
Abstract
Comorbidity burden in patients with acute cholecystitis (AC) managed by percutaneous cholecystostomy tube (PCT) placement may determine whether patients progress to cholecystectomy (CCY) or require ongoing non-operative management. This retrospective observational case series examined 139 patients admitted with PCT placement for AC at a rural Appalachian tertiary referral center between October 2020 and March 2025. The most prevalent comorbidities among these patients were hypertension (79.9%), smoking (61.2%), and hyperlipidemia (47.5%). Of the 139 patients, 31.7% (n = 44) underwent subsequent CCY and had 78.7% lower 6-month mortality compared to those managed non-operatively (P < .001). Patients progressing to CCY had significantly lower Charlson Comorbidity Index (CCI) scores (3.89 vs. 5.57, P = .05) and were significantly less likely to have active cancer (P = .002), COPD (P = .001), or CHF (P = 0.032). In resource-constrained environments where advanced endoscopic alternatives are unavailable, these comorbidity profiles can guide preoperative risk stratification and inform individualized counseling regarding anticipated treatment pathways after PCT.
Early laparoscopic CCY remains the standard of care for symptomatic acute cholecystitis (AC). 1 However, a substantial proportion of patients presenting to rural hospitals carry significant comorbidity burdens that render them poor candidates for immediate surgery. The Tokyo Guidelines 2018 (TG18) recommend that patients with Grade III AC and a Charlson Comorbidity Index (CCI) ≥4 be considered poor candidates for early laparoscopic CCY. 2 In these instances, TG18 advises percutaneous cholecystostomy tube (PCT) placement followed by delayed CCY. Percutaneous cholecystostomy tube placement is associated with significant clinical improvement within 48 hours and serves as an effective temporizing measure. 3 However, many patients who receive a PCT never proceed to definitive surgery. The comorbidity burden that initially precluded surgery often persists or worsens, effectively defining the patient’s long-term treatment trajectory. This distinction, between patients who can ultimately be brought to the operating room and those for whom PCT becomes the definitive intervention, is critically important for preoperative counseling and resource allocation, particularly in settings where advanced endoscopic alternatives such as EUS guided gallbladder drainage are not available. This study aims to identify the specific comorbidities that differentiate patients who progress to CCY after PCT placement from those who do not and to contextualize these findings within the practical management challenges of a rural, resource-constrained Appalachian setting.
This retrospective observational case series was IRB approved (#00003204) and conducted at a tertiary referral center in rural Appalachia. The study involved 139 adult patients admitted for AC who underwent PCT placement between October 1, 2020, and March 15, 2025. Patients were stratified into two groups: those who underwent subsequent CCY and those managed with PCT alone. Comorbidity burden was quantified using the CCI calculated at the time of admission. The primary outcome was 6-month all-cause mortality. Secondary outcomes included rates of specific comorbidities between groups. Data was analyzed using descriptive statistics, chi-squared test for categorical variables, and Mann-Whitney U test for continuous variables given non-normal distribution of CCI scores. Odds ratios with 95% confidence intervals were calculated for comorbidity comparisons.
The most common comorbidities among the identified patients with PCT placement were hypertension (79.9%), smoking (61.2%), and hyperlipidemia (47.5%). From the 139-patient sample, 31.7% (n = 44) underwent subsequent CCY. Patients who progressed to CCY had a 78.7% lower rate of mortality within 6 months after admission compared to those who never had a subsequent CCY [95% CI: 46.4%-90%] (P < 0.001).
Comorbidity burden, as measured by CCI, was significantly lower in patients who proceeded to CCY compared to PCT alone (median CCI 3.89 [IQR 2.25-6.00] vs 5.57 [IQR 4.00-7.00], P = 0.05). The comorbidities most strongly associated with non-progression to CCY were active cancer (91.8% less likely to progress, [95% CI: 36.9%-98.9%], P = 0.002), COPD (87.5% less likely, [95% CI: 56.6%-96.4%], P = 0.001), and CHF (62.8% less likely, [95% CI: 7.2%-85.1%], P = 0.032) (Figure 1). These three comorbidities, along with the overall CCI score, effectively identified a population for whom PCT placement functions not as a bridge to surgery but as the definitive management strategy. Statistically significant differences in comorbidities between PCT with delayed CCY group and PCT alone group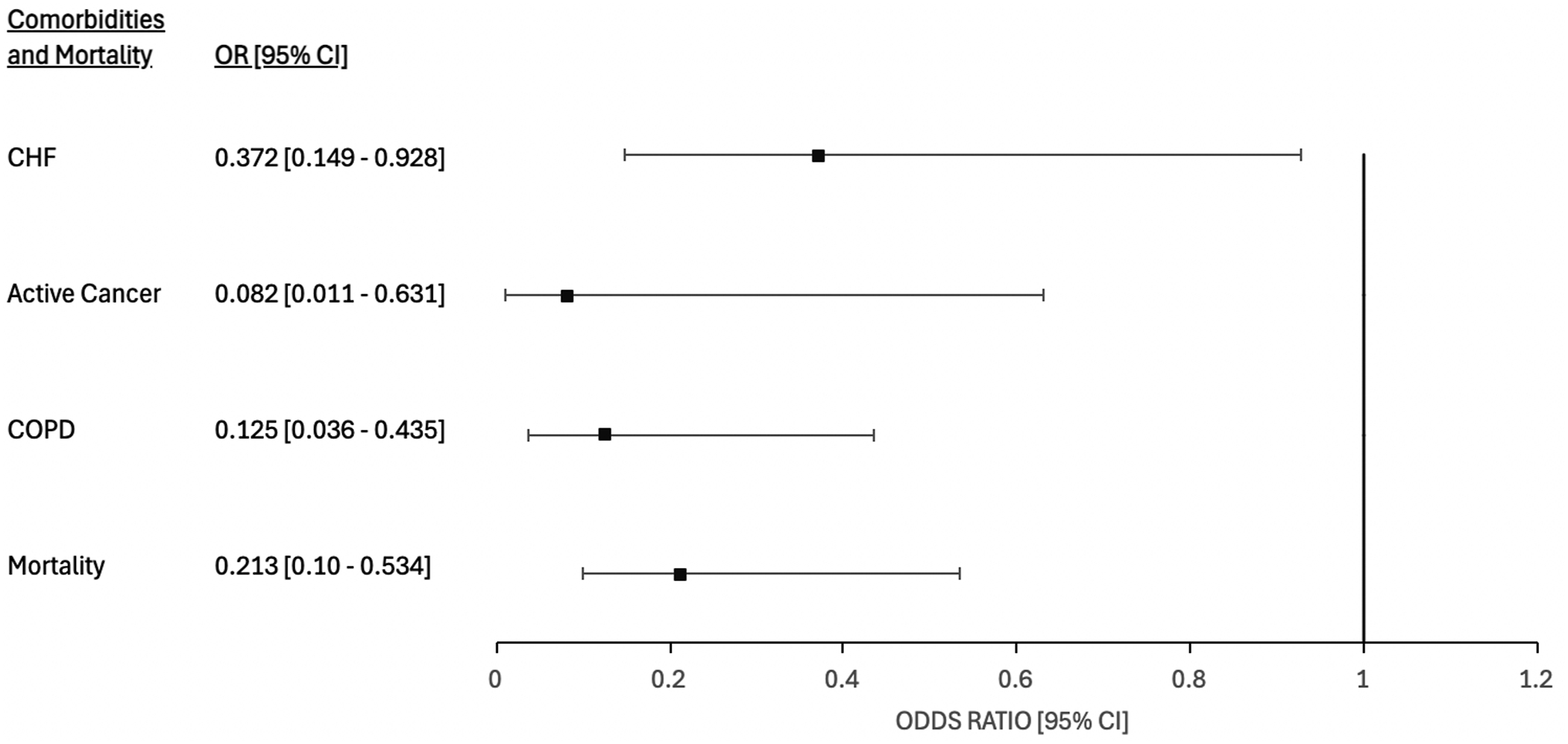
These findings demonstrate that comorbidity burden defines treatment pathways after PCT placement for AC. In our rural Appalachian patient population, the presence of active cancer, COPD, or CHF, and an elevated CCI score, identified patients who were unlikely to progress to definitive surgical management and who carried substantially higher 6-month mortality. This has direct implications for how clinicians counsel patients and their families at the time of PCT placement. Patients with these comorbidities should be informed that surgery may not be feasible and that a non-operative management strategy is the likely trajectory.
The management pathway for patients who do not progress to CCY is an area where practical guidance remains limited, particularly outside of high-volume academic centers. A recent international Delphi consensus study 4 recommended that patients with CCI ≥6 and ASA-PS ≥4 who are deemed non-surgical candidates should retain their PCT for a minimum of 3 weeks, after which tube cholangiography should confirm biliary tree patency before tube removal is considered. At our institution, patients who do not undergo CCY are reassessed for surgical candidacy at outpatient follow-up. Tube removal is considered only after documented resolution of the acute episode and radiographic confirmation of a patent cystic duct in the absence of residual gallstones. For patients with persistent cystic duct obstruction, calculous disease, or ongoing surgical unsuitability, the PCT is maintained with periodic exchanges and clinical reassessment. Thresholds for reconsidering surgery include stabilization or resolution of the index comorbidity (e.g., completion of cancer treatment, optimization of CHF), improvement in functional status, and patient preference following informed discussion.
In contemporary practice, alternatives to PCT and CCY are increasingly discussed. EUS guided gallbladder drainage (EUS-GBD) using metal stents has demonstrated a favorable safety profile compared to percutaneous drainage, with lower rates of adverse events and fewer reinterventions.5,6 Professional societies including the American Gastroenterological Association and the European Society of Gastrointestinal Endoscopy have endorsed EUS-GBD as an alternative in high-risk surgical patients. 7 However, these modalities require advanced endoscopic expertise, specialized equipment, and institutional infrastructure that are not widely available in rural and resource-constrained settings. In Appalachia, where specialty surgical services are limited, PCT remains the most accessible and practical drainage modality for high-risk patients with AC.8,9 Our experience therefore reflects the reality for a significant proportion of patients and providers nationwide who manage AC without access to advanced endoscopic alternatives.
This study successfully identified that comorbidity burden, particularly active cancer, COPD, and CHF, defines the treatment trajectory for patients managed with PCT for AC. These findings suggest that comorbidity burden plays a critical role in determining progression to definitive surgical management. In resource-constrained environments, where advanced endoscopic alternatives are unavailable, these comorbidity profiles serve as practical tools for risk stratification and anticipatory patient counseling. Future investigations should evaluate longitudinal outcomes in patients managed non-operatively, including rates of recurrent AC, PCT-related morbidity (such as tube complications), the need for repeat interventions, and the efficacy of protocolized reassessment pathways to improve outcomes in this high-risk population.10,11
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.