolerance and dependence, requiring escalating doses for the same clinical effects. 1 On the other hand, inadequately managed pain can increase the risk of progression to chronic pain disorders and thus impair physical function. 2 Effective pain management is particularly challenging in a surgical intensive care unit (SICU) due to the severity of injuries and postoperative pain. This study aims to collect more data on how opioid use prior to admission affects morphine milligram equivalents (MMEs) needed for pain control in ventilated and non-ventilated SICU patients.
This study analyzes opioid-prescribing trends among ventilated and non-ventilated patients with and without persistent opioid use before hospitalization in an academic American College of Surgeons Adult Level 1 Trauma Center. Our Institutional Review Board (IRB297326) deemed the study exempt. We used a previously created institutional interactive data collection and visualization software program to create a regularly updated MME aggregator using our hospital’s EMR. 3 Beginning in July 2021, this database prospectively captured daily MMEs, demographic data, and ventilator status for all patients admitted to the SICU.
Persistent opioid patients were defined as having an active outpatient order at the time of admission, while naïve opioid patients had no active outpatient order. Any patients with an admission day outside of the study period (July 2021-June 2024) were excluded. Patients on a continuous infusion of a neuromuscular blockade, those with a percutaneous left ventricular assist device or on Extracorporeal Membrane Oxygenation, and patients with an intracranial pressure monitor for a severe TBI were also excluded. Analysis of MME per patient day was performed based on prior opioid exposure and ventilation status for each day during their stay in the SICU: naïve ventilated, naïve non-ventilated, persistent ventilated, and persistent non-ventilated.
Demographics, including age, sex, race, and discharge disposition, were summarized for each ventilated status group. Within each status group, these factors were compared between naïve and persistent opioid users using Student’s T-tests and chi-square tests depending on the composition of the variable. Similarly, the average MME per patient day was compared between these groups. After reviewing the distribution of the demographics between the opioid usage groups, a multivariable model was built, looking at persistent opioid usage as the primary predictor of average MME per patient day while controlling for age, sex, and race. Age was treated as a continuous variable in all multivariate linear regression models. The negative coefficients for age in both the ventilated and non-ventilated MME models indicate that each additional year of age is associated with a reduction in daily opioid administration (MME/pt-day), independent of sex, race, and prior opioid use status. A model evaluating the effect of opioid usage on length of stay was also performed. Significant associations were reported if the P-value fell below an alpha level of 0.05. All analyses were completed in R version 4.4.1 (the Free Software Foundation).
The study included 2729 patients with 3385 admissions. 2.2% of ventilated and 3.4% of non-ventilated patients were opioid persistent. The median ages were similar across all groups. There was a similar percentage of male naïve and persistent ventilated patients (67.4% vs 61.3%; P = 0.603), but a higher proportion of men were in the non-ventilated group (62.8% vs 44.1%; P = 0.003). Similarly, there were more white patients with persistent opioid use in the non-ventilated group (P = 0.039) despite no differences by race in the ventilated group (P = 0.270).
Ventilated patients with persistent opioid use received 52% more MME/day than ventilated naïve patients (346.9 vs 228.0; P = 0.003). In the non-ventilated group, patients with persistent opioid use received 127% more MME/day than non-ventilated naïve patients (55.7 vs 24.5 MME; P < 0.001). Persistent opioid use was not associated with longer hospital stays among ventilated patients (11.52 vs 10.64 days; P = 0.627) but was associated with a longer length of stay among non-ventilated patients (12.11 vs 8.38 days; P < 0.001).
Multivariate Regression Analysis
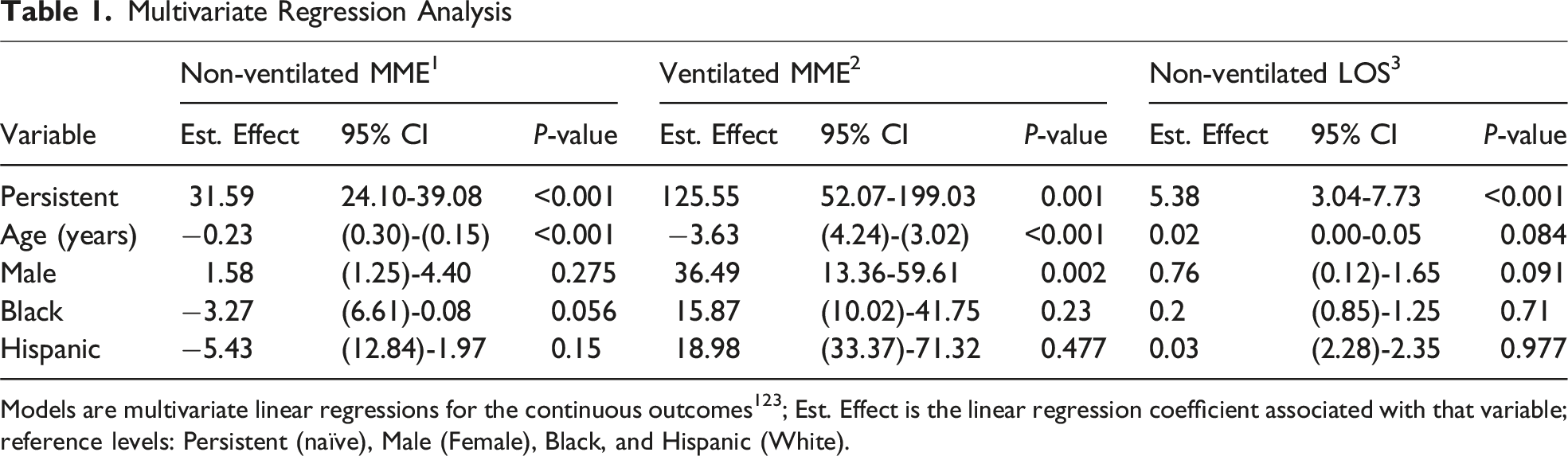
Models are multivariate linear regressions for the continuous outcomes123; Est. Effect is the linear regression coefficient associated with that variable; reference levels: Persistent (naïve), Male (Female), Black, and Hispanic (White).
Balancing effective pain management with opioids while minimizing their adverse effects remains challenging, particularly in the ICU, where patients frequently suffer from severe injury and postoperative pain. This study sought to determine opioid requirements for ventilated and non-ventilated patients depending on their opioid use before hospitalization. Persistent opioid use was associated with a higher MME/patient day in both ventilated and non-ventilated patients, as well as an increased hospital LOS in non-ventilated patients. These results remained while controlling for age, sex, and race.
This study was limited by our small sample population of persistent opioid users for both ventilated (2.2%) and non-ventilated (3.4%) patients. Additionally, there are many definitions of opioid persistence represented in the literature. 4 Our knowledge of a patient’s opioid status was limited to the presence of an active outpatient prescription at the time of their admission. Due to prescribing laws in many states, including ours, restricting opioid prescriptions to 7 days unless legal criteria are met, we can assume that those with active outpatient orders were most likely an exception to that 7-day criterion and were taking opioids chronically. Unfortunately, this did not allow us to consider illicit or unreported opioid use, or to definitively say that those patients with an active prescription were taking it. With our current software and electronic medical record, this was the most accurate data we had access to. Additionally, chronic use status is not always asked by clinical staff, and patients may respond inaccurately due to negative stigma regarding chronic opioid dependence. We are exploring opportunities to improve our data collection process on opioid use by integrating more detailed screening into our hospital EMR. We also had limited knowledge of the reason for the patient’s SICU admission, their comorbidities, prior surgeries, and the severity of injuries for trauma patients. These are potential confounding variables; however, attempting to group our already small cohort of patients by too specific criteria could dilute the results.
While patients with opioid use prior to admission typically have a higher tolerance and require higher doses for pain relief, there is limited data on how much more they may need. Our data showing an increase in administered opioids based on ventilation status and prior opioid use can help identify patients who may require higher doses. For example, a ventilated patient with prior opioid use could potentially need more than fourteen times the dose (346.9 vs 24.5 MME/pt-day) of a non-ventilated, naïve patient for adequate pain relief. The knowledge we gained from this study highlights the importance of continued research into personalized pain management.
Footnotes
Ethical Considerations
Our Institutional Review Board (IRB297326) deemed this study exempt on 5/30/2024.
Author Contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially supported by UAMS’s Translational Research Institute (TRI) grant UL1 TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kalkwarf is a state trauma center site surveyor and ATLS instructor. He is also a member of the Arkansas Preventable Mortality Committee Member and the former Medical Consultant for the Arkansas Trauma System. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Source data is available from authors upon reasonable request.