
Abstract
Purpose
This study aimed to describe perioperative outcomes associated with emergency cholecystectomy (EC) in elderly/high-risk patients based on Tokyo Guidelines 2018 (TG18).
Methods
A single-center retrospective surgical database included 2189 patients who underwent cholecystectomy between 2005 and 2025, and the study population included 550 patients who underwent EC for AC, excluding patients with elective cholecystectomy. The patients were divided into Grade I and II-III groups by AC severity. The patient characteristics and perioperative outcomes were compared between groups, and risk factors of severe postoperative complications were assessed using logistic multivariate analysis. Multiple linear regression analysis was performed to identify factors independently associated with the length of postoperative hospital stay.
Results
The patients with Grade I (n = 355) and those with Grade II-III (n = 195) were included. As a subgroup analysis, the Grade II-III group was divided into 2 groups: surgically low-risk patients (Low-risk, n = 82) and high-risk patients (High-risk, n = 113). The overall complication rate was approximately 15%. The rate of severe postoperative complications was 5.3%, and the 30-day mortality was zero in the entire cohort. The Grade II-III group had significantly more severe postoperative complications than the Grade I group (8.2% vs 3.7%, P = 0.028). There were no statistically significant differences in perioperative outcomes between the low-risk and high-risk groups, except for hospital stay. Multivariate analysis showed that LC (odds ratio = 0.414, P = 0.037) was associated with lower rates of severe postoperative complications.
Conclusions
EC may be a feasible option in selected elderly or comorbid patients with Grade II-III AC, with acceptable short-term outcomes.
Introduction
Acute cholecystitis (AC) is one of the most common reasons for patients to present to the emergency department with acute abdominal pain.1,2 In particular, elderly patients and those with multiple comorbidities are more likely to develop severe symptoms and complicate perioperative management.1,3-6 Emergency cholecystectomy (EC), especially laparoscopic cholecystectomy (LC), is a standard treatment for AC and is useful in terms of early symptom relief, improvement of quality of life, and prevention of recurrence. 7 However, the safety of EC in surgically high-risk patients, such as elderly patients and those with multiple comorbidities remains controversial. Approximately 40% of patients visiting emergency departments are over 65 years old, a percentage that is steadily increasing as the population ages, and it is expected that the number of high-risk patients will increase in the future.8,9 Therefore, we should reconsider how we treat patients who are currently considered to be at high risk.
The Tokyo Guidelines 2018 (TG18) is widely used as a treatment guideline for AC at present.10,11 TG18 classifies the severity of AC into Grade I (mild), Grade II (moderate), and Grade III (severe) and recommends treatment strategies according to the AC severity. TG18 also proposed the Charlson Comorbidity Index (CCI), including age adjustment as a surgical risk factor so that as a patient is older, their CCI score increases and they are considered to be at a higher risk. 12 Early gallbladder drainage, such as percutaneous transhepatic gallbladder drainage (PTGBD), after appropriate respiratory and circulatory management has been recommended for high-risk patients until recently. However, according to Loozen et al, a randomized controlled trial that compared LC and PTGBD in high-risk patients with AC found that LC had a much lower rate of major postoperative complications and reinterventions, but there were no significant differences in mortality. 13 In recent years, the data available in the current literature still cannot answer the question of what is the optimal treatment for AC in high-risk patients. In particular, there is limited evidence regarding the safety of EC for moderate-to-severe AC in high-risk patients.
Although large-scale national databases and multicenter collaborative studies have established that severe AC is associated with poor prognosis, limited knowledge remains regarding how surgeons make decisions in actual emergency settings, particularly in elderly patients and those with comorbidities. 2 Specifically, the balance between disease severity, physiological risk, surgical timing, and surgical approach remains unclear at the institutional level.
In this context, single-center experience remains valuable in clarifying how patient selection and surgical strategy translate into short-term safety. This study examined outcomes after EC for Grade II-III AC at a tertiary referral hospital, focusing specifically on elderly and high-risk patients, with the aim of utilizing this information for practical decision-making rather than simply replicating risk stratification. These findings help define practical safety boundaries for EC in high-risk patients in institutional settings where a drainage-first strategy cannot be routinely employed.
Methods
Patients
We retrospectively collected data from a surgical database of a single institution and included 2189 consecutive patients who underwent cholecystectomy between 2005 and 2025. 1639 patients with elective cholecystectomy were excluded, and 550 patients who underwent EC for AC were included in the study population (Figure 1). EC was defined as cholecystectomy performed within 72 h after admission (not symptom onset) with a diagnosis of AC. The diagnosis of AC is primarily based on TG18.12,14 The diagnosis was made based on systemic inflammatory signs, including fever, elevated C-reactive protein, and elevated white blood cell (WBC) count; local clinical signs, including Murphy’s sign, palpable mass in the right upper quadrant, and spontaneous pain; and imaging findings, including gallbladder enlargement, gallbladder wall thickening, and pericholecystic exudate. The severity of AC was also based on the TG18. Severe (Grade III) AC was defined as being accompanied by the presence of circulatory or respiratory disorders, central nervous system disorders, renal dysfunction, hepatic dysfunction, or blood coagulation abnormalities. Moderate (Grade II) AC was defined as the presence of any of the following: WBC count >18 000/mm3, palpable painful mass in the right hypochondrium, symptoms persisting for more than 72 h after the onset of symptoms, or significant local inflammatory findings (findings suggestive of gangrenous cholecystitis, emphysematous cholecystitis, pericholecystic abscess, bile peritonitis, etc.). Mild (Grade I) AC was defined as AC that did not meet the criteria for severe or moderate AC. Based on the severity of AC, the patients were divided into 2 groups: those with Grade I (Grade I group, n = 355) and those with Grade II-III (Grade II-III group, n = 195). In addition, we further divided the Grade II-III group into 2 groups for subgroup analysis: those with surgically low-risk group (Low-risk group, n = 82), and those with surgically high risk (High-risk group, n = 113). According to TG18, American Society of Anesthesiologists-physical status (ASA-PS) ≥3
15
or an age-adjusted CCI ≥6
16
is to be regarded as a surgical high-risk variable in Grade I and Grade II AC patients. In Grade III, high-risk variables were ASA-PS ≥3 or age-adjusted CCI ≥4, whereas the others were low-risk. The Clavien-Dindo Classification (CDC) was used to rate and group postoperative complications.
17
A CDC grade ≥ IIIa was defined as a severe postoperative complication. Thromboembolic complications included cerebral infarction, myocardial infarction, mesenteric infarction, pulmonary thromboembolism, and acute arterial embolism. The classification of postoperative bleeding complications followed the description provided by the International Society of Thrombosis and Haemostasis.
18
This definition includes many types of bleeding, such as luminal bleeding (eg, gastrointestinal bleeding), abdominal bleeding, cerebral hemorrhage, and abdominal wall hematoma. Surgical mortality was defined as death occurring within 30 and 90 days of a surgical procedure. Informed consent was obtained from all patients preoperatively. The study was approved by the Kokura Memorial Hospital Clinical Research Ethics Committee (#19061903) and complied with the Declaration of Helsinki. Consort diagram of the study. Abbreviations: EC: emergency cholecystectomy; AC: acute cholecystitis; ASA-PS Classification: The American Society of Anesthesiologists Physical Status classification; age-adjusted CCI: age-adjusted Charlson Comorbidity Index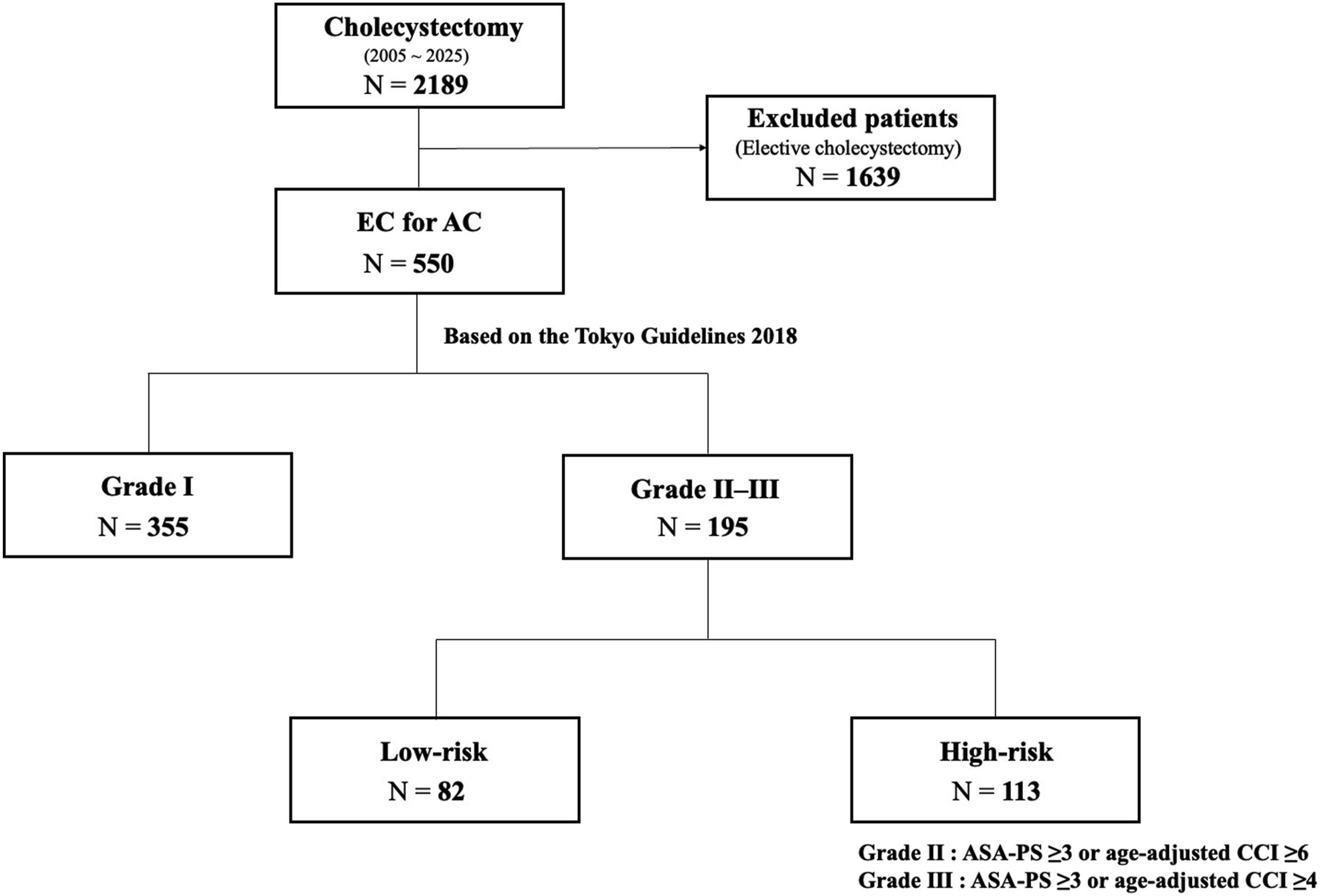
Statistical Analysis
Continuous variables are represented as mean (standard deviation) or median (range), whereas categorical variables are presented as absolute numbers and percentages. Fisher’s exact probability test was used to assess categorical variables for univariate comparisons. One-way analysis of variance and Tukey’s test were used to examine continuous variables for normally and non-normally distributed data, respectively. We selected clinically important factors and examined them using univariate analysis. A multivariate logistic regression analysis was conducted to identify the risk factors associated with severe postoperative complications (CDC ≥ IIIa). In multiple linear regression analysis, the following explanatory variables were included in the model: age, ASA-PS Classification ≥3, Grade II-III, LC, APT, and ACT. These factors were selected based on clinical relevance and previous studies. Important clinical variables such as timing from symptom onset, severity of systemic illness, and ICU admission were not consistently available and could not be included in the analysis. As a result of the preliminary multicollinearity assessment, high VIFs (6.08 and 6.69, respectively) were found between age and the age-adjusted CCI, so the age-adjusted CCI was excluded to ensure model stability. As a result, the VIFs of all variables were less than 5, and concerns about multicollinearity were resolved. Factors with a P-value of less than 0.05 in the univariate analysis were adopted as covariates in the multivariate analysis. All P-values were calculated using a two-sided test, and those with a value less than 0.05 were deemed to be statistically significant. Statistical analyses were conducted using EZR, a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria, version 1.68), at the Saitama Medical Center, Jichi Medical University. Specifically, it is an altered iteration of the R commander created to incorporate the statistical functions often utilized in the field of biostatistics. 19
Results
Patient and Perioperative Characteristics
Patient Characteristics in the Current Cohort
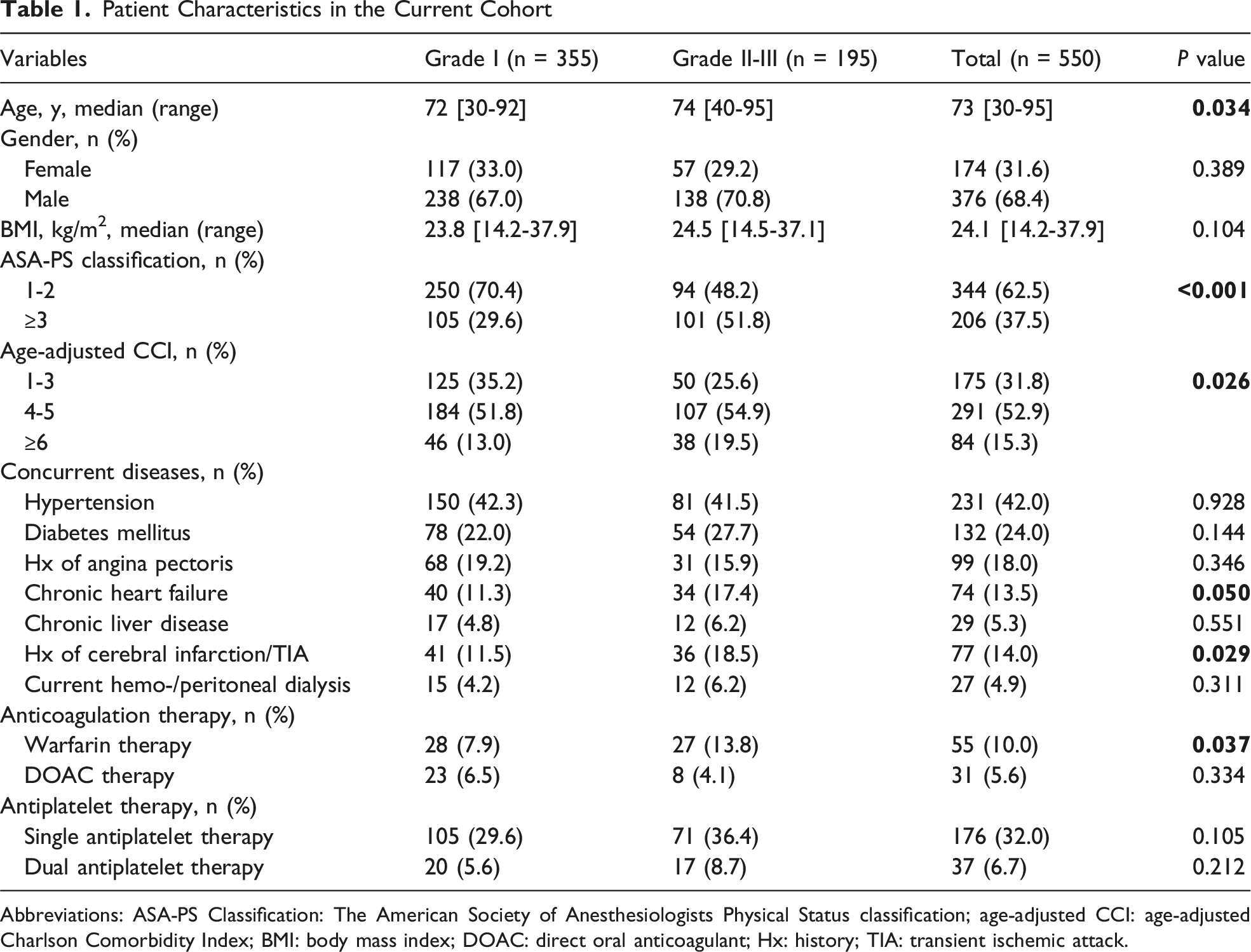
Abbreviations: ASA-PS Classification: The American Society of Anesthesiologists Physical Status classification; age-adjusted CCI: age-adjusted Charlson Comorbidity Index; BMI: body mass index; DOAC: direct oral anticoagulant; Hx: history; TIA: transient ischemic attack.
Perioperative Outcomes in the Current Cohort
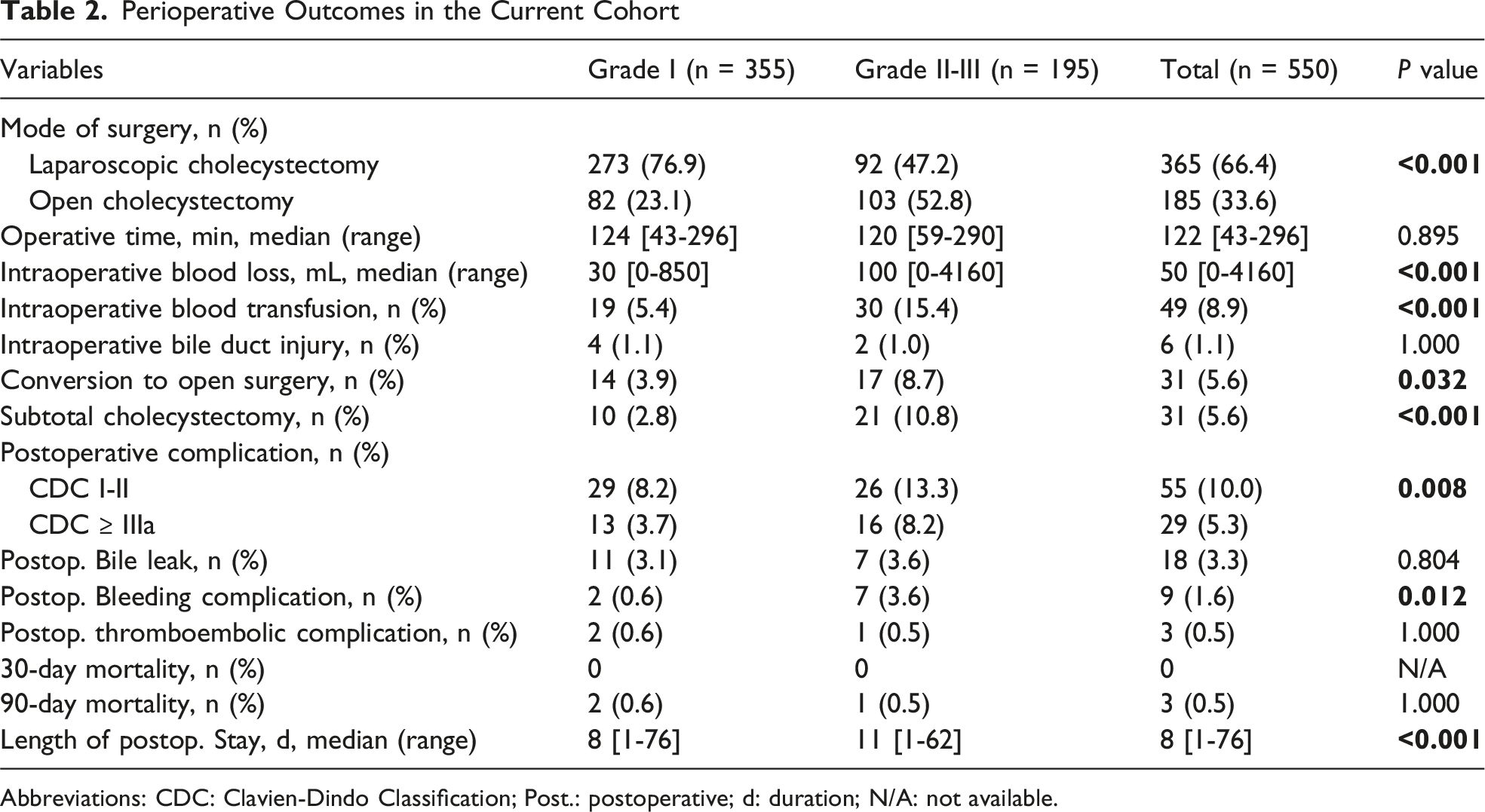
Abbreviations: CDC: Clavien-Dindo Classification; Post.: postoperative; d: duration; N/A: not available.
Patient Characteristics in Subgroup Analysis
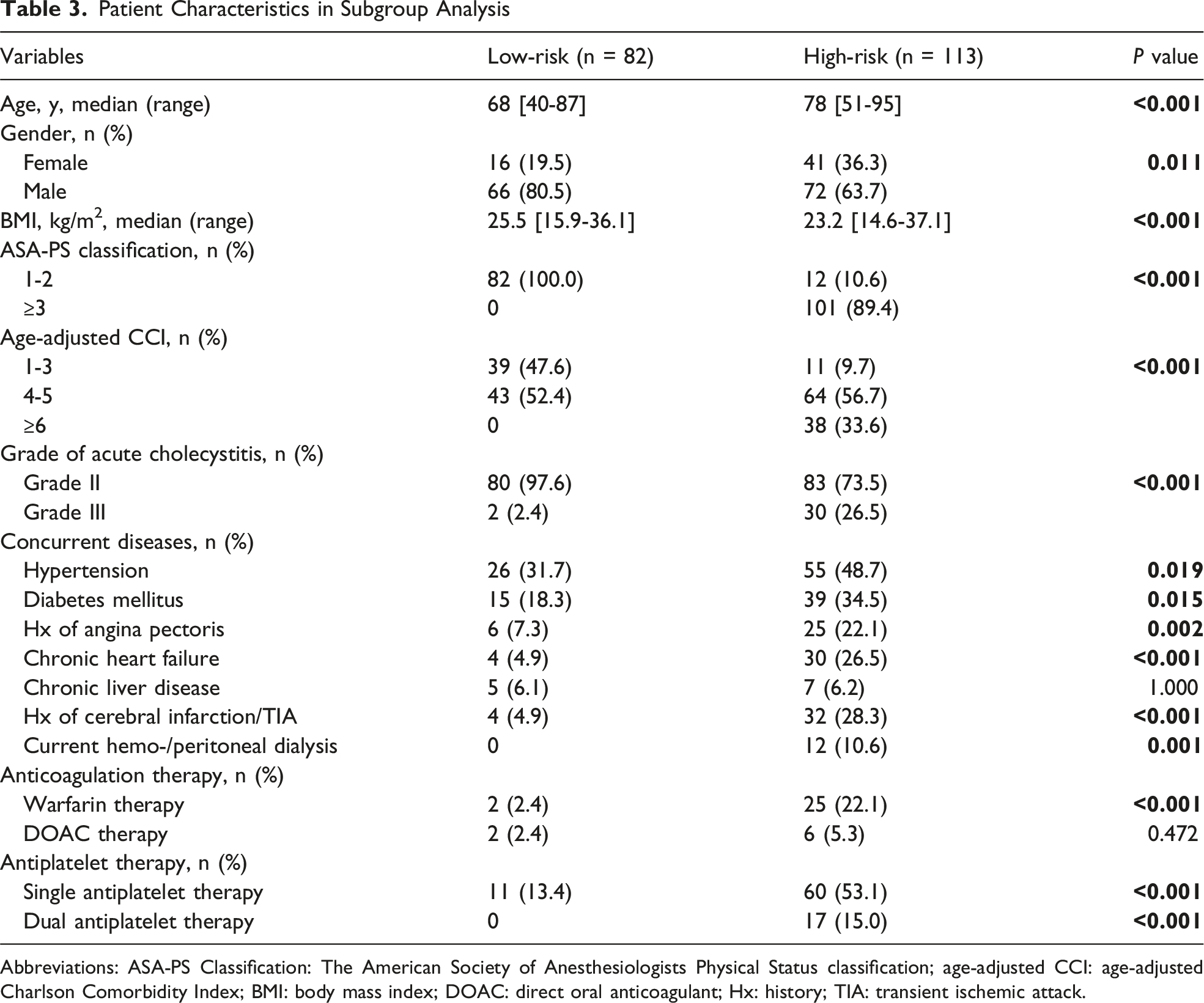
Abbreviations: ASA-PS Classification: The American Society of Anesthesiologists Physical Status classification; age-adjusted CCI: age-adjusted Charlson Comorbidity Index; BMI: body mass index; DOAC: direct oral anticoagulant; Hx: history; TIA: transient ischemic attack.
Perioperative Outcomes in Subgroup Analysis
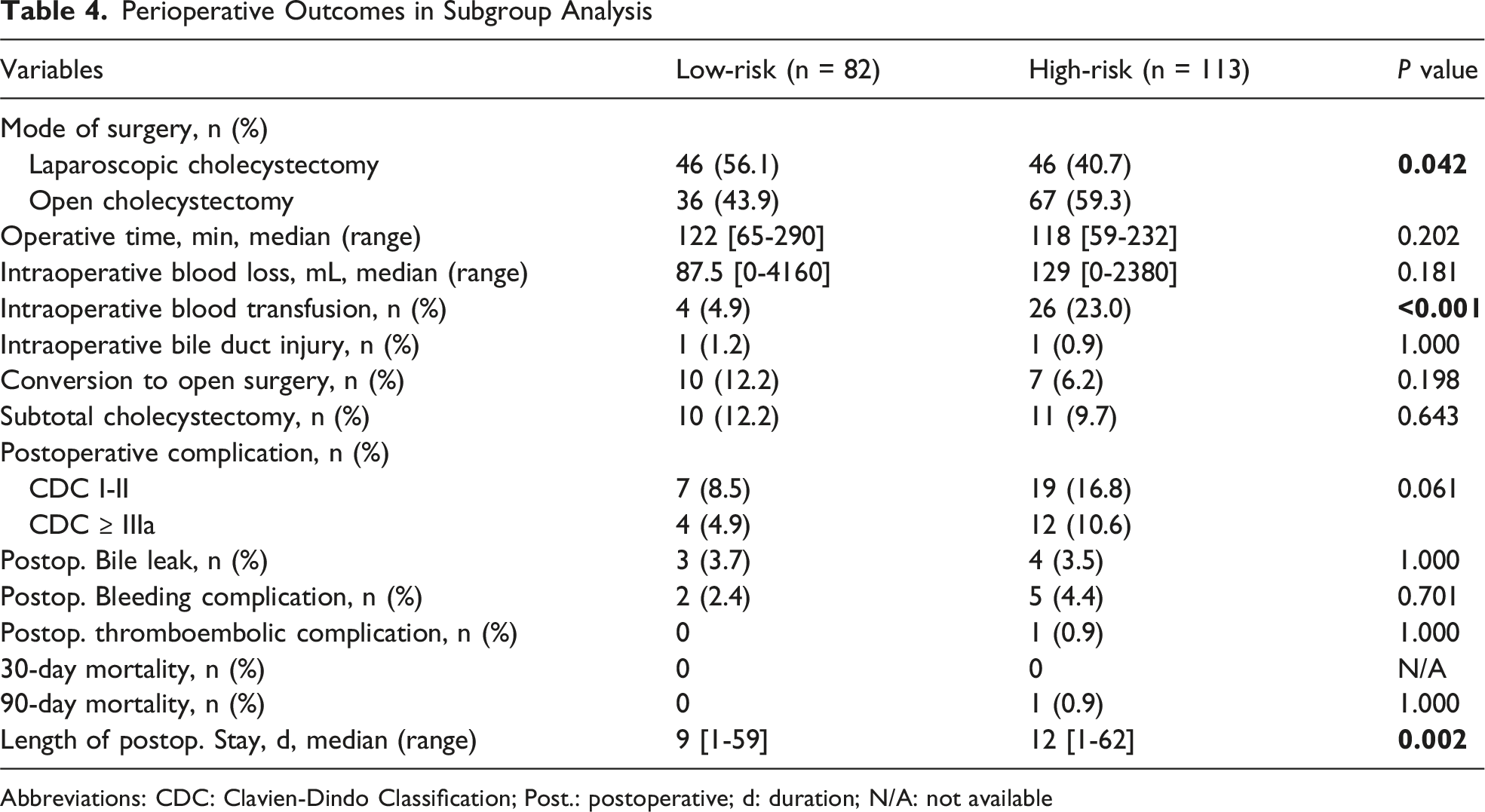
Abbreviations: CDC: Clavien-Dindo Classification; Post.: postoperative; d: duration; N/A: not available
Risk Factors Affecting Severe Postoperative Complications (Clavien-Dindo Classification ≥ IIIa)
Univariate and Multivariate Analysis of Severe Postoperative Complications (Clavien-Dindo Classification ≥ IIIa)
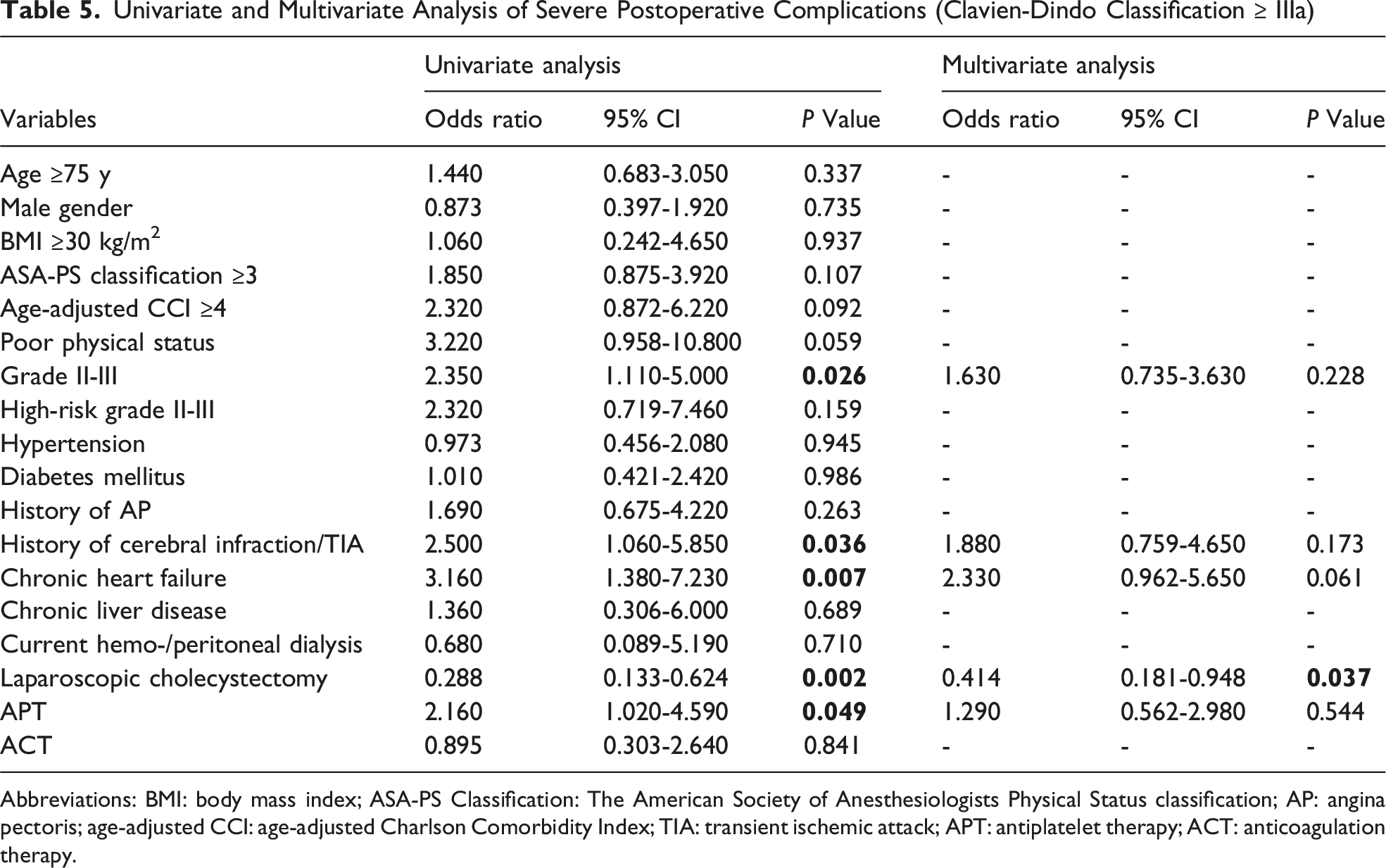
Abbreviations: BMI: body mass index; ASA-PS Classification: The American Society of Anesthesiologists Physical Status classification; AP: angina pectoris; age-adjusted CCI: age-adjusted Charlson Comorbidity Index; TIA: transient ischemic attack; APT: antiplatelet therapy; ACT: anticoagulation therapy.
Predictive Factors Associated With Length of Postoperative Hospital Stays
Multiple Linear Regression Analysis of Predictive Factors Associated With Length of Postoperative Hospital Stays
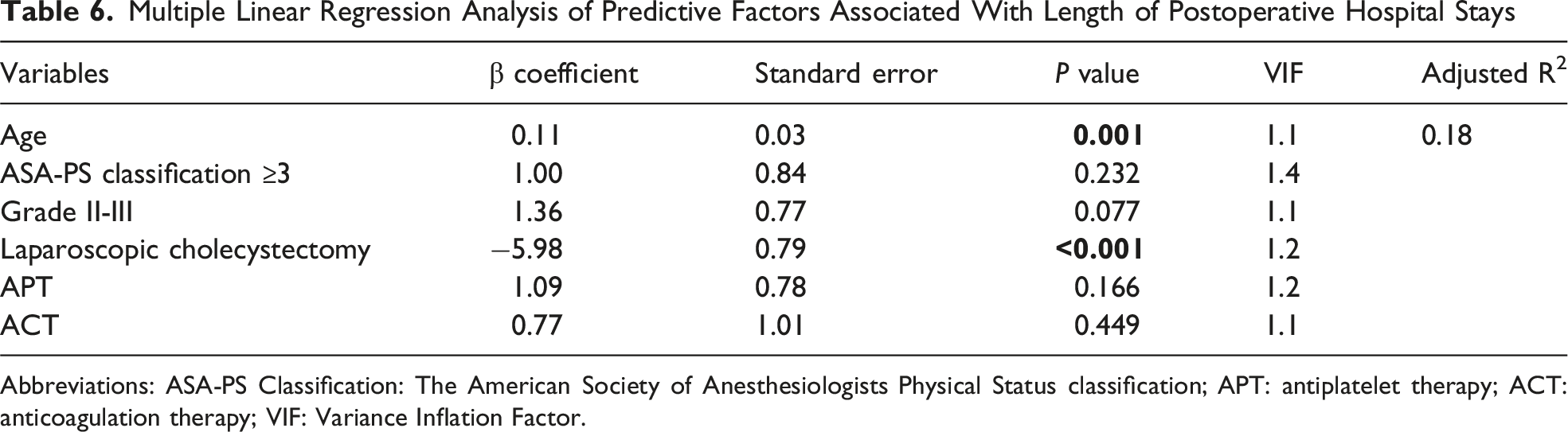
Abbreviations: ASA-PS Classification: The American Society of Anesthesiologists Physical Status classification; APT: antiplatelet therapy; ACT: anticoagulation therapy; VIF: Variance Inflation Factor.
Discussion
This is a single-center retrospective study at a tertiary referral hospital to evaluate perioperative outcomes of emergency cholecystectomy for Grade II-III acute cholecystitis in surgically high-risk patients based on TG18. Intraoperative blood loss, intraoperative blood transfusion rate, conversion rate to open surgery, and subtotal cholecystectomy were significantly higher in the Grade II-III group than in the Grade I group, suggesting a higher difficulty of surgery. In the Grade II-III groups, although the incidence of severe postoperative complications (CDC ≥ IIIa) was 8.2%, the 30-day mortality was 0%, which was a low short-term mortality, despite a moderate overall complication burden. There were no statistically significant differences in the rate of severe postoperative complications between the low-risk and high-risk groups, although the study may have been underpowered to detect small differences. The high-risk group had poorer conditions in terms of background factors (age, comorbidities, etc.), but the perioperative outcomes were not significantly different from those of the low-risk group. Traditionally, conservative treatment and gallbladder drainage have been prioritized for high-risk patients, and surgical intervention has required careful judgment. However, this study suggests that EC may be a feasible option in selected high-risk patients.
Multivariate analysis of this study showed that LC was an independent factor associated with lower rates of severe postoperative complications (odds ratio = 0.414, P = 0.037), although this finding may reflect selection bias. In addition, LC also contributed to shortening the length of postoperative hospital stay. From these results, it can be said that LC has many advantages and may be considered a preferred approach for AC when feasible.6,20 However, LC is not necessarily applicable to all cases. In fact, LC was selected in only 66.4% of AC in this study. In situations such as dense adhesions around the gallbladder, gallbladder perforation, and Mirizzi syndrome, the decision to promptly switch to open conversion or subtotal cholecystectomy is necessary. Therefore, rather than expanding the indications for LC uniformly, it will be important to select surgical procedures according to the condition of each patient. The risk of perioperative complications is likely multifactorial and influenced by disease severity, patient comorbidities, and the need for open surgery or bailout procedures.
As the aging of society progresses, the number of elderly patients with cholelithiasis and those with multiple comorbidities is increasing, and the number of patients receiving antithrombotic therapy (ATT) is also increasing.21,22 As risk assessment using the age-adjusted CCI is proposed by TG18, the number of patients with AC considered to be at high risk is expected to increase. In this study, 57.9% of the Grade II-III group were classified as high risk. For high-risk patients, conservative treatment and gallbladder drainage are often preferred, but PTGBD may be difficult in patients undergoing ATT due to the risk of bleeding complications. 23 In such cases, the usefulness of endoscopic transpapillary gallbladder drainage (ENGBD) has been reported,24,25 but it is technically difficult and difficult to universally perform in emergency situations. Given this background, the importance of EC is expected to increase in the future. In recent years, the safety of EC has been supported even in patients receiving ATT.26,27 In this study, although the proportion of ATT patients was high, the rate of postoperative bleeding complications was 1.6%, and the 30-day mortality rate was zero, demonstrating favorable results. Furthermore, some reports suggest that EC has better perioperative outcomes than gallbladder drainage, even in high-risk patients,13,28 indicating that with appropriate perioperative management and case selection, EC may be able to be performed safely even in elderly, high-risk patients. Although many tools and scoring systems have been reported to assess the functional status of elderly surgical patients,29,30 there is no consensus on which of the existing surgical risk scores is better at predicting postoperative mortality in AC. In the future, it is expected that risk assessment tools that will enable more detailed patient stratification will be developed, and prospective randomized controlled trials will be conducted to establish optimal treatment strategies for AC in high-risk patients.
Another important decision point in the treatment of Grade II-III AC is whether to perform percutaneous gallbladder drainage before definitive surgery. 12 Although some guidelines recommend percutaneous cholecystostomy as an alternative strategy for high-risk patients, it was not routinely used in this cohort. This reflects our institutional practice, as many patients presented with cardiovascular or cerebrovascular disease and were receiving antithrombotic therapy. In such patients, urgent percutaneous intervention is considered to carry a significant risk of bleeding complications. 31 Therefore, this study does not evaluate a strategy that prioritizes percutaneous cholecystostomy (PC), but rather characterizes outcomes after upfront EC. These findings do not contradict the TG18 recommendations; rather, we believe that percutaneous cholecystostomy remains an appropriate option in certain patients, and these data describe the outcomes in a situation where EC was preferred in the initial stages. Therefore, these findings should be interpreted as suggesting the safety profile of definitive surgical treatment in a decision-making framework where the availability of alternative minimally invasive treatment options is inherently limited. In the same framework, robot-assisted cholecystectomy was not incorporated into the treatment algorithm of this study. In Japan, robotic-assisted cholecystectomy is not covered by national health insurance, significantly limiting its availability, especially in emergency medical settings. As a result, surgical decision-making in this cohort was limited to laparoscopic or open surgery. This unique health care system context is important for considering the generalizability of our findings. However, because laparoscopic and open surgery remain the primary treatments for EC in many institutions worldwide, our findings continue to provide practical insights into actual surgical decision-making for severe AC.
Clinical Implications for Decision-Making in Grade II-III Acute Cholecystitis
The results of this study provide several practical implications for surgeons managing moderate to severe AC. First, despite increased disease severity, the 30-day mortality rate in this cohort remained low, suggesting that Grade II-III AC alone should not preclude consideration of early definitive surgery if physiological stabilization is achievable. This difference highlights the importance of distinguishing between perioperative resource utilization and surgical safety when evaluating the indications for EC in elderly patients or those with comorbidities. Second, the observed association between LC and reduced serious complications should be interpreted with caution. This finding does not suggest a direct preventive effect of LC, but rather likely reflects the feasibility of minimally invasive surgery in cases with appropriate patient selection and favorable intraoperative conditions. Therefore, a primary laparoscopic approach may be a realistic strategy in experienced centers that prioritize discretion and flexibility over adherence to a surgical procedure.
This study has several limitations. First, because it is a single-center retrospective study for long time period, there may have been selection bias and changes in surgical techniques and perioperative management over the long study period may have influenced outcomes. Second, this study does not include patients who did not undergo surgery (including those managed with drainage or conservative treatment), which limits direct comparisons between treatment strategies. Third, because this study was conducted at a tertiary referral hospital, the results were obtained with skilled and experienced surgeons and a sufficient perioperative management system and therefore may not necessarily be applicable to general facilities. Fourth, separate analysis of Grade III AC was limited by the relatively small number of Grade III cases in this cohort.
Conclusions
EC for Grade II-III AC in elderly or comorbid patients was associated with acceptable short-term outcomes in this selected surgical cohort, with low mortality and a moderate incidence of complications. These findings support the possibility of selective early definitive surgery, taking into account the patient’s physiological characteristics, the surgeon’s judgment, and the facility’s capabilities.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.