
Abstract
Purpose
This study aimed to provide an updated evaluation of the clinicopathological characteristics and survival outcomes of mammary Paget disease by analyzing pure Paget, Paget + DCIS, and Paget + IDC subgroups within the contemporary SEER cohort, which includes consistent HER2 reporting and reflects the modern systemic therapy era.
Methods
Cases diagnosed in the SEER database between 2010 and 2021 were analyzed. Clinicopathological parameters were compared across subgroups. Overall survival (OS) and cancer-specific survival (CSS) were evaluated using Kaplan-Meier analyses and multivariable Cox regression models.
Results
Paget-associated subgroups exhibited distinct biological profiles, characterized by lower hormone receptor positivity and markedly higher HER2 positivity compared with IDC. In unadjusted analyses, pure Paget and Paget + IDC groups demonstrated lower survival, whereas Paget + DCIS showed the most favorable outcomes (P < 0.001). However, after adjustment for key prognostic determinants, including age, stage, grade, nodal status, and treatment, histological subgroup was not an independent predictor of OS or CSS.
Conclusion
In the modern therapeutic era, survival differences across the Paget spectrum appear to reflect the underlying carcinoma’s biological and clinical characteristics rather than the presence of Paget disease itself. This study represents the most contemporary, comprehensively adjusted population-level analysis to date and clarifies that, when tumors are matched for stage and subtype, Paget disease does not independently worsen prognosis.
Introduction
Mammary Paget disease is a rare subtype of breast cancer and is most commonly associated with ductal carcinoma in situ (DCIS) or invasive ductal carcinoma (IDC).1,2 Clinically, it may present with erythema, scaling, and eczematous changes of the nipple-areolar complex, and it is histopathologically defined by the presence of characteristic Paget cells within the epidermis. Several studies have reported that the biological features of this disease may differ from those of conventional breast cancer types, particularly with respect to parameters such as hormone receptor status and HER2 expression.2-5
The in situ or invasive characteristics of lesions accompanying Paget disease may lead to meaningful differences in clinical course and therapeutic approaches.6,7 However, data remain limited regarding the clinical distribution and survival outcomes of cases in which Paget disease presents with different accompanying components (such as pure Paget, Paget + DCIS, or Paget + IDC) within large populations.4-7 Therefore, comparing the varying clinical forms of Paget disease across broader patient cohorts may contribute to a more comprehensive understanding of the current evidence.
This study aims to characterize the clinicopathological features and survival outcomes of Paget disease and its associated subgroups by examining records from the SEER database between 2010 and 2021. The study period was intentionally restricted to 2010 onward because HER2 receptor status and molecular subtype information were systematically incorporated into SEER beginning that year, enabling accurate subtype-adjusted survival analyses that were not possible in earlier SEER eras. By evaluating four distinct clinical groups (Paget, Paget + DCIS, Paget + IDC, and IDC) and incorporating detailed treatment and biological variables into multivariable models, this study provides an updated and contemporary assessment of whether Paget histology independently influences prognosis in the modern therapeutic era.
Materials and Methods
This study was conducted using data from the Surveillance, Epidemiology, and End Results (SEER) 17 registries research database, which represents approximately 26% of the U.S. population. Female patients diagnosed with breast cancer between 2010 and 2021 were identified using SEER*Stat software. Eligible cases were restricted to those with the following ICD-O-3 morphology codes: 8540/3 (Paget disease, mammary), 8541/3 (Paget disease and infiltrating ductal carcinoma of breast), 8543/3 (Paget disease and intraductal carcinoma), and 8500/3 (infiltrating duct carcinoma, NOS). Patients with other histological subtypes, male breast cancers, cases identified only through autopsy or death certificate, and those with multiple primary tumors were excluded.
Demographic and clinicopathological variables extracted from the database included age at diagnosis, race, marital status, tumor location, laterality, histological grade, estrogen receptor (ER) status, progesterone receptor (PR) status, molecular subtype, T stage, N stage, and AJCC stage. Information on the presence of bone, liver, lung, and brain metastases at diagnosis was also collected. Treatment-related variables included surgical intervention, radiotherapy, chemotherapy, and systemic therapy.
Statistical Analyses
All statistical analyses were performed using R software (version 4.5.2; R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were used to summarize baseline clinicopathological characteristics of the four study groups (Paget, Paget + DCIS, Paget + IDC, and IDC). Categorical variables were compared using the chi-square test, and continuous variables were summarized as medians with interquartile ranges.
Overall survival (OS) and cancer-specific survival (CSS) were evaluated using the Kaplan-Meier method. Survival curves were compared using the log-rank test, and median survival times with 95% confidence intervals were obtained directly from Kaplan-Meier estimates. CSS was defined as death attributed to breast cancer, with non-breast cancer deaths censored at the date of death.
To examine the association between clinicopathological variables and survival outcomes, univariate Cox proportional hazards regression models were first constructed. All variables with clinical relevance or statistical significance in univariate analyses were entered into multivariable Cox proportional hazards models to determine independent predictors of OS and CSS. Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported. Proportional hazards assumptions were assessed using Schoenfeld residuals.
Multivariable models included age, marital status, race, tumor grade, T stage, N stage, AJCC stage, molecular subtype (HR/HER2-defined), type of surgery, radiotherapy, chemotherapy, and systemic therapy. For the primary exposure, Paget was used as the reference group, and hazard ratios were estimated for Paget + IDC, Paget + DCIS, and IDC.
Pairwise survival comparisons between the four groups were conducted using adjusted P-values to account for multiple comparisons. Forest plots summarizing multivariable HR estimates and 95% CIs were generated using the ggplot2 package. Kaplan-Meier curves were constructed with shaded confidence intervals and number-at-risk tables. Flow diagrams were created using the Diagramme R package. A two-tailed P-value <0.05 was considered statistically significant.
Results
Cohort and Baseline Characteristics
A total of 406,389 women met the inclusion criteria: Paget (n = 213), Paget + IDC (n = 758), Paget + DCIS (n = 431), and IDC (n = 404,987) (Figure 1). Study cohort selection flowchart. Flow diagram showing the identification of eligible patients with pure Paget disease, Paget + DCIS, Paget + IDC, and invasive ductal carcinoma (IDC) from the SEER 2010-2021 database after application of exclusion criteria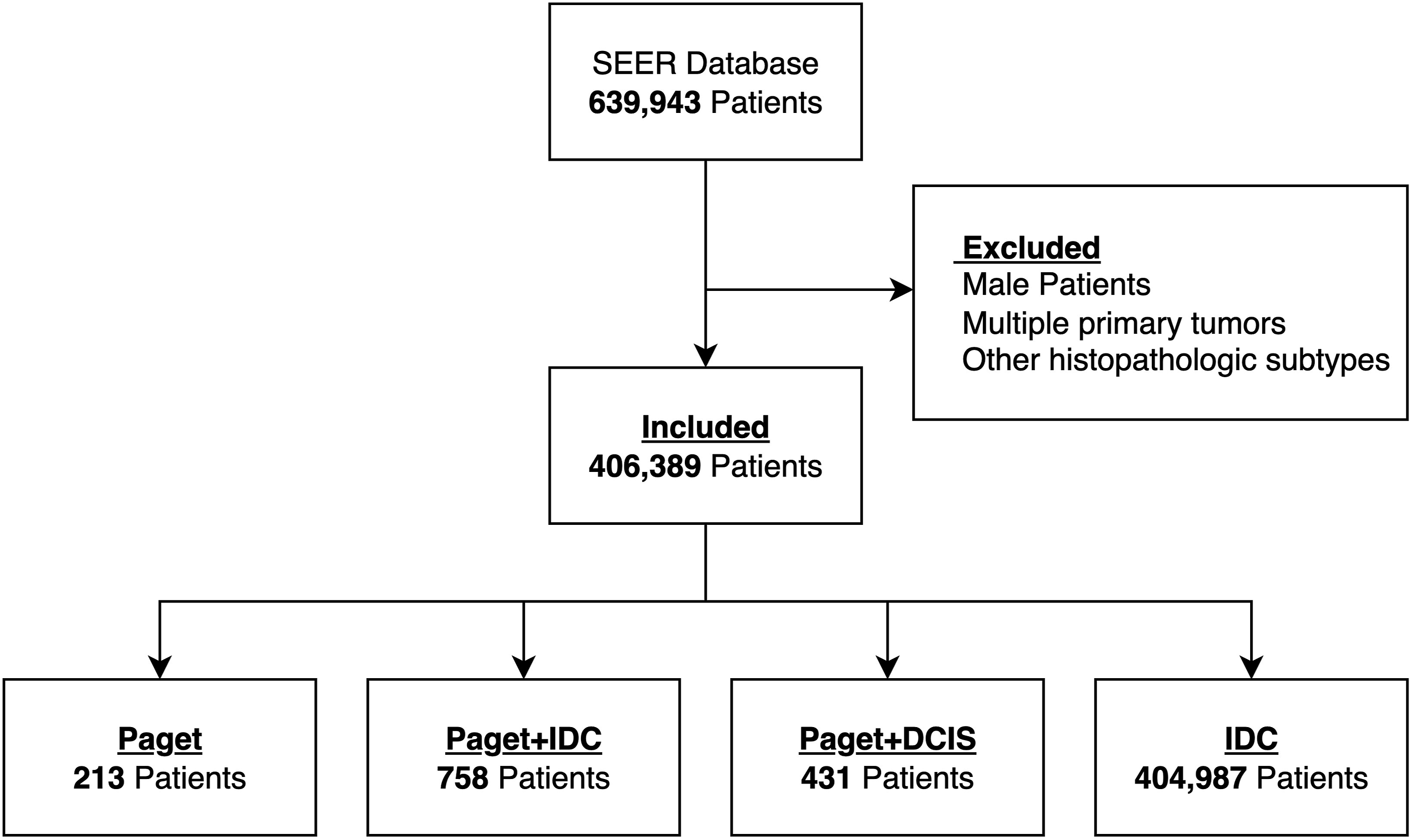
Baseline Characteristics
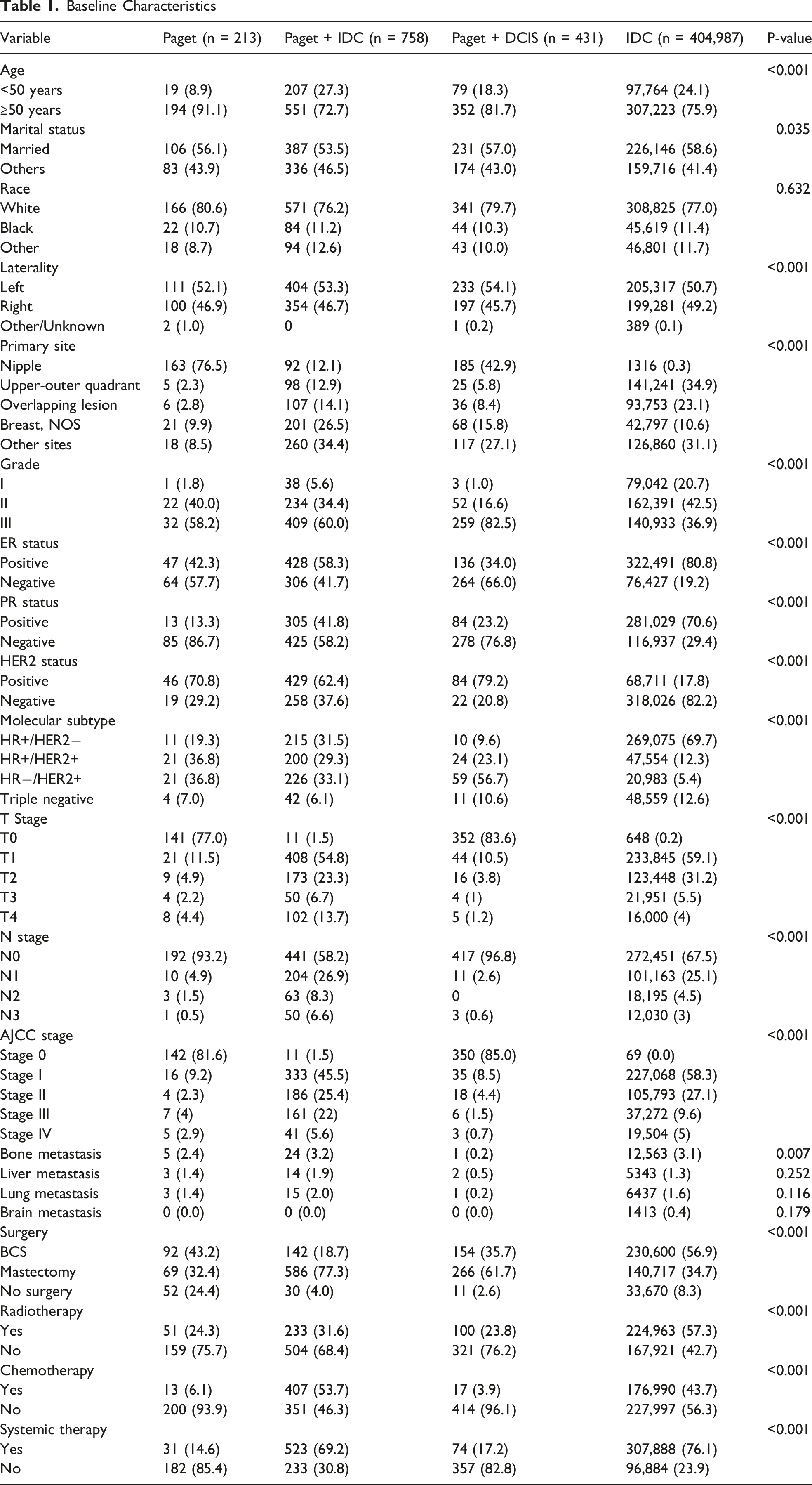
Histologic differentiation also varied across groups (P < 0.001). Grade III tumors were more frequent in Paget (58.2%) and Paget + IDC (60.0%), and were most common in Paget + DCIS (82.5%), compared with 36.9% in IDC. Molecular subtype distributions showed marked heterogeneity (P < 0.001): HR+/HER2− disease predominated in IDC (69.7%), whereas HR−/HER2 + tumors were relatively enriched in Paget + DCIS (56.7%).
Tumor burden at diagnosis reflected these differences. Paget and Paget + DCIS commonly presented with in situ disease (T0: 77.0% and 83.6%, respectively), while Paget + IDC and IDC were more often invasive (T1: 54.8% and 59.1%; P < 0.001). Nodal negativity was most frequent in Paget and Paget + DCIS (N0: 93.2% and 96.8%), and less common in Paget + IDC (58.2%) and IDC (67.5%; P < 0.001). Consequently, stage 0 disease predominated in Paget (81.6%) and Paget + DCIS (85.0%), whereas stage I was the most frequent stage in IDC (58.3%) and Paget + IDC (45.5%; P < 0.001).
Distant metastasis at diagnosis was uncommon in all groups. Bone metastasis ranged from 0.2% in Paget + DCIS to 3.2% in Paget + IDC (P = 0.007), while liver, lung, and brain metastases were each observed in ≤2% of patients, without significant between-group differences (all P > 0.05).
Treatments
Patterns of local and systemic treatment differed substantially according to histologic group (Table 1). Breast-conserving surgery (BCS) was most frequently performed in IDC (56.9%), whereas mastectomy was the predominant procedure in Paget + IDC (77.3%) and Paget + DCIS (61.7%; P < 0.001). Notably, 24.4% of Paget patients did not undergo surgery, a proportion considerably higher than in the other groups.
Use of adjuvant therapies also varied (all P < 0.001). Radiotherapy was administered to 57.3% of IDC patients but to only 24.3% of Paget cases. Chemotherapy was most common in Paget + IDC (53.7%) and less frequent in Paget (6.1%) and Paget + DCIS (3.9%). Systemic therapy (including endocrine and targeted treatments) was recorded in 76.1% of IDC cases, compared with 69.2% of Paget + IDC, 17.2% of Paget + DCIS, and 14.6% of Paget patients.
Survival Outcomes
Kaplan-Meier analyses revealed distinct overall survival (OS) patterns among the four groups (Figure 2). With 19 observations excluded due to missing data, the estimated 5-year OS rates were: • Paget: 76.1% • Paget + IDC: 78.0% • Paget + DCIS: 87.4% • IDC: 85.4% Kaplan-Meier overall survival (OS) curves by subgroup. Overall survival probabilities for pure Paget, Paget + DCIS, Paget + IDC, and IDC groups. The global log-rank P-value is displayed on the plot., with Paget + DCIS demonstrating the most favorable OS
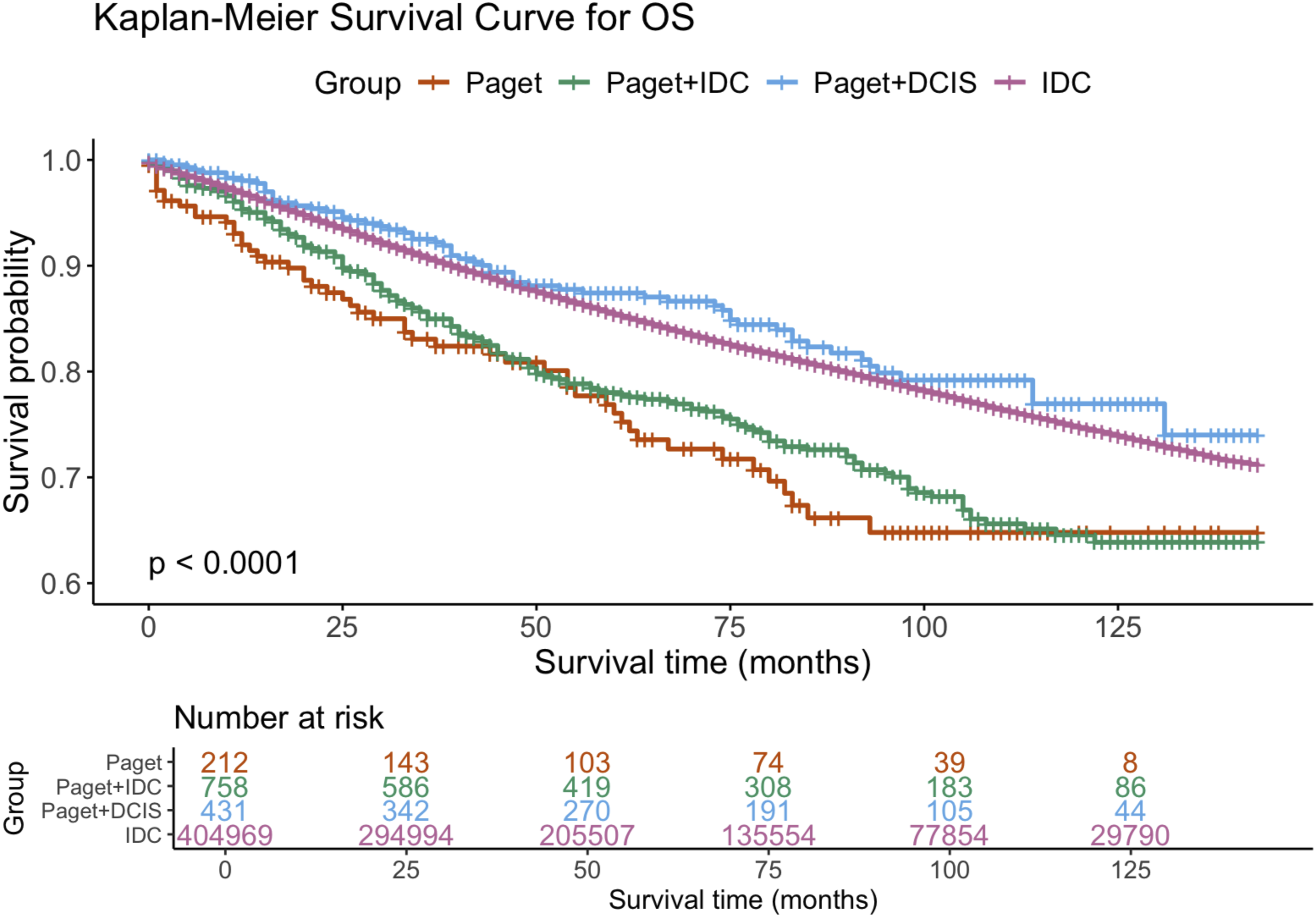
At 10 years, OS was 64.8% for Paget, 64.6% for Paget + IDC, 77.0% for Paget + DCIS, and 74.7% for IDC. The global log-rank test for OS was highly significant (P < 0.0001). Pairwise comparisons showed that OS in Paget + DCIS was superior to that in Paget, Paget + IDC, and IDC (all P < 0.001), whereas Paget and Paget + IDC did not differ significantly from each other (P = 0.392). Paget and IDC showed comparable crude OS (P < 0.001 in favor of IDC, but curves were closely overlapping in later follow-up).
For cancer-specific survival (CSS), Kaplan-Meier curves demonstrated a similar pattern (Figure 3). Paget + DCIS again exhibited the most favorable breast cancer–specific outcomes, while Paget + IDC and IDC showed intermediate survival and Paget the lowest unadjusted CSS. Overall and pairwise log-rank tests confirmed significant differences between Paget + DCIS and each of the other groups (all P < 0.001), whereas the difference between Paget and IDC was not statistically significant (P = 0.561). Kaplan-Meier cancer-specific survival (CSS) curves by subgroup. Cancer-specific survival outcomes across the four groups. Paget + DCIS shows the highest CSS, while Paget and Paget + IDC demonstrate lower unadjusted CSS compared with IDC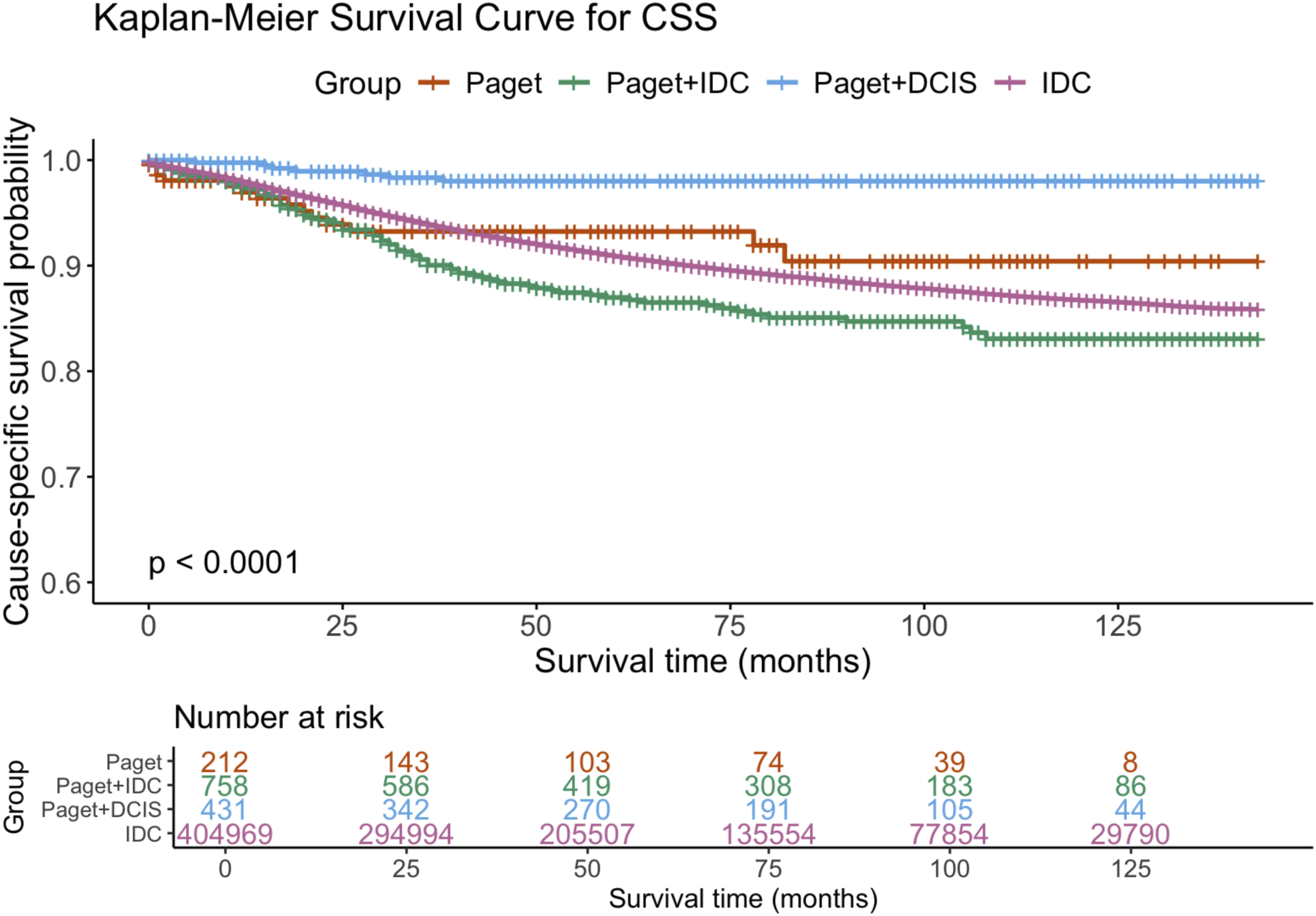
Multivariable Analysis for Overall Survival
In the multivariable Cox regression model adjusting for demographic, tumor-related, and treatment variables (Figure 4, Tables 2 and 3), histologic group was not independently associated with OS when Paget was used as the reference category: • Paget + IDC: HR 0.70, 95% CI 0.33-1.51, P = 0.364 • Paget + DCIS: HR 0.57, 95% CI 0.23-1.43, P = 0.232 • IDC: HR 0.61, 95% CI 0.29-1.28, P = 0.187 Multivariate Cox regression model for overall survival (OS). Forest plot of adjusted hazard ratios (HRs) for OS, including Paget subgroups, demographic factors, tumor stage, grade, nodal status, molecular subtypes, surgical treatment, radiotherapy, systemic therapy, and chemotherapy Univariate and Multivariate Cox Regression Analysis for Overall Survival (OS) Univariate and Multivariate Cox Regression Analysis for Cancer-specific Survival (CSS)
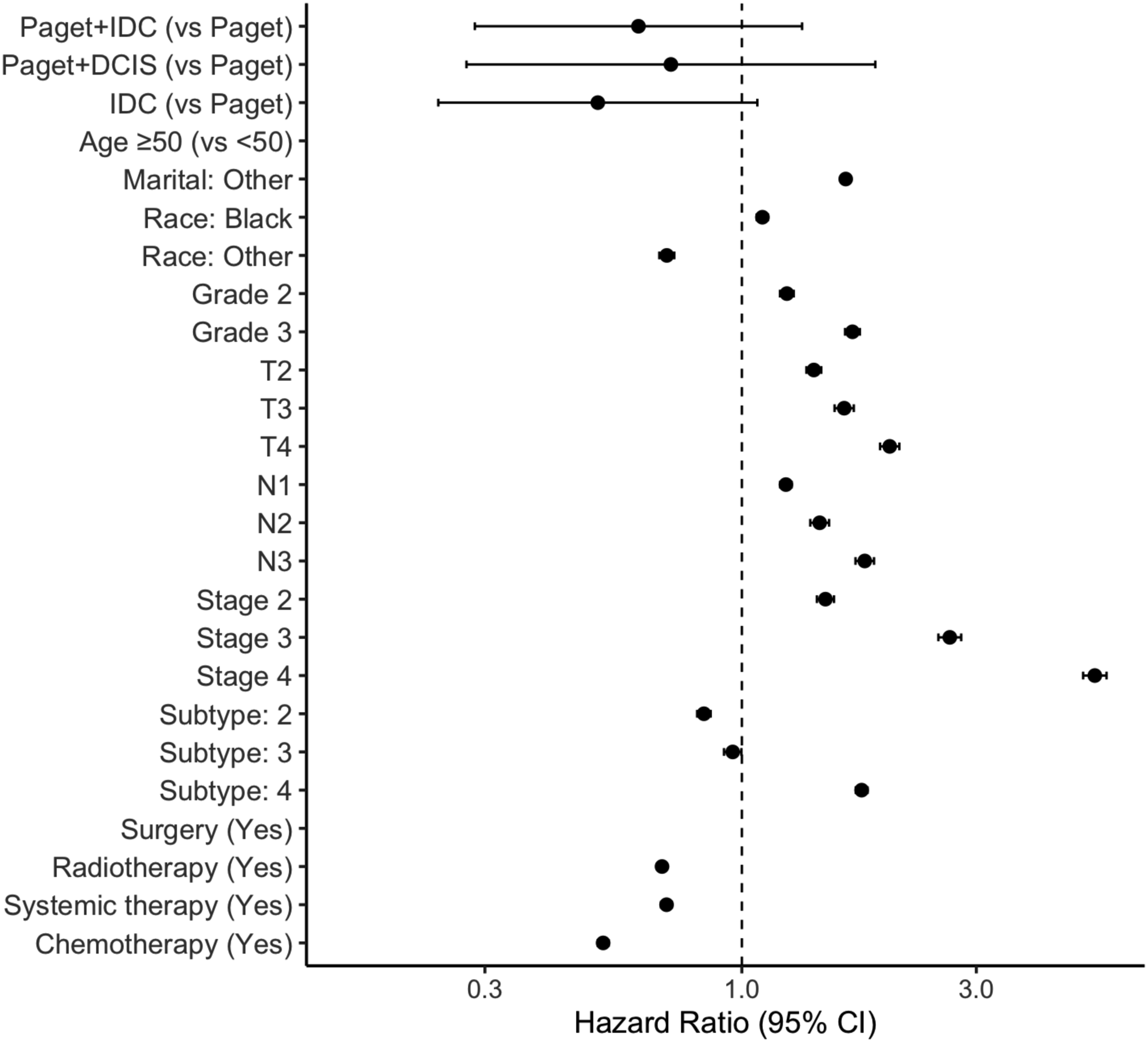
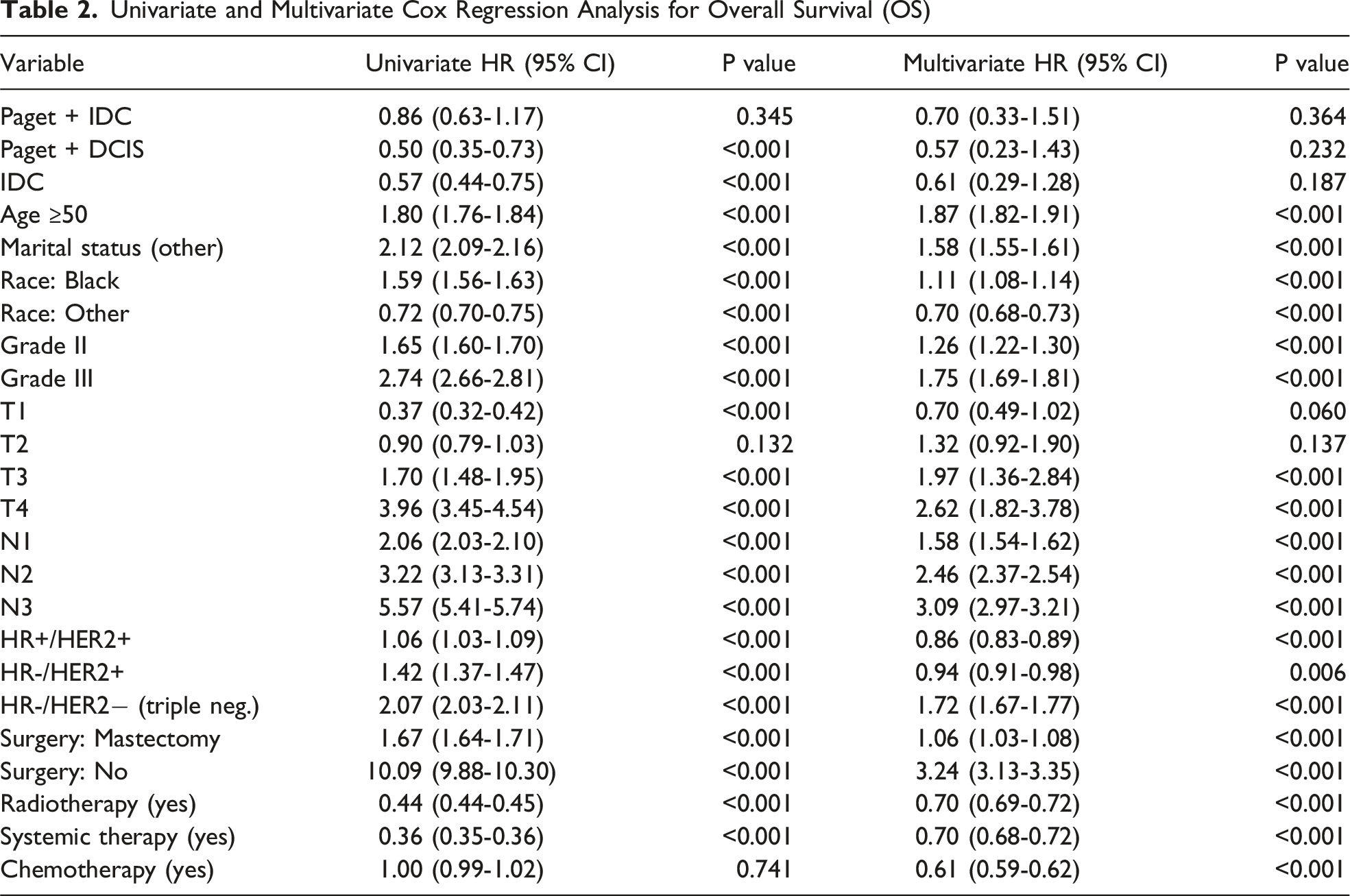
In contrast, several established prognostic factors retained strong associations with OS. Age ≥50 years (HR 1.87, 95% CI 1.82-1.91), unmarried status (HR 1.58, 95% CI 1.55-1.61), Black race (HR 1.11, 95% CI 1.08-1.14), higher histologic grade (grade II HR 1.26; grade III HR 1.75; both P < 0.001), and advanced T and N stages were all linked to worse OS. Regarding molecular subtype, triple-negative disease (HR−/HER2−) conferred the highest risk (HR 1.72, 95% CI 1.67-1.77).
Treatment variables also showed expected effects. Compared with BCS, mastectomy was associated with a modestly higher risk of death (HR 1.06, 95% CI 1.03-1.08, P < 0.001), while no surgery carried a markedly increased risk (HR 3.24, 95% CI 3.13-3.35, P < 0.001). Radiotherapy and systemic therapy were independently associated with improved OS (HR 0.70 and 0.70, respectively; both P < 0.001), and chemotherapy was also protective after adjustment (HR 0.61, 95% CI 0.59-0.62, P < 0.001).
Multivariable Analysis for Cancer-specific Survival
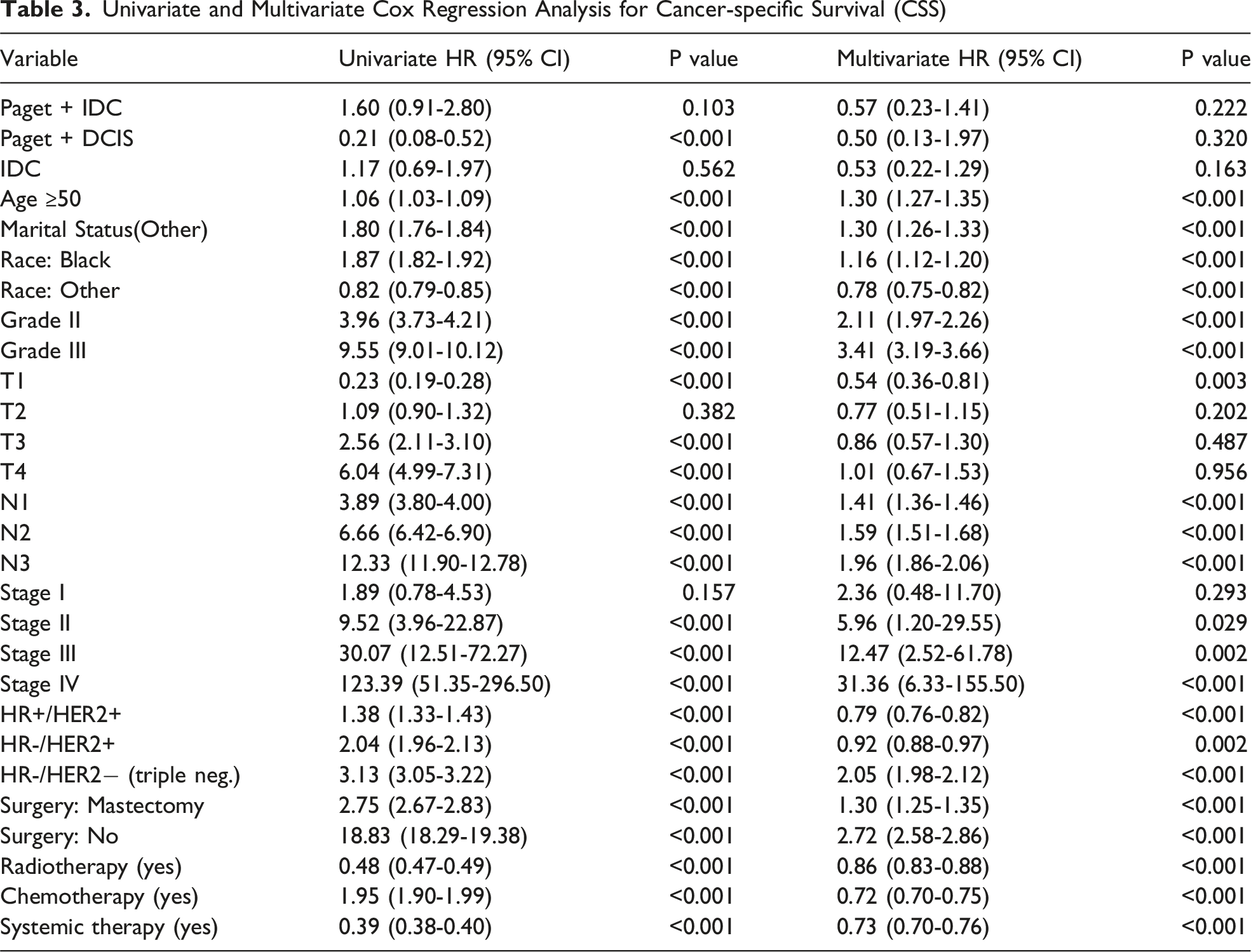
Findings for CSS mirrored those for OS (Figure 5, Table 3). After multivariable adjustment, histologic group again was not an independent predictor of breast cancer–specific mortality relative to Paget: • Paget + IDC: HR 0.57, 95% CI 0.23-1.41, P = 0.222 • Paget + DCIS: HR 0.50, 95% CI 0.13-1.97, P = 0.320 • IDC: HR 0.53, 95% CI 0.22-1.29, P = 0.163 Multivariate Cox regression model for cancer-specific survival (CSS)
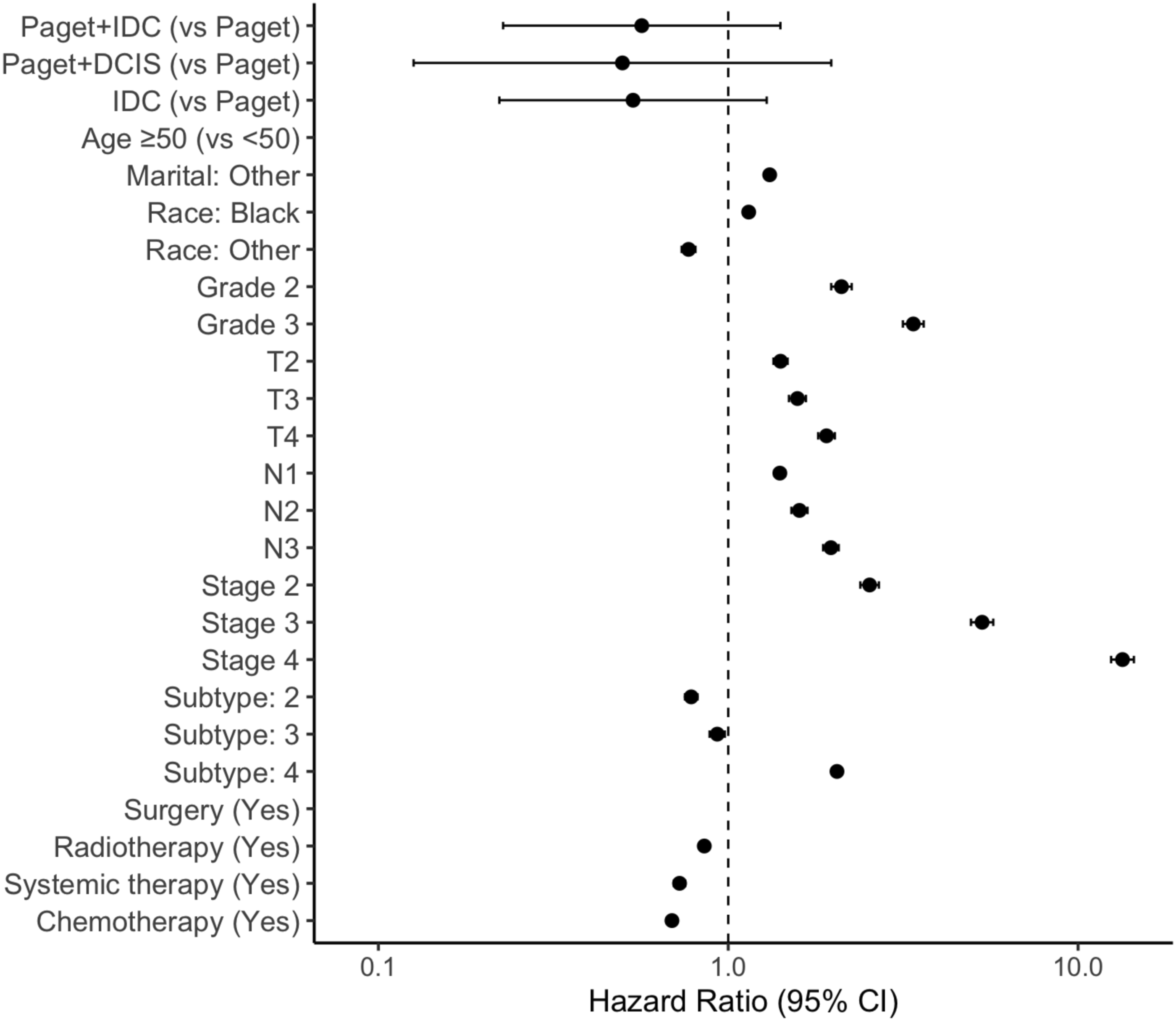
Instead, CSS was primarily driven by tumor burden and biology. Higher grade (grade II HR 2.11; grade III HR 3.41; both P < 0.001), advanced nodal stage (N1-N3; all P < 0.001), and increasing AJCC stage were strongly associated with cancer-specific mortality (stage II HR 5.96, stage III HR 12.47, stage IV HR 31.36 vs stage 0; all P ≤ 0.029). Molecular subtype again showed a gradient of risk, with the poorest CSS in triple-negative tumors (HR 2.05, 95% CI 1.98-2.12).
Regarding treatment, absence of surgery remained a powerful adverse factor (HR 2.72, 95% CI 2.58-2.86, P < 0.001). Radiotherapy, chemotherapy, and systemic therapy were each associated with improved CSS (HR 0.86, 0.72, and 0.73, respectively; all P < 0.001).
Taken together, these results indicate that although Paget-associated tumors display distinct clinicopathologic and molecular characteristics and show crude survival differences, histologic group per se does not independently influence overall or cancer-specific survival once stage, tumor biology, and treatment are taken into account.
Discussion
This study represents one of the most up-to-date analyses evaluating the clinicopathological features and survival outcomes of Paget disease and its associated carcinomas within a large SEER cohort covering the years 2010-2021. The systematic comparison of four distinct histological subgroups (pure Paget, Paget + DCIS, Paget + IDC, and IDC) provides a comprehensive perspective on the clinical spectrum of Paget disease. Overall, our findings suggest that the Paget spectrum differs biologically and clinically from conventional invasive ductal carcinoma, yet these differences do not appear to have an independent impact on survival outcomes.
Unlike earlier SEER-based reports, our analysis evaluates Paget disease within a modern therapeutic and diagnostic era. HER2 data became consistently available only after 2010, and prior studies were unable to fully adjust for molecular subtype or treatment variables such as systemic therapy. By integrating these parameters into multivariable models, our study offers a more precise interpretation of whether Paget histology independently affects survival. The contemporary timeframe, combined with a four-group analytic structure, allows clearer differentiation of the prognostic contribution of Paget disease vs the underlying carcinoma component.
From a clinical perspective, our findings indicate that Paget disease should be interpreted within the context of the underlying carcinoma rather than as an independent prognostic entity. When stage, nodal status, grade, and molecular subtype are considered, the presence of Paget changes does not confer additional survival risk. Accordingly, treatment decisions should be guided by the biological and anatomical characteristics of the associated DCIS or IDC, rather than by Paget histology alone. This distinction clarifies that Paget disease represents a phenotypic manifestation of the underlying tumor, and that management should follow established principles based on tumor burden and molecular phenotype. By separating histologic phenotype from tumor biology, our study refines the prognostic interpretation of Paget disease for contemporary clinical practice.
In our study, cases associated with Paget disease demonstrated markedly lower hormone receptor positivity and significantly higher HER2 positivity. This pattern is consistent with the HER2-dominant phenotype previously described for Paget disease.33,4,7 Caliskan et al reported HER2 positivity rates as high as 88% in Paget patients, 8 and similarly, Zhao et al (2018) and Wang et al (2018) showed predominant hormone receptor negativity and HER2 positivity.4,9 The notably high proportion of HR−/HER2 + tumors particularly in the Paget + DCIS subgroup suggests that this subtype may exhibit a biologically distinct behavior. 5 In contrast, the Paget + IDC subgroup demonstrated a more heterogeneous molecular distribution, consistent with the findings of Wu et al (2017), who reported higher grade, more advanced stage, and prominent HER2 positivity in the PD-IDC subgroup. In this context, our study reinforces these biological trends within a larger population. 10
In the survival analyses, notable differences were observed across the groups; specifically, the Paget + DCIS subgroup demonstrated superior overall survival and cancer-specific survival. In contrast, the pure Paget and Paget + IDC groups exhibited lower survival in unadjusted analyses. This suggests that the observed survival differences in crude comparisons may stem not from Paget disease itself but rather from unfavorable tumor characteristics that more commonly accompany Paget disease, such as more advanced stage, higher grade, HER2 positivity, and nodal involvement. The poorer survival observed in pure Paget cases compared with the Paget + DCIS group may also be attributable to factors such as older age, delayed diagnosis, and a higher frequency of adverse prognostic tumor features, rather than an intrinsic biological effect of Paget disease.
Similarly, in the SEER analysis conducted by Zhao et al (2018), the Paget + DCIS subgroup demonstrated the most favorable survival, whereas the Paget + IDC subgroup showed the poorest outcomes. 4 Although some earlier studies interpreted these crude differences as evidence of a “poor prognostic effect” attributable to Paget disease itself, the limited availability of HER2 data and the omission of treatment variables in Zhao et al.’s model made it difficult to clarify any independent effect.4-9 In contrast, in our study, once strong prognostic factors, including age, stage, histological grade, nodal involvement, and treatment modalities, were incorporated into the multivariable models, histological subgroup did not emerge as an independent predictor of survival.
Wang et al likewise demonstrated that tumor stage, axillary lymph node metastasis, HER2 positivity, and distant metastasis were associated with poorer survival in Paget cases, emphasizing that the prognosis of Paget disease is primarily determined by the underlying tumor burden and biological characteristics. 9 These findings align with our results, in which histological subgroup was not identified as an independent prognostic factor in multivariable analyses. Wu et al (2017) also reported that in the PD-IDC subgroup, histological type was not an independent prognostic variable in multivariable models; instead, the principal determinants of survival were stage, HER2 status, and nodal involvement. 10
In the large Chinese cohort reported by Han et al, Paget disease was identified as an independent adverse prognostic factor for disease-free survival when evaluated together with underlying IDC/DCIS. 11 In contrast, in our SEER-based analysis, once age, stage, histological grade, nodal involvement, and treatment variables were comprehensively incorporated into the model, no independent difference in overall or cancer-specific survival was observed between the Paget spectrum and conventional IDC. When these findings are considered collectively, it appears likely that the association between Paget disease and poor prognosis reported in some series may be at least partly attributable to incomplete adjustment for coexisting factors such as tumor burden, biological subtype, and treatment differences.
Paget disease may be considered a phenotypic manifestation that tends to occur alongside tumors with more unfavorable clinicopathological characteristics, rather than an independent biological factor determining the behavior of breast cancer. However, when two tumors of the same stage, grade, nodal status, and comparable biological features are compared, the presence of Paget disease does not adversely affect survival, nor do patients with Paget disease experience a worse clinical course.
These findings may contribute to a more integrated interpretation of the survival patterns reported for Paget disease in the literature. For example, in the SEER analysis by Bae et al, lower cancer-specific survival was noted in the Paget + IDC subgroup, particularly within the HR+/HER2− subtype. 7 Natural variations across studies, such as patient selection, subgroup definitions, follow-up periods, and analytical approaches, can lead to heterogeneity in the reported results. In the present study, the evaluation of the Paget spectrum within a large, contemporary data set, while accounting for key determinants such as tumor stage, histological grade, biological subtype, and treatment modalities, enabled a more comprehensive interpretation of the findings. In this context, it appears that when appropriate treatment is provided, the presence of Paget disease does not independently worsen survival.
However, this study has certain limitations that should be taken into consideration when interpreting the results. The SEER database lacks several important variables, including detailed information on endocrine therapy, HER2-targeted treatments, and other systemic therapeutic modalities. In addition, because data on recurrence and disease progression are not available, the survival outcomes may not fully reflect the biological course of the disease. The retrospective design also inherently carries a risk of selection bias. Nevertheless, the large sample size and the use of comprehensive multivariable analyses enhance the reliability of the findings. In addition, SEER lacks important clinical variables that may influence outcomes. Smoking history is not captured, and because smoking is associated with both overall health and certain breast cancer characteristics, the absence of this information may introduce unmeasured confounding when comparing subgroups. SEER also does not provide data on locoregional recurrence or disease-free survival, preventing assessment of whether patterns of relapse differ across the Paget spectrum. Another limitation is the potential for misclassification of Paget disease, DCIS, and IDC, as SEER coding is derived from registry-level abstraction of pathology reports rather than standardized central review; discrepancies between clinical and pathological characterization cannot be excluded. Additionally, SEER contains limited information on patient comorbidities, which may affect both treatment selection and overall survival and could contribute to residual confounding in adjusted models. Although these limitations are inherent to population-based registry analyses, they do not materially alter the main conclusion that survival differences are primarily driven by underlying tumor biology rather than Paget histology itself.
Overall, the high rate of HER2 positivity and the relatively low rate of hormone receptor positivity observed in carcinomas associated with Paget disease represent a biologically noteworthy distinction. However, this biological difference does not appear to translate into an independent prognostic impact when appropriate surgical and systemic treatment strategies are applied. Therefore, in the clinical management of Paget disease, individualized treatment plans that focus on the characteristics of the accompanying in situ or invasive component, disease stage, and biological subtype are likely to be more decisive. 12
An additional conceptual limitation concerns the definition of “pure Paget disease.” It has been argued that truly isolated Paget disease without underlying carcinoma may be uncommon, and that some cases categorized as pure Paget at presentation may in fact harbor occult in situ or invasive carcinoma that is not detected at initial evaluation. In such cases, Paget disease may represent a clinical manifestation of an undetected primary lesion rather than a biologically distinct entity. Because SEER classification is based on registry coding at the time of diagnosis, we were unable to determine whether additional carcinoma components were identified later during follow-up. Therefore, our categorization reflects presentation-based histology rather than definitive biological separation, and survival differences in the pure Paget group should be interpreted with this consideration in mind.
Conclusion
This study provides the most contemporary, comprehensively adjusted, population-level analysis of Paget disease heterogeneity to date. By leveraging the 2010-2021 SEER era, with consistent HER2 reporting and widespread adoption of modern systemic therapies, our findings refine earlier observations from prior SEER and institutional studies. Specifically, by separately evaluating pure Paget, Paget + DCIS, and Paget + IDC in comparison with IDC, and by adjusting for stage, molecular subtype, nodal burden, and treatment patterns, we demonstrate that Paget histology itself does not confer an independent prognostic disadvantage. Instead, survival differences across the Paget spectrum are largely explained by the characteristics of the underlying carcinoma and the distribution of biological subtypes. These results clarify the prognostic interpretation of Paget disease in contemporary practice and underscore the importance of individualized management based on tumor biology and stage rather than the presence of Paget changes alone.
Footnotes
Ethical Considerations
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study utilized de-identified data from the SEER database, which is publicly available and maintains patient anonymity, ethical approval and informed consent were not required.
Author Contributions
B.T.: Project administration, Critical review, Writing – original draft, Writing – review & editing.
A.N.S.: Conceptualization, Methodology, Data curation, Software, Formal analysis, Visualization.
A.K: Formal analysis, Critical review, Data curation.
D.E.T.S.: Supervision, Validation, Visualization, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.