
Abstract
Background
Robotic liver resection (RLR) for intrahepatic cholangiocarcinoma (ICC) remains a newly adopted approach with limited data supporting its oncologic validity. We aimed to evaluate perioperative outcomes and early oncologic metrics following RLR for ICC at a single hepatobiliary center.
Methods
A retrospective analysis was conducted on patients undergoing RLR for histologically confirmed ICC between January 2018 and December 2024. Data were collected and analyzed using descriptive statistics.
Results
Thirty-five patients underwent RLR for ICC. Mean age was 69 years, with 66% male and a mean ASA grade of III. Major resections comprised 54% of cases, with no conversions to open surgery or intraoperative complications. Mean operative time was 321 years and mean estimated blood loss was 239 mL. R0 resection was achieved in 97% of cases. Mean lymph node harvested was 5, with 37% of patients having ≥6 nodes retrieved. Mean tumor size was 6 cm, with 94% of patients harboring tumors >2 cm and 60% staged as N0. Postoperative complication rate was 34%, with Clavien-Dindo ≥III at 14%. No reoperation occurred. 90-day mortality was 6%. Mean length of stay was 6 days. At a mean follow-up of 21 months, recurrence was observed in 25% of patients, with a mean disease-free survival of 17 months.
Conclusion
Robotic liver resection for ICC is safe and feasible, yielding high rates of R0 resection, low conversion and complication rates, with acceptable oncological outcomes. These findings support the continued integration of robotics in complex liver oncology.
Keywords
Introduction
Intrahepatic cholangiocarcinoma (ICC) is a rare but aggressive primary liver malignancy that originates from the epithelial cells of the bile ducts within the liver. 1 Although uncommon, it is the second most prevalent primary liver cancer. The annual incidence rate of ICC in Western countries in recent years is two cases per 100,000 people. 2 In contrast, certain regions in Southeast Asia report rates of ICC as high as 10 to 71 per 100,000 people annually. 3 Despite this global discrepancy in prevalence, the rates of incidence in Western countries have been rising in recent decades. 2 Curative outcomes and at least prolonged overall survival are possible with complete tumor resection with negative resection margins (R0) together with a porta hepatis lymphadenectomy. 4 However, due to a late onset of symptoms and the cancer’s aggressive biological behavior, a sizable proportion of patients with ICC are not eligible for a curative-intent resection. 5
The optimal surgical approach to treating ICC has varied over the past couple of decades. Traditionally, open surgical resection has been regarded as the cornerstone of curative treatment for ICC. The complex anatomy and location of these tumors pose significant challenges, often resulting in high rates of recurrence and suboptimal long-term outcomes. 6 Recent advancements in minimally invasive techniques to resect ICC tumors have shown promise in overcoming some of these challenges by reducing perioperative morbidity rates and potentially improving oncologic outcomes. Additionally, both laparoscopic and robotic approaches have shown potential to improve perioperative outcomes, such as decreasing hospital length of stay, intraoperative complications, and overall recovery time compared to the open approach. 1 The robotic platform holds several advantages over the laparoscopic platform, including an enhanced range of instrument manipulation, three-dimensional visualization, and improved surgeon dexterity during the operation. 7 Despite these advancements, the long-term outcomes of robotic resection for ICC patients remain inadequately explored at many hepatobiliary institutions.
Due to the significant number of ICC cases seen at our tertiary institution, we therefore use our data to dive deeper into this issue. This study aims to address this gap by retrospectively analyzing perioperative and long-term oncological survival outcomes of patients who underwent RLR of ICC, thereby providing insights into the effectiveness and prognostic factors associated with this technique.
Methods
Study Population
With institutional review board (IRB) approval, 35 patients who underwent robotic hepatectomy for ICC were retrospectively analyzed for perioperative and oncological outcomes between January 2018 and December 2024 at AdventHealth Tampa. All patients are considered for robotic approach unless contraindications are present. Contraindications include obvious involvement of major hepatic veins in the future liver remnant <35%, IVC and Porta Hepatis. Patients who underwent open resections were excluded. Patients who underwent a hepatectomy for other primary and metastatic liver cancers were excluded.
Patient Variables
The preoperative variables collected were split into three categories: Patient factors [age, gender, body mass index (BMI), American Society of Anesthesiology (ASA) class, history of hypertension, diabetes, coronary artery disease (CAD), myocardial infarction (MI), renal failure, and chronic obstructive pulmonary disease (COPD)], liver condition factors [history of previous liver operations, cirrhosis, steatosis, and hepatitis status], and clinical assessment scores [Charlson Comorbidity Index (CCI), Child-Pugh grade, Model of End-Stage Liver Disease (MELD) score, IWATE score, and Tampa difficulty score]. Liver cirrhosis was radiologically detected on preoperative CT scan or MRI and it is then histologically confirmed by a routine intraoperative liver biopsy.
The intraoperative variables examined were operative duration, estimated blood loss (EBL), conversion to open, intraoperative complications, lymph nodes examined, and resection status. Lastly, the postoperative variables analyzed could be separated into two categories: operative outcomes [Clavien-Dindo Score, postoperative complications, length of stay (LOS), follow-up time, 30 and 90-day readmissions, 90-day mortality, 90-day reoperation, tumor recurrence, and disease-free survival] and tumor factors [tumor size, and tumor location]. We used IWATE and TAMPA liver scores to assess the difficulty of each robotic liver operation conducted. The IWATE criteria consider the extent of liver resection, tumor location, tumor size, proximity to a major vessel, HALS/Hybrid, and liver function. TAMPA difficulty score considers the patient’s history of neoadjuvant chemotherapy, tumor location, tumor size, tumor type, extent of parenchymal resection, need for portal lymphadenectomy, and need for extrahepatic biliary resection with hepaticojejunal reconstruction. Lastly, we calculated the long-term oncological survival using Kaplan Myer method to display 5-year disease free survival (DFS) and overall survival (OS).
Statistical Analysis
This study’s data was maintained on Excel spreadsheets. P-values were calculated with an unpaired t-test or two-tailed chi-square analysis. Significance was set at <0.05. Data was presented as mean ± standard deviation. Kaplan Meier survival curve analysis was utilized to measure survival outcomes.
Results
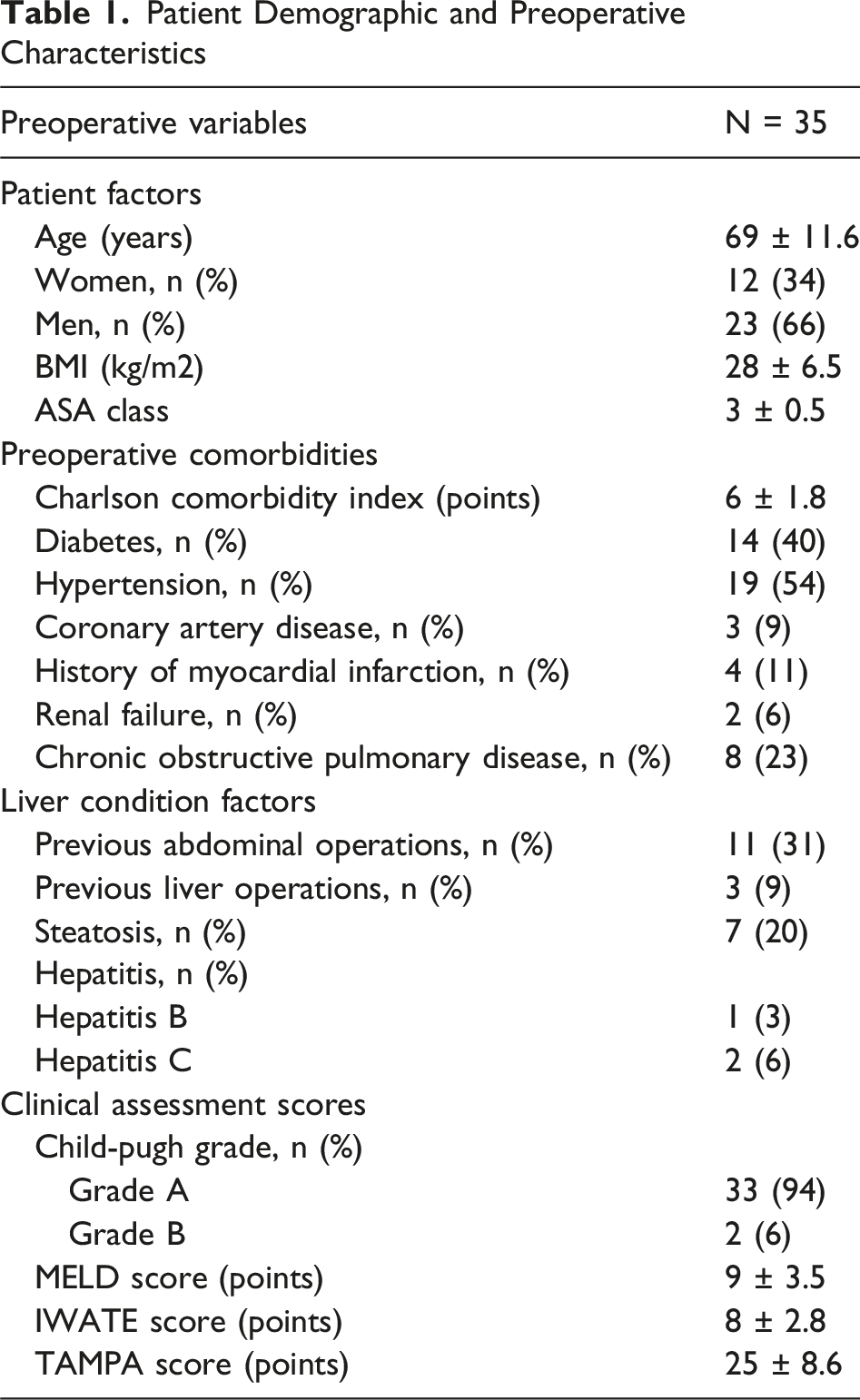
A total of 35 patients underwent robotic liver resection for intrahepatic cholangiocarcinoma. The mean age of the cohort was 69years ±11.6, and the majority were men (66%). The mean body mass index was 28 kg/m2 ± 6.5, and most patients were classified as ASA class III, reflecting at least moderate baseline surgical risk. Patients carried an increased comorbidity burden, with a mean Charlson Comorbidity Index of 6 ± 1.8. Hypertension and diabetes were the most common comorbidities, present in 54% and 40% of patients, respectively. Chronic obstructive pulmonary disease (23%) and prior myocardial infarction (11%) were also notable.
In terms of liver-related history, 31% had prior abdominal operations, and 9% had undergone previous liver resections. Histologic liver abnormalities were frequent, including fibrosis F1-3 (17%), cirrhosis F4 (9%), and steatosis (20%). History of hepatitis C and B infection were infrequently observed, affecting 6% and 3% of patients, respectively. Most patients had preserved liver function, with 94% categorized as Child-Pugh Grade A and only two patients as Grade B. The mean MELD, IWATE, and TAMPA scores were 9 ± 3.5, 8 ± 2.8, and 25 ± 8.6, respectively, indicating moderate surgical complexity.
Tumor characteristics revealed a mean tumor size of 6 cm ± 3.3, with 94% of lesions measuring larger than 2 cm. T-staging showed predominant T2 disease (51%), followed by T1b (23%), T1a (17%), and T3 (9%). Lymph node involvement was documented in 20% of cases (N1), while 60% were node-negative (N0) and 20% had indeterminate nodal status (Nx). No patients had distant metastases at the time of surgery.
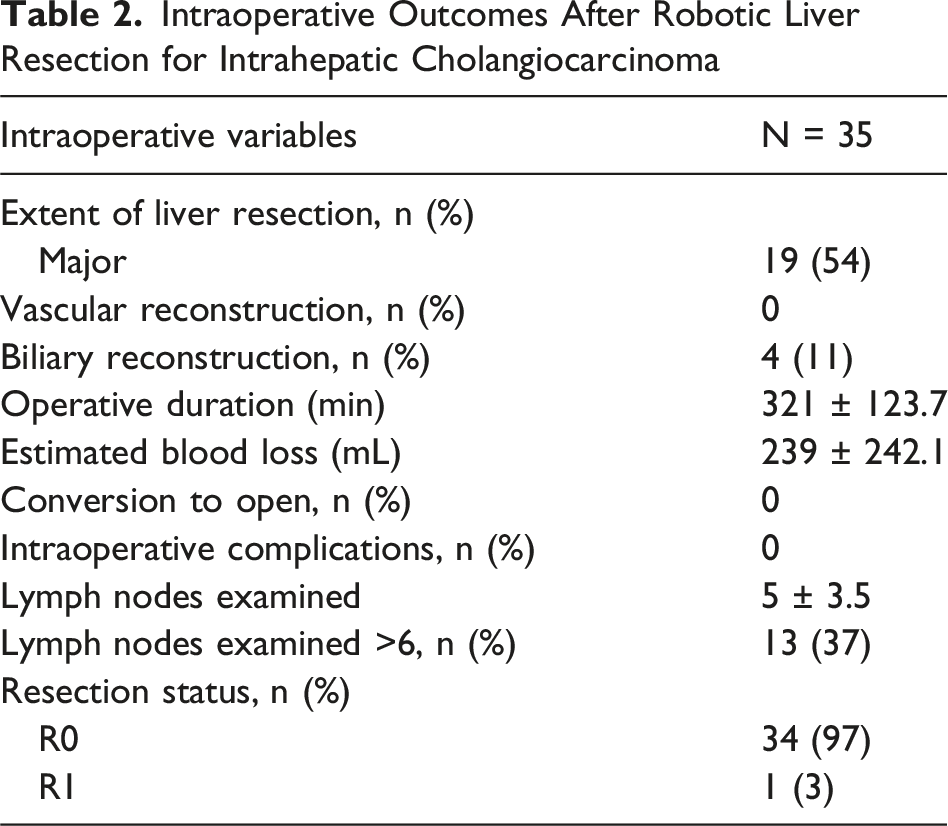
Major liver resections were undertaken in 54% of patients, with an additional 26% classified as technically major. No vascular reconstructions were necessary, and biliary reconstruction was performed in 11% of cases due to proximity with or involvement of the hilar region. The mean operative duration was 321minutes ±123.7 and mean estimated blood loss was 239 mL ± 242.1. There were no intraoperative complications or conversions to open operation. A mean of 5 lymph nodes ±3.5 were examined, with 37% of patients having six or more nodes sampled. R0 resection was achieved in 97% of patients.
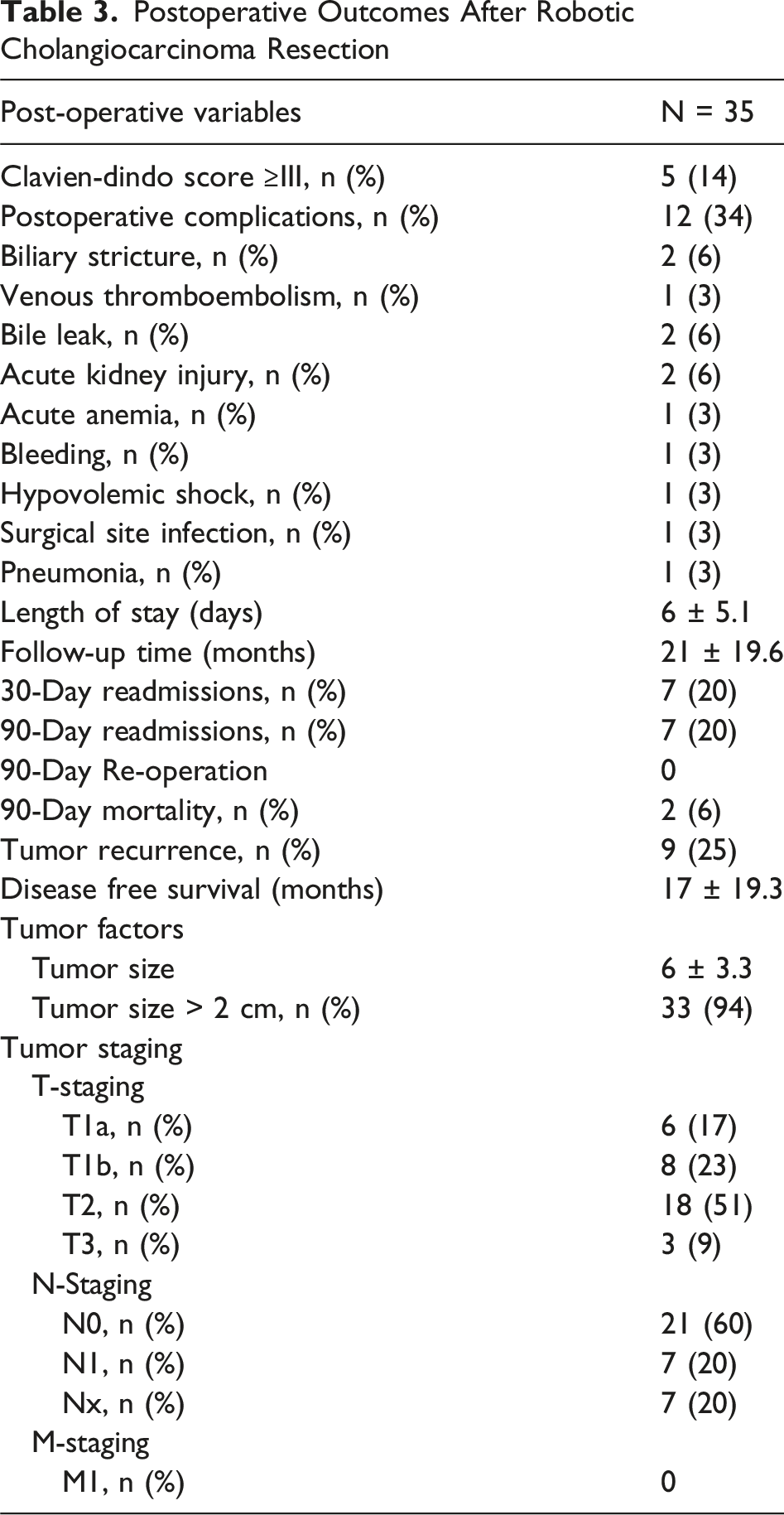
Postoperative complications occurred in 34% of patients, with 14% experiencing Clavien-Dindo grade III or higher complications. Bile leak and venous thromboembolism were the most frequent complications, 6% each, while isolated events of acute kidney injury, anemia, bleeding, hypovolemic shock, pneumonia, and surgical site infection were infrequently observed (Graph 1). No patients required reoperation. The mean hospital length of stay was 6days ±5.1, suggesting rapid recovery in most patients.
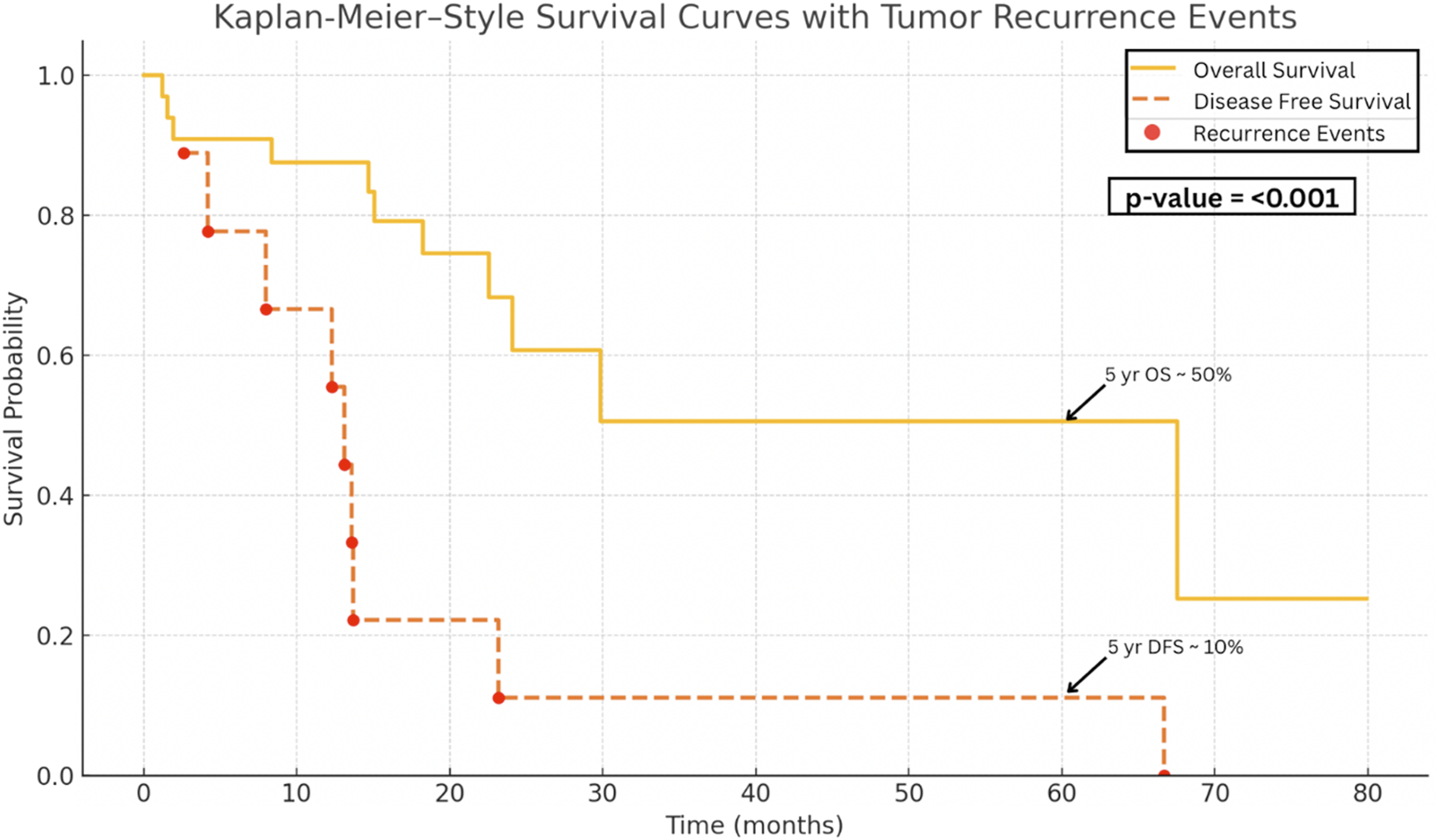
Oncologic follow-up data demonstrated a mean surveillance period of 21months ±19.6. The 30-day and 90-day readmission rates were both 20%, and the 90-day postoperative mortality rate was 6%. Tumor recurrence occurred in 25% of patients, with a mean disease-free survival of 17months ±19.3, highlighting the aggressive biological behavior of intrahepatic cholangiocarcinoma despite optimal surgical management (Graph 1). Kaplan-Meier analysis revealed that the 3-year and 5-year overall survival rate were approximately 50%, whereas the 3-year and 5-year disease-free survival rate were approximately 10%, P-value = <0.001 (Graph 2). Key Outcomes of Robotic Liver Resection for Intrahepatic Cholangiocarcinoma Overall Survival After Robotic Liver Resection for Intrahepatic Cholangiocarcinoma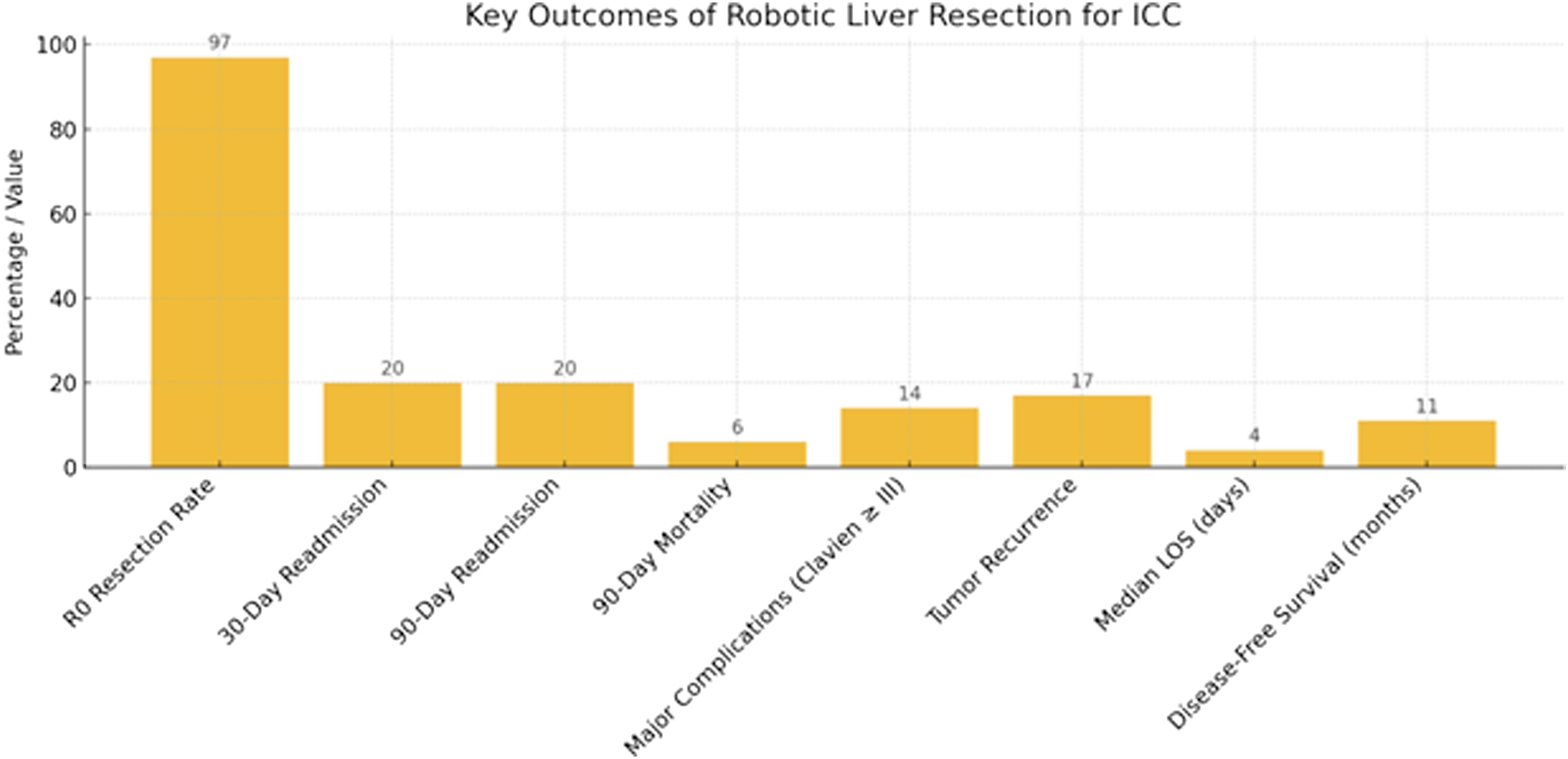
Discussion
Intrahepatic cholangiocarcinoma remains a rare but highly lethal primary liver malignancy with rising incidence. Complete surgical resection continues to be the only potentially curative treatment, although long-term survival remains modest due to high recurrence rates and variability in surgical quality metrics. Our study involving 35 patients undergoing RLR for ICC demonstrates favorable short-term outcomes in a comorbid population, with high R0 resection rates, low conversion, and acceptable complication rates. Comparative analysis with recent literature offers insight into how robotic approaches measure against open and laparoscopic methods across important surgical domains.
Patient Characteristics
Our patient population had a mean age of 69 years and high comorbidity burden (mean ASA of III, Charlson Comorbidity Index of 6), reflecting real-world surgical complexity. Bartsch et al similarly reported that elderly patients (≥70 years) undergoing major liver resection for ICC achieved comparable perioperative and oncologic outcomes to younger patients, supporting surgical intervention in physiologically fit elderly patients when curative resection is possible. 8 Banas et al further emphasized that surgeon experience, particularly after 30-40 liver resections, contributes significantly to reducing operative time, complications, and transfusion rates, a finding that highlights the importance of procedural volume and sub-specialization in hepatobiliary surgery. 9
Liver-Related and Surgical History
In our cohort, chronic liver disease was common, 20% steatosis, 17% F1-3 fibrosis and 9% cirrhosis. Despite these risks, no intraoperative complications or conversions occurred. These findings align with Hamad et al, who analyzed a national cohort and found that RLR resulted in significantly reduced length of stay and equivalent short- and long-term survival compared to open resection in patients with comorbid disease, further supporting the minimally invasive strategy in high-risk patients 1
Tumor Characteristics and Lymphadenectomy
Tumors in our study were predominantly T2 (51%), with 94% > 2 cm and 20% N1. Lymphadenectomy was performed in 80% of our patients, with a mean lymph node yield of 5 and ≥6 nodes achieved in 37%. It is important to note that at least 1/3 of patients in this cohort were operated upon prior to the publication of AJCC 8th edition guidelines, where since radical lymphadenectomy was heavily emphasized. These findings echo the global underutilization of lymphadenectomy as detailed by Lluís et al, who found that despite universal acknowledgment of LND’s staging importance, mean yields remain under AJCC 8th edition’s recommended threshold of six. 10 Krenzien et al and Kim & Park both emphasized the prognostic role of nodal status, suggesting that accurate lymph node staging is essential for guiding adjuvant therapy and for understanding disease prognosis.11,12 Sposito et al reinforced this conclusion in their international surgeon survey, revealing significant variability in LND practices, with only half of respondents consistently retrieving ≥6 nodes. 13 Lauterio et al further noted that although the therapeutic benefit of LND is still debated, its role in staging and multidisciplinary planning is undisputed. 14 Comparatively, Hamad et al demonstrated equivalent lymph node yield (median 4 vs 3.5 nodes) and no difference in nodal evaluation rates between robotic and open surgery. 1 In contrast, the de Hondt meta-analysis reported higher absolute yields with minimally invasive approaches (median 8 vs 7 nodes, P = 0.113), confirming oncologic equivalence. 15 In our experience, robotic platforms facilitated equivalent to the standard nodal evaluation without compromising resection margin quality.
Intraoperative Outcomes
Our mean operative time (321 minutes) and blood loss (239 mL) compare favorably with other robotic series. Shapera et al similarly reported reduced blood loss in robotic resections (100 mL vs 420 mL open), along with higher rates of R0 resection and equivalent lymph node yields. 6 In larger series, Steinkraus et al reported blood loss of 300 mL vs 750 mL (P = 0.001), while de Hondt et al demonstrated a pooled reduction in blood loss of approximately −123 mL with minimally invasive approaches compared to open surgery.15,16 Operative time was comparable, with robotic 173 min vs 219 min (P = 0.072) in Steinkraus et al. 16 Sheng et al highlighted the risks associated with conversion in laparoscopic ICC resection, noting increased operative time, transfusion requirements, and complication rates following unplanned laparoscopic to open conversion, outcomes avoided entirely in our robotic cohort. 17 These findings demonstrate comparable estimated blood loss and operative time in our cohort, highlighting the impact of surgical experience and institutional proficiency in optimizing intraoperative efficiency, even within technically demanding minimally invasive approaches.
Postoperative Outcomes
The overall complication rate in our series was 34%, with 14% experiencing Clavien-Dindo grade III or higher complications (Graph 1). Mean length of stay was 6 days. Specifically, Hamad et al reported a mean LOS of 5.8 vs 8.9 days, for MIS and open cohorts respectively. 1 Similarly, Steinkraus et al demonstrated median LOS of 5 vs 11 days for robotic vs open resections, confirming safety in comorbid populations. 16 This is consistent with our robotic cohort, which demonstrated a similarly reduced LOS, reinforcing the reproducibility of enhanced recovery with minimally invasive approaches. These findings are favorable when compared to benchmark values reported by Alaimo et al, who identified LOS of ≤14 days and major complication rates of ≤14.3% as international surgical quality thresholds in high-volume ICC centers. 2 Comparatively, de Hondt et al reported overall morbidity of 27.4% vs 35.4% and major morbidity of 11.5% vs 15.1% for minimally invasive vs open surgery, respectively. 15 Steinkraus et al reported major morbidity 30.8% vs 48.6%, median CCI of 0 vs 8.7, and complication-free recovery 61.5% vs 37.1%, all favored robotic surgery. 16 Hamad et al reported no difference in readmission (5.6% vs 7.7%) or mortality, reinforcing perioperative safety. 1 Length of stay remains the most consistent advantage, with reported values of 5-6 days (robotic) vs 8-11 days (open) across studies.1,15,16 Our results suggest that robotic resection, in experienced hands, may not only meet but surpass these performance metrics in selected patients.
Oncological Outcomes
With a 97% R0 resection rate, a 25% recurrence rate, and mean disease-free survival of 17 months, our outcomes reflect the aggressive biology of ICC. In comparison, Hamad et al reported R0 rates of 80.6% (robotic) vs 81.6% (open) with no difference, while Steinkraus et al reported 76.6% vs 82.9% (P = 0.28), again demonstrating equivalence.1,16 In contrast, the de Hondt meta-analysis reported higher R0 rates with minimally invasive approaches (90.4% vs 81.4%, OR 1.40), though this may reflect selection bias. 15 Taken together, these findings suggest that in our cohort, even in technically complex ICC cases, robotic resection can achieve greater that benchmarked margin-negative outcomes while maintaining oncologic integrity.
Kaplan-Meier analysis revealed that the 3-year and 5-year overall survival rate was approximately 50%, whereas the 3-year and 5-year disease-free survival rate was approximately 10%. The difference between survival curves was statistically significant, indicating a higher incidence of disease recurrence relative to mortality. According to existing literature, 5-year overall survival for ICC ranges widely between 14% and 49%, depending largely on tumor burden, nodal metastasis, vascular invasion, and margin status. Krenzien et al highlighted that after curative liver resection for ICC, mean survival time was 28-30 months, and 5-year survival was 30%. Whereas disease-free survival was calculated to be about 20 months with survival percentage of less than 5%. Our observed 5-year survival (50%) based on the Kaplan Meier curve (Graph 2) aligns with the upper end of these reported ranges, suggesting favorable surgical outcome despite the aggressive nature of the disease.11,12,14 Hamad et al reported median overall survival was 41 months with no difference between robotic and open approaches (HR 0.71, P = 0.249), while de Hondt et al demonstrated improved DFS with MIS (3-year DFS 49.9% vs 38.5%) but similar recurrence rates (62.8% vs 63.1%).1,15 Wright et al found no survival advantage for resection vs intra-arterial therapy in multifocal ICC, reinforcing the notion that recurrence may be driven more by tumor biology than surgical technique alone. 18 Similarly, Munir et al evaluated textbook oncologic outcomes (TOO) across robotic, laparoscopic, and open approaches, reporting equivalent or superior long-term survival in robotic cases despite lower lymph node yield, particularly when adjuvant therapy was administered. 19
Patrone et al, in a systematic review of minimally invasive ICC surgery, found MIS associated with lower blood loss, shorter LOS, and comparable survival, albeit with lower lymph node yields than open surgery. 20 These findings parallel our own and support the careful expansion of RLR in appropriately selected patients.
Conclusion
Patient Demographic and Preoperative Characteristics
Intraoperative Outcomes After Robotic Liver Resection for Intrahepatic Cholangiocarcinoma
Postoperative Outcomes After Robotic Cholangiocarcinoma Resection
Footnotes
Author Contributions
Conceptualization: Garnet Vanterpool Jr, Sharona B. Ross, Roberta Odorizzi, Henry Zhang, Kristina Milivojev Covilo, Iswanto Sucandy; Methodology: Garnet Vanterpool Jr, Sharona B. Ross, Roberta Odorizzi, Henry Zhang, Kristina Milivojev Covilo, Iswanto Sucandy; Formal analysis and investigation: Garnet Vanterpool Jr, Sharona B. Ross, Roberta Odorizzi, Henry Zhang, Kristina Milivojev Covilo, Iswanto Sucandy; Writing - original draft preparation: Garnet Vanterpool Jr, Sharona B. Ross, Roberta Odorizzi, Henry Zhang, Kristina Milivojev Covilo, Iswanto Sucandy; Writing - review and editing: Garnet Vanterpool Jr, Sharona B. Ross, Roberta Odorizzi, Henry Zhang, Kristina Milivojev Covilo, Iswanto Sucandy; Resources: Garnet Vanterpool Jr, Sharona B. Ross, Roberta Odorizzi, Henry Zhang, Kristina Milivojev Covilo, Iswanto Sucandy; Supervision: Sharona B. Ross, Iswanto Sucandy. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
Garnet Vanterpool Jr, Roberta Odorizzi, Kristina Milivojev Covilo, Henry Zhang, and Iswanto Sucandy have no conflict of interest to disclose. Sharona B. Ross has been a consultant for Intuitive Surgical, Quentus, Medtronic, Caresyntax, Boston Scientific and Johnson & Johnson. She is a part of the advisory board for Intuitive Surgical and has accepted grants from both Medtronic and Intuitive Surgical for her Women in Surgery Career Symposium.