
Abstract
Background
Colorectal cancer is a common and deadly form of cancer. Sigmoid colon cancer is the most prevalent type of colon cancer. Robotic-assisted surgical systems, like the Senhance Digital Laparoscopy System, have attracted considerable attention in recent years. The purpose of this study was to confirm the non-inferiority of Senhance-assisted surgery regarding its short-term safety compared with conventional laparoscopic surgery for sigmoid colon cancer.
Methods
This retrospective single-center study analyzed data from patients undergoing a sigmoidectomy between March 2020 and 2025. Propensity score matching was employed to create comparable groups. Patient characteristics, short-term surgical outcomes, and pathological data were assessed. Postoperative complications were graded using the Clavien-Dindo system.
Results
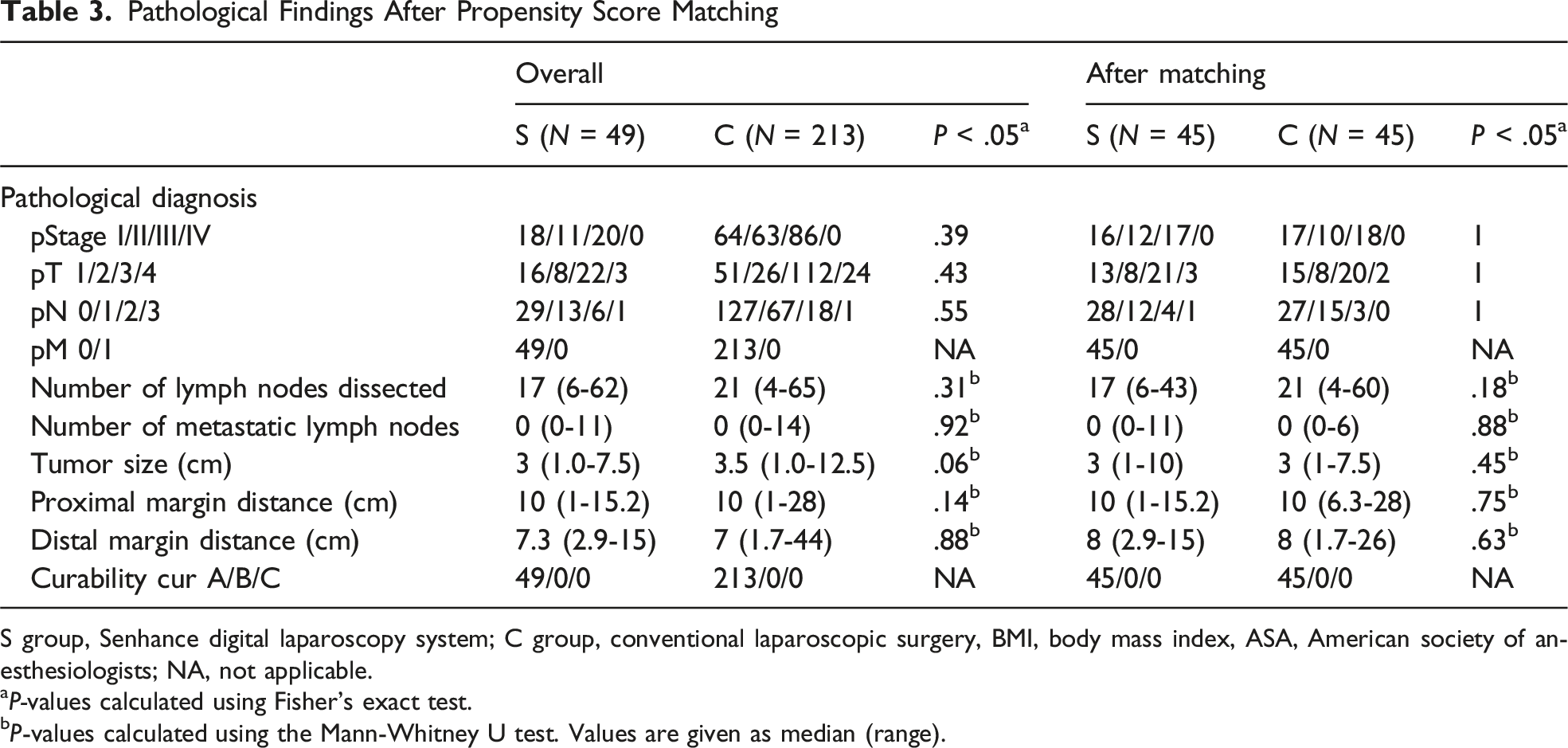
Prior to propensity score matching, there were differences in cancer stage between groups. After matching, two groups comprising 45 patients each were comparable across various factors. The operative time was significantly longer in the Senhance-assisted group compared with the conventional laparoscopic surgery group (236 min vs 204 min, P = .001), underscoring the importance of optimizing surgical techniques. Postoperative Numerical Rating Scale pain scores were significantly lower in the Senhance-assisted group on day 1 (3 [1-5] vs 4 [2-6], P = .03) and day 3 (2 [0-4] vs 3 [2-5], P = .02). However, no there were no significant differences in blood loss, complications, or pathological characteristics between the groups.
Conclusions
This study demonstrated that Senhance-assisted sigmoidectomy was non-inferior to conventional laparoscopic surgery in terms of short-term safety outcomes.
Keywords
Key Takeaways
This single-center retrospective study examined the safety of Senhance-assisted surgery compared with conventional laparoscopic surgery for sigmoid colon cancer. Postoperative Numerical Rating Scale pain scores were significantly lower in the Senhance-assisted group compared with the conventional laparoscopic surgery group. However, there were no significant differences in postoperative complications between groups. Robotic-assisted sigmoidectomy using Senhance is non-inferior to conventional laparoscopic surgery regarding short-term safety outcomes.
Introduction
Colorectal cancer (CRC) is the third most common cancer and the second most common cause of cancer mortality worldwide. 1 Sigmoid colon cancer is the most common type of colon cancer. 2 The safety and efficacy of laparoscopic surgery for CRC have been reported in RCTs, and laparoscopic surgery has become widespread.3-9 The Japan Clinical Oncology Group (JCOG) 0404 study reported that laparoscopic surgery was not non-inferior to open surgery regarding overall survival in patients with stage II or III colon cancer.10,11 The subgroup analysis of JCOG0404 revealed that some institutional variations in safety and efficacy occurred in laparoscopic surgery, highlighting the need for a qualification system, including training and education, when new surgical techniques are introduced in clinical practice. 12
Recently, attention has been focused on introducing and developing surgical robots.13,14 The Senhance Digital Laparoscopy System (Asensus Surgical Inc, Morrisville, NC, USA) is a surgical robot developed following the da Vinci surgical system. Senhance is an extension of laparoscopic surgery wherein the forceps used are the same as those used for laparoscopy without the articulating function, which is different from those of the da Vinci. Because it uses the same forceps as laparoscopic surgery, it is reported to be less expensive than the da Vinci. 15 Furthermore, Senhance is a state-of-the-art surgical robot that offers higher quality and stability than laparoscopic surgery owing to its hand motion elimination, motion scaling, tactile feedback, gaze-following camera, 3D vision, and unique cockpit.
There have been several reports on the use of Senhance for CRC; however, few studies have evaluated the safety of Senhance-assisted surgery vs conventional laparoscopic surgery for CRC.15-25 The purpose of this study was to confirm the non-inferiority of Senhance-assisted surgery regarding its short-term safety compared with conventional laparoscopic surgery for sigmoid colon cancer.
Methods
Study Design
This single-center retrospective comparative study included patients with sigmoid colon cancer who underwent a sigmoidectomy in our department between March 2020 and March 2025. The study was approved by Saitama Medical School International Medical Center (Approval No. 2021-088).
Patient backgrounds, short-term surgical outcomes, and pathological characteristics were compared between the two types of procedure (Senhance-assisted surgery and conventional laparoscopic surgery). The patients were divided after a paired match using propensity scores.
Patients of any age and sex who underwent laparoscopic colectomy as a curative treatment for sigmoid colon cancer were included. The exclusion criteria were as follows: stage IV colon cancer, chemoradiotherapy, recurrent cases, multiple cancers, and emergency surgery.
Data on patient age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, previous abdominal surgery, medical comorbidities, Numerical Rating Scale (NRS) pain scores (on postoperative days 1, 3, and 5), and TNM stage were retrospectively collected from electronic medical records. Postoperative complications were classified as grade 2 or higher according to the Clavien-Dindo system.26,27
Perioperative Management
Patients in both groups were admitted to the hospital one day before surgery. They were prohibited from eating from the time of admission. They received sodium picosulfate hydrate, magnesium citrate, dimethicone, kanamycin monosulfate, and metronidazole as bowel preparation for reducing anastomotic leakage. Postoperatively, patients started drinking water, were actively weaned from the bed on the first day, and were fed a soft diet on the third day. If there were no problems after the patients started eating, they were discharged from the hospital on the sixth or seventh day, and the first outpatient visit was made 1 month after surgery.
Surgical Technique
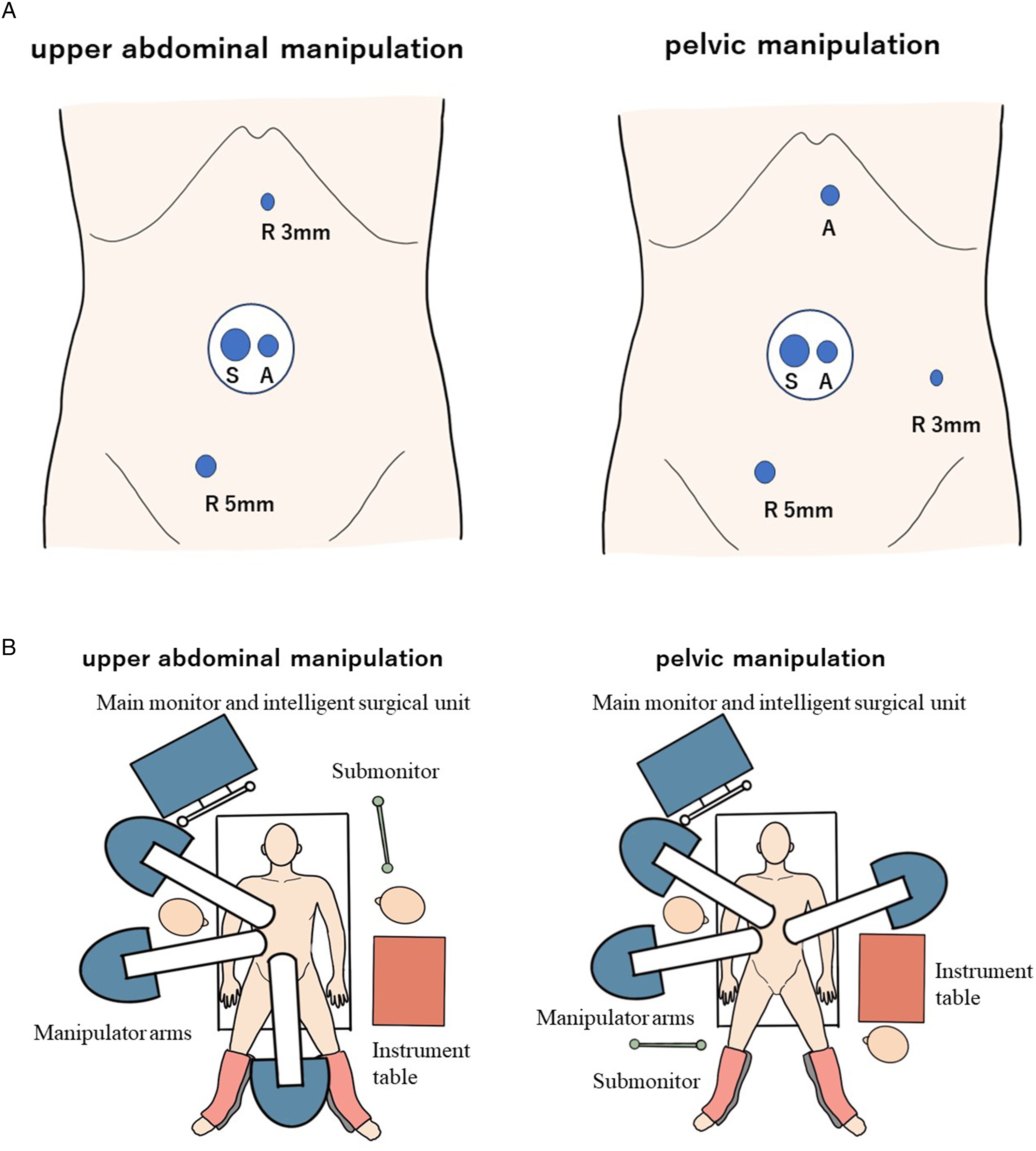
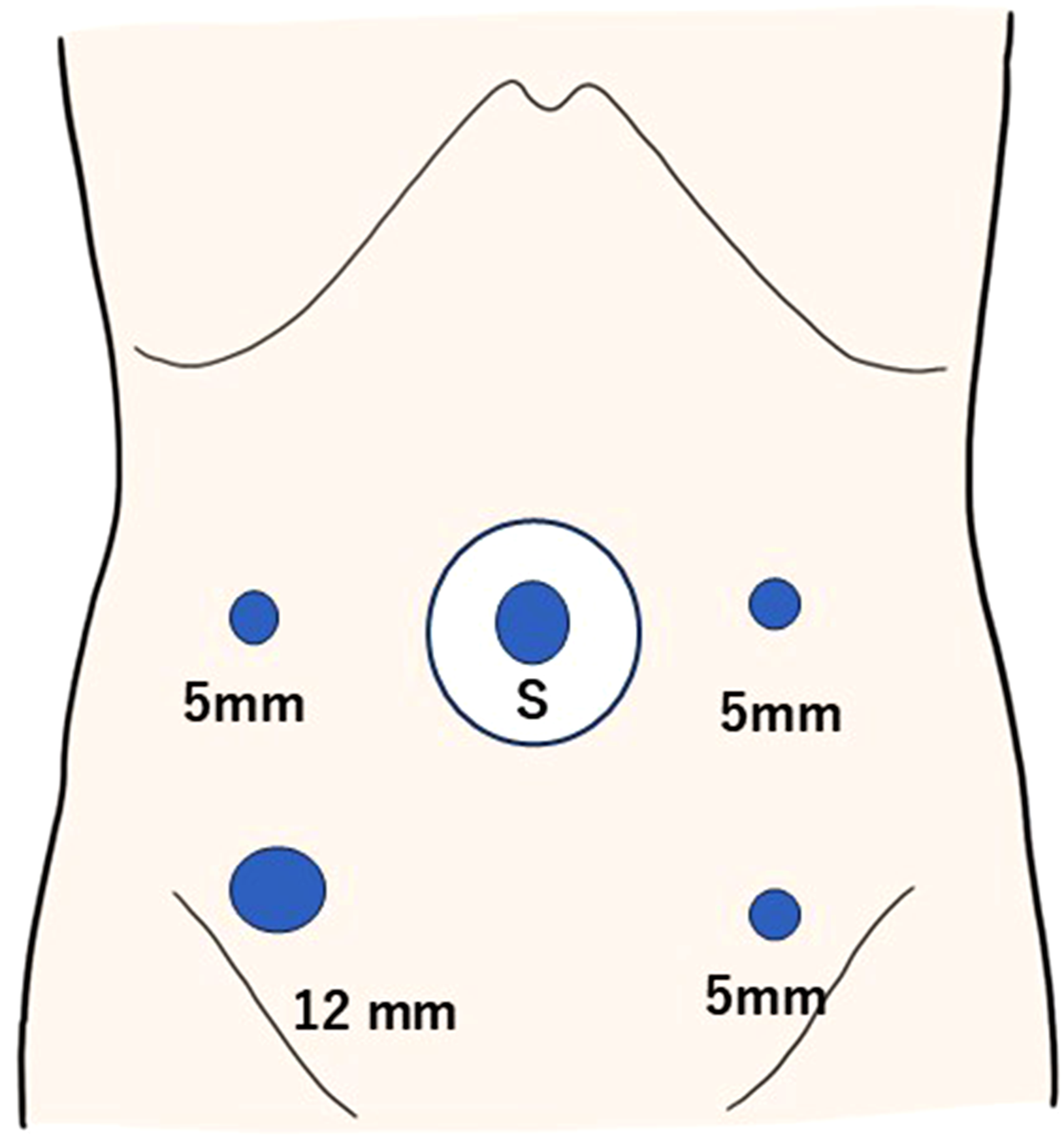
Senhance consists of a single manipulator arm, a cockpit, and an intelligent surgical unit that controls the digital signals from both arms and the video signal from the laparoscopic camera system (Figure 1). Forceps can be attached to any arm and moved to various approach sites by appropriately changing the arm to which the camera and forceps are attached. The Senhance-assisted and laparoscopic port arrangements for sigmoidectomy in our department are shown in Figures 2 and 3. In our department, small incisions preceded both procedures in the umbilical region. After opening the abdomen through a longitudinal incision of approximately 3 cm in the umbilical region, a lap protector (Hakko Shoji) and EZ access (Hakko Shoji) were placed. For Senhance-assisted surgery, the scope port and the assistant’s 12 mm port were placed in the EZ access, and two Senhance forceps ports (3 mm, upper abdomen; 5 mm, lower abdomen) were inserted for upper abdominal manipulation. During pelvic manipulation, the 3 mm upper abdomen port was changed to the left lower abdomen (Figures 2 and 3). The Senhance digital laparoscopy system (A) Manipulator arms; (B) intelligent surgical unit; and (C) cockpit 2-A Senhance-assisted port arrangements for sigmoidectomy. S, scope R, senhance forceps A, assistant. Figure 2-B Senhance docking for sigmoidectomy Laparoscopic port arrangements for sigmoidectomy. S, scope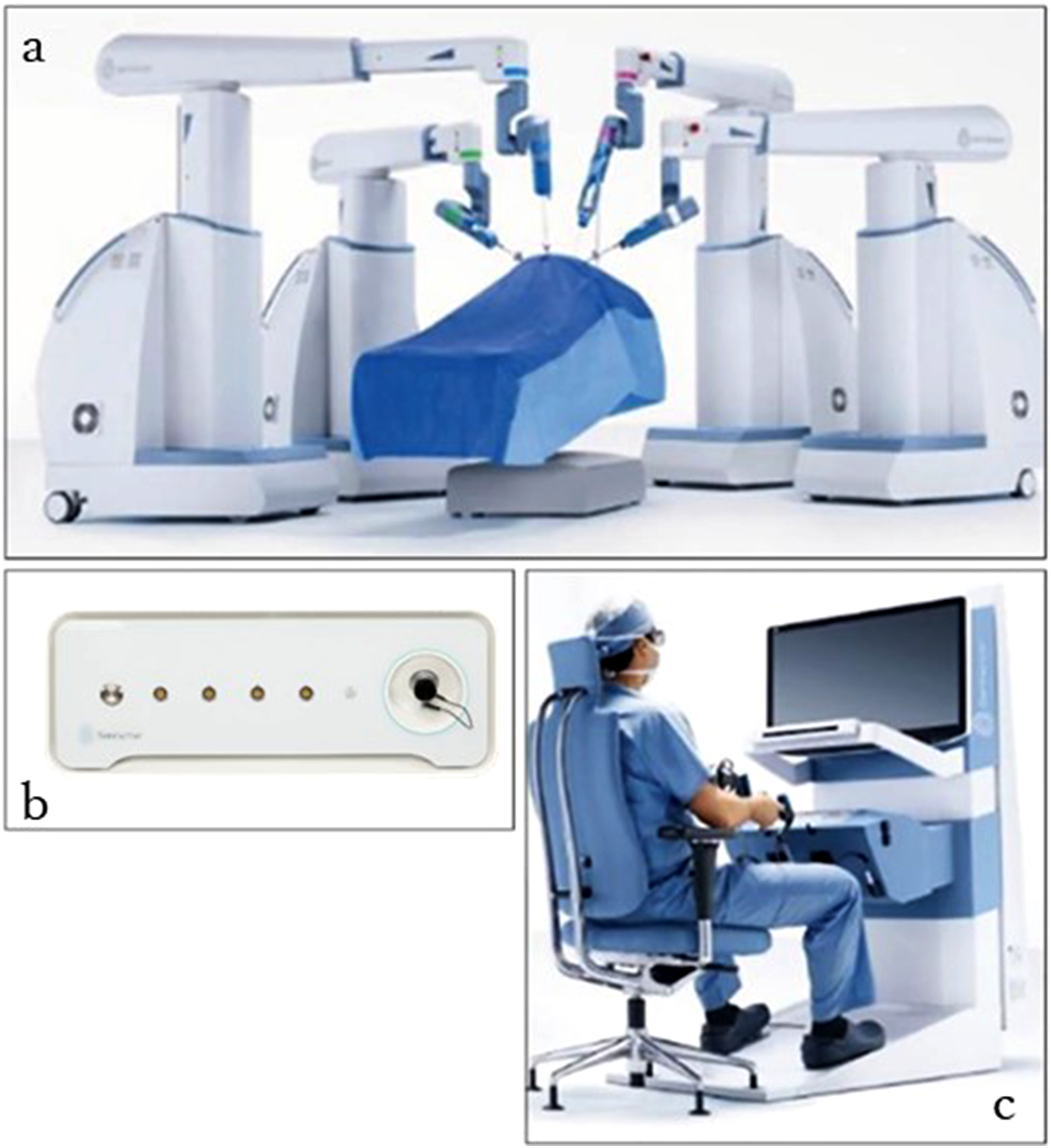
Senhance-assisted surgery is similar to general sigmoidectomy. The procedure starts with the medial approach of venturing the inferior mesenteric artery vascular stalk using an Internal Organ Retractor (B. Braun AESCULAP) (Figure 4). Port replacement and arm re-docking are required before pelvic manipulation. Functional end-to-end anastomosis or end-to-end anastomosis via a double stapling technique is performed, depending on the tumor’s location. An abdominal drain is generally not placed, although this depends on the case. Medial approach of venturing the inferior mesenteric artery vascular stalk using an internal organ retractor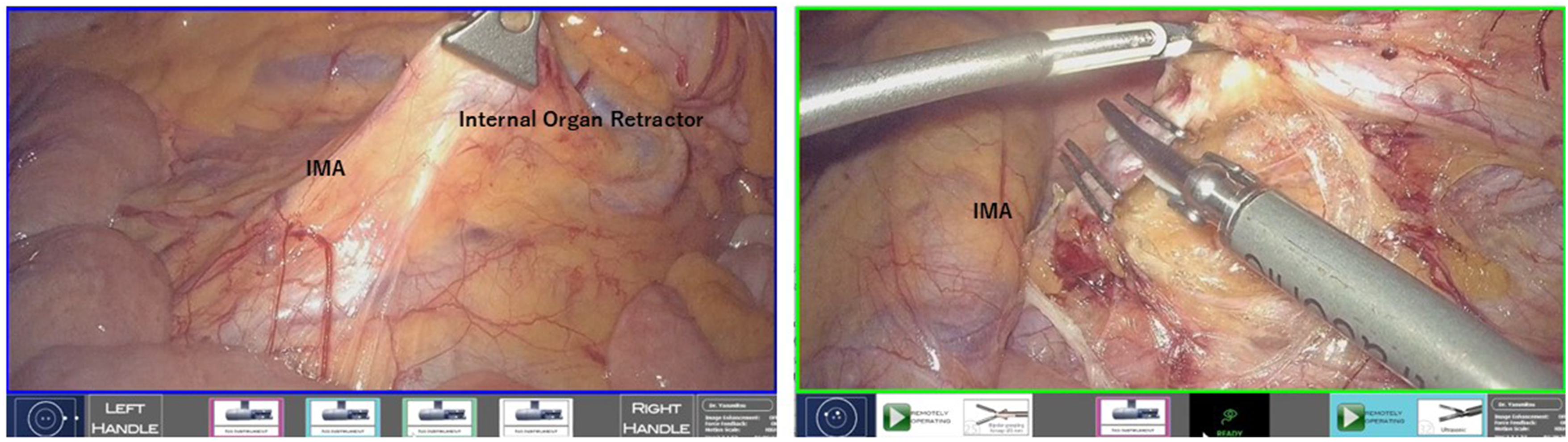
Propensity Score Matching (PSM)
Propensity scores were calculated for each patient using bivariate logistic regression based on the following covariates: age, sex, BMI, ASA score, previous abdominal surgery, cT, cN, cM, and cStage. These propensity scores matched patients in the Senhance-assisted surgery group (group S) in a 1:1 ratio with patients in the conventional laparoscopic surgery group (group C). We applied the nearest Mahalanobis metric matching within calipers, as defined by the propensity score (caliper = 0.02).
Statistical Analysis
Statistical analyses were performed using EZR software (Eazy R). Continuous variables were summarized as medians and ranges, and categorical variables as counts. Between-group comparisons were conducted using the Mann-Whitney U test for continuous variables and the Fisher’s exact test for categorical variables in univariate analyses with statistical significance set at P < .05.
Results
Characteristics Before and After PSM
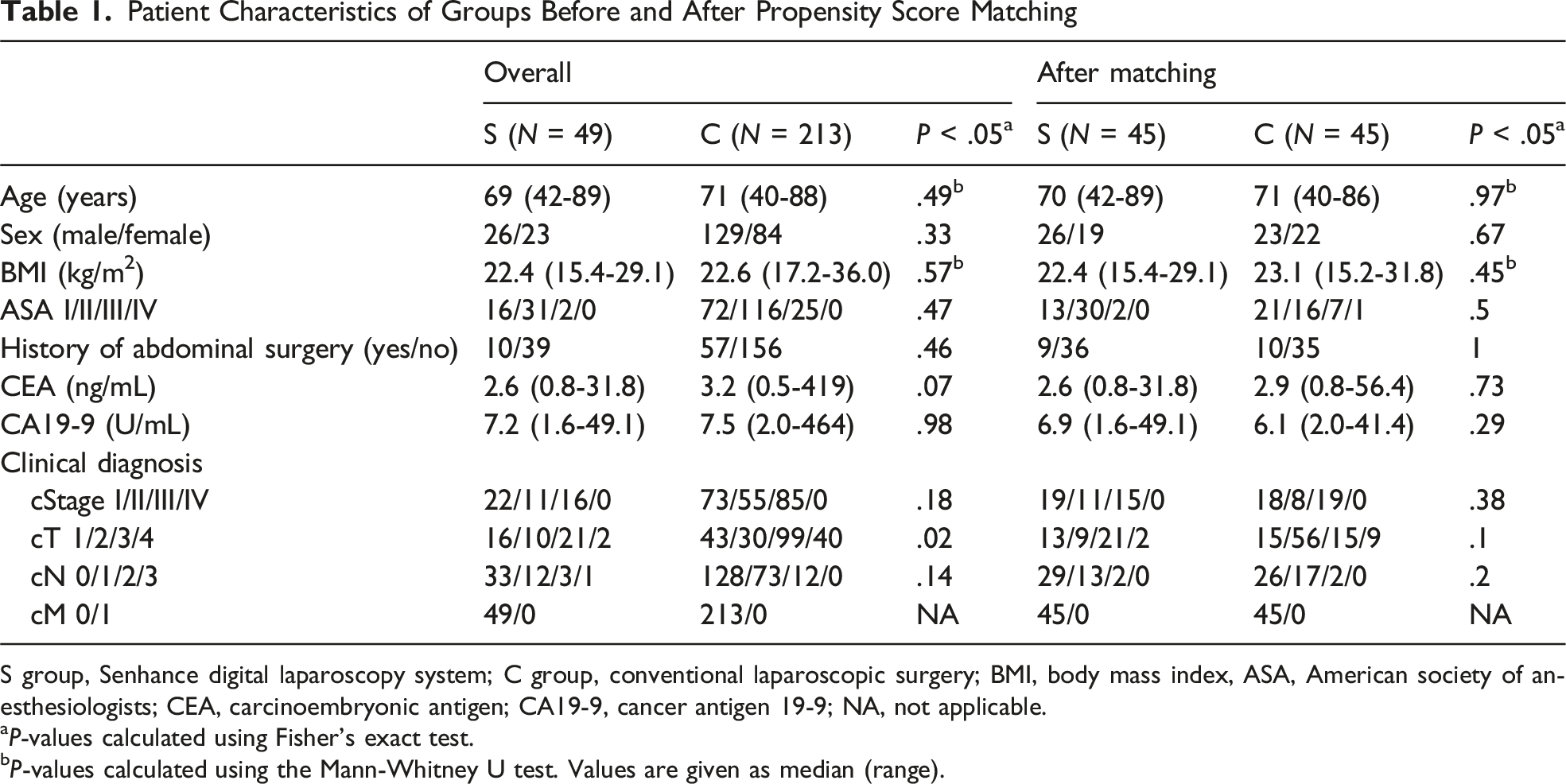
Between March 2020 and March 2025, 262 patients with sigmoid colon cancer underwent Senhance-assisted surgery (group S) or conventional laparoscopic surgery (group C). Before PSM, there were significant differences between the two groups regarding stages c (P = .01), cT (P = .02), and cN (P = .02). After PSM, each group included 45 patients and did not differ significantly in age, sex, BMI, ASA, tumor markers, previous abdominal surgery, cT, cN, cM, or cStage (Figure 5, Table 1). Patient propensity score matching. SR, sigmoid colon resection; S. Senhance digital laparoscopy system; C, conventional laparoscopic surgery; BMI, body mass index; ASA, American society of anesthesiologists Patient Characteristics of Groups Before and After Propensity Score Matching S group, Senhance digital laparoscopy system; C group, conventional laparoscopic surgery; BMI, body mass index, ASA, American society of anesthesiologists; CEA, carcinoembryonic antigen; CA19-9, cancer antigen 19-9; NA, not applicable. aP-values calculated using Fisher’s exact test. bP-values calculated using the Mann-Whitney U test. Values are given as median (range).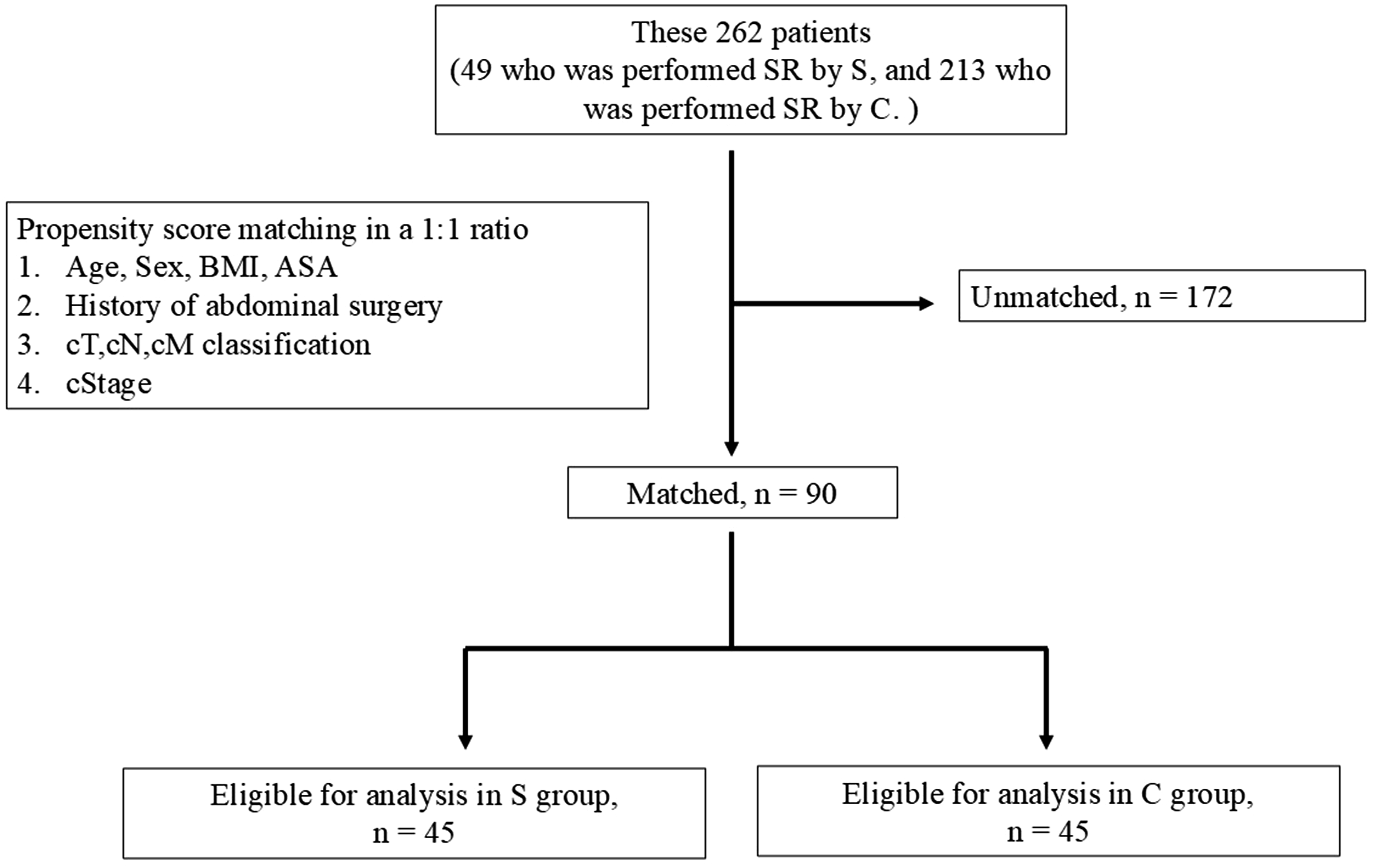
Peri- and Postoperative Outcomes After PSM
Peri- and Postoperative Outcomes After Propensity Score Matching
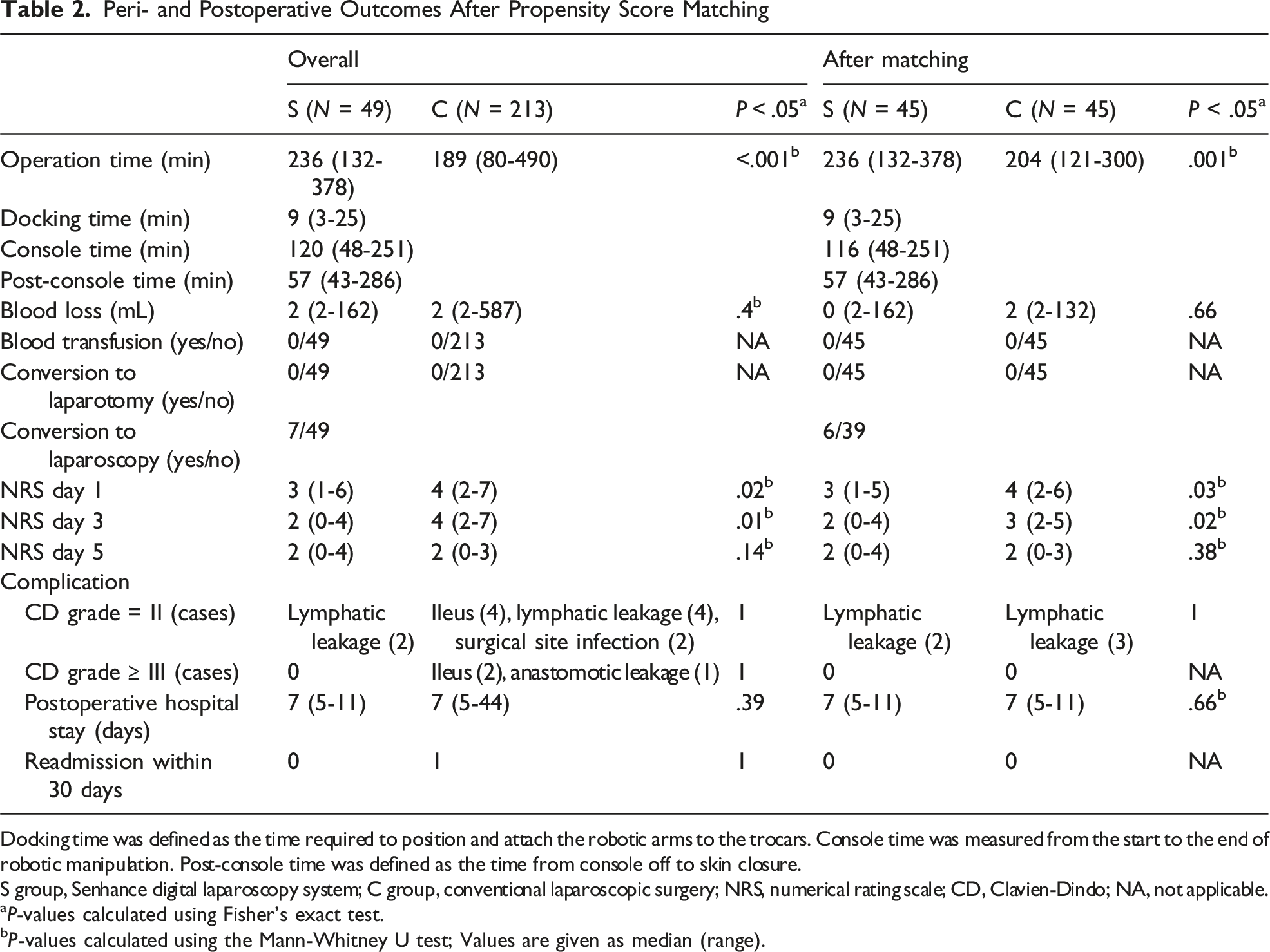
Docking time was defined as the time required to position and attach the robotic arms to the trocars. Console time was measured from the start to the end of robotic manipulation. Post-console time was defined as the time from console off to skin closure.
S group, Senhance digital laparoscopy system; C group, conventional laparoscopic surgery; NRS, numerical rating scale; CD, Clavien-Dindo; NA, not applicable.
aP-values calculated using Fisher’s exact test.
bP-values calculated using the Mann-Whitney U test; Values are given as median (range).
Pathological Findings After PSM
Pathological Findings After Propensity Score Matching
S group, Senhance digital laparoscopy system; C group, conventional laparoscopic surgery, BMI, body mass index, ASA, American society of anesthesiologists; NA, not applicable.
aP-values calculated using Fisher’s exact test.
bP-values calculated using the Mann-Whitney U test. Values are given as median (range).
Discussion
This study compared Senhance-assisted sigmoidectomy with laparoscopic colon surgery. Short-term outcomes for the two groups were comparable except for operation time. There were no blood transfusions, laparotomy transitions, or CD grade Ⅲ or higher postoperative complications in the Senhance-assisted surgery group. In addition, postoperative NRS scores on day 3 were significantly lower in the Senhance-assisted surgery group than in the conventional laparoscopic surgery group. Therefore, the present study demonstrated that Senhance-assisted sigmoidectomy was non-inferior to conventional laparoscopic surgery in terms of short-term safety outcomes. Comparing the da Vinci system with laparoscopic surgery, robotic surgery generally takes longer. 28 In the present study, the operation time was longer in the Senhance-assisted surgery group than in the conventional surgery group (236 min [132-378] vs 204 min [121-300]; P = .001). The relatively slower movement of the instruments and the limited range of motion of the robotic arms in the Senhance system may have contributed to the longer operative time because occasional repositioning or re-docking was required, particularly during pelvic dissection. Therefore, minimizing the time of forceps replacement and port docking is important, and effective port placement is necessary to shorten the operation time. It was previously reported that the camera and forceps manipulating the arms should be placed perpendicular to the direction of the surgical procedure to avoid re-setting because of the limited range of motion of the Senhance robotic arm. 22 In the case of sigmoid colon cancer, all surgical procedures can theoretically be completed in a right-to-left direction; therefore, our department uses a straight line in the cephalocaudal direction. The patients in this study underwent surgery using this port arrangement. In all cases requiring conversion to laparoscopy, this was attributed to the limited range of motion of the Senhance arms after re-docking during pelvic dissection. However, conversion was easily achieved because the Senhance system uses conventional laparoscopic trocars and instruments.
There were no significant differences in postoperative complications between groups. This indicates that Senhance-assisted surgery can be performed safely. High-resolution 3D vision provides more detailed visual information than conventional laparoscopic surgery, allowing the surgeon to perform surgery while recognizing more detailed anatomy. Senhance-assisted surgery for CRC has been reported to be safe in previous studies.17,18,21 Lin et al reported the short-term results of Senhance-assisted colorectal resection in 46 cases in Taiwan and advocated caution regarding its use. 19 The short-term results and safety assurance of Senhance-assisted colorectal surgery have also been reported for the early stages of its introduction and formulation of surgical techniques, including port placement.20-23 In the present study, Senhance-assisted surgery was performed as safely as laparoscopic surgery. The safety of Senhance-assisted sigmoidectomy for sigmoid colon cancer is therefore ensured, and this procedure is indicated for patients who can undergo laparoscopic surgery.
Postoperative NRS pain scores were significantly lower in the Senhance-assisted surgery group than in the conventional laparoscopic surgery group (3 [1-5] vs 4 [2-6], P = .03) and day 3 (2 [0-4] vs 3 [2-5], P = .02). This difference may be attributable, at least in part, to the system’s digital fulcrum function, which minimizes torque and stress at the trocar site, thereby reducing tissue trauma. In addition, the relatively slower movement of the instruments in the Senhance system may further decrease intraoperative manipulation stress on the abdominal wall and surrounding tissues, potentially contributing to reduced postoperative pain. More favorable postoperative pain outcomes with robotic surgery compared to laparoscopic surgery have been reported previously29,30, and the present study yielded similar finding.
The present study had some limitations however. First, it was a single-center, retrospective study, and therefore, its level of evidence was low compared to that of RCTs and multicenter studies. We used PSM to decrease bias and make the two groups comparable for sex, age, BMI, ASA score, previous surgery, tumor location, depth of invasion, and N classification. However, hidden bias might remain even after PSM to control for common variables that may influence prognosis. Second, although the prolonged operative time was considered to be mainly attributable to the technological limitations of the Senhance system, we did not assess the learning curve of the surgeons. Therefore, the potential influence of surgeon-related factors cannot be completely excluded. The learning curve for Senhance-assisted surgery should be addressed in future studies. Third, we did not objectively evaluate the physical or cognitive workload of the surgeons or the procedure cost. Future studies should include ergonomic and cost analyses to provide a more comprehensive evaluation.
Previously, Senhance has been compared with the da Vinci in another field 15 ; however, there are currently no such comparative reports in the field of colorectal surgery. In the field of CRC surgery, future studies comparing the Senhance and da Vinci systems should focus not only on clinical outcomes but also on ease of use, ergonomics, flexibility, and cost-effectiveness. The Senhance system allows unlimited reuse of forceps and utilizes the same ports and instruments as conventional laparoscopic surgery, which may help reduce running costs.
In conclusion, Senhance-assisted sigmoidectomy was non-inferior to conventional laparoscopic surgery regarding short-term safety outcomes. Further case studies are required to investigate the curative potential of this technique and its prognostic value.
Footnotes
Ethical Considerations
This study was approved by the Clinical Research Review Committee of Saitama Medical School International Medical Center (Approval No. 2021-088).
Consent to Participate
Informed consent was waived because of the retrospective design, with an opt-out option provided.
Consent for Publication
Consent for publication was waived as only anonymized data were used.
Author Contributions
Sohei Akuta conceived and designed the study, collected and analyzed the data, and drafted the manuscript. Yasuhiro Ishiyama, Misuzu Yamato, Takatsugu Fujii, and Chikashi Hiranuma contributed to patient data acquisition and assisted with data analysis. Yasumitsu Hirano and Yusuke Kinugasa supervised the study, critically revised the manuscript, and provided important intellectual input.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Yasumitsu Hirano: Consultant (Self): (Asensus Surgical), Honoraria (Self): (Asensus Surgical). Yusuke Kinugasa: Consultant (Self) (Johnson & Johnson K.K./JJKK), Consultant (Self) (Medtronic Japan Co., Ltd). Sohei Akuta, Yasuhiro Ishiyama, Misuzu Yamato, Takatsugu Fujii, and Chikashi Hiranuma have declared no conflicts of interest.
Data Availability Statement
The data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.