
Abstract
Gallbladder volvulus, or “floating gallbladder,” is a rare but serious and potentially life-threatening condition that is frequently overlooked for more common biliary pathologies. Preoperative diagnosis can be challenging given a similar clinical presentation to the more common acute cholecystitis, and a high index of suspicion for gallbladder volvulus is required for prompt diagnosis. Unlike cholecystitis, patients with gallbladder volvulus cannot and should not be managed nonoperatively, and failure of conservative therapy in suspected cholecystitis should prompt consideration for an unconventional diagnosis such as torsion. Timely surgical treatment avoids the complications and morbidity of delayed cholecystectomy and leads to overall improved patient outcomes. We report a case of gallbladder volvulus in an elderly patient presenting with signs and symptoms mimicking acute cholecystitis. The patient was admitted for laparoscopy and intraoperatively found to have twisting of the cystic pedicle causing gallbladder ischemia. Given the increased incidence of gallbladder volvulus in the geriatric population, the more liberal use of alternative imaging modalities such as magnetic resonance cholangiopancreatography (MRCP) may be warranted moving forward. Importantly, early surgical intervention is key to successful management of gallbladder volvulus.
Background
Gallbladder volvulus (GV) is a rare but potentially life-threatening condition that often mimics acute cholecystitis (ACC). First described by Wendel in 1898 as a “floating gallbladder,” 1 the exact mechanism of why such torsion occurs remains unclear. Several theories have been proposed, the most widely accepted of which is that an elongated gallbladder mesentery, either congenital or due to physiologic changes with aging resulting in loss of visceral fat and fibrous connective tissue. 2 Review of existing literature reveals only approximately 500 documented cases. 3 The preoperative diagnosis of GV remains challenging but crucial to appropriate surgical management. We report a case of GV in a geriatric patient presenting with signs and symptoms mimicking acute cholecystitis who was intraoperatively found to have gallbladder necrosis secondary to volvulus.
Case Report
An 87-year-old Caucasian woman presented to the emergency room with a one-day history of right upper quadrant (RUQ) abdominal pain after eating. She had no significant past medical or surgical history and denied associated nausea or systemic signs of infection. Physical exam revealed a soft, nondistended abdomen with moderate right upper quadrant tenderness to palpation. She was hemodynamically normal with no leukocytosis or LFT abnormalities on initial labs. Abdominal ultrasound (US) and computed tomography (CT) imaging demonstrated distended gallbladder with wall thickening and edema concerning for acute cholecystitis (Figure 1). She was admitted to the surgical service and taken to the operating room for laparoscopic cholecystectomy the next day.
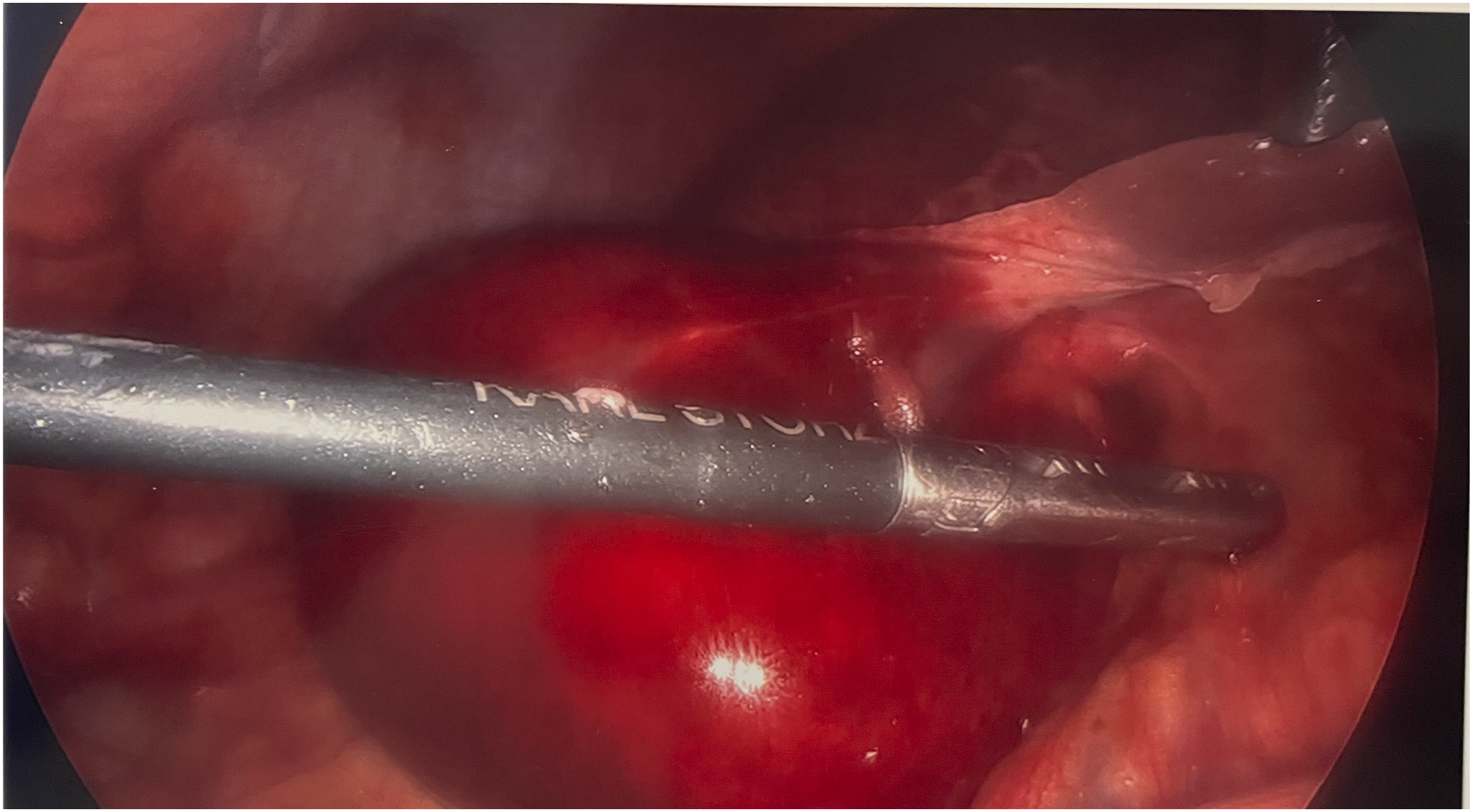
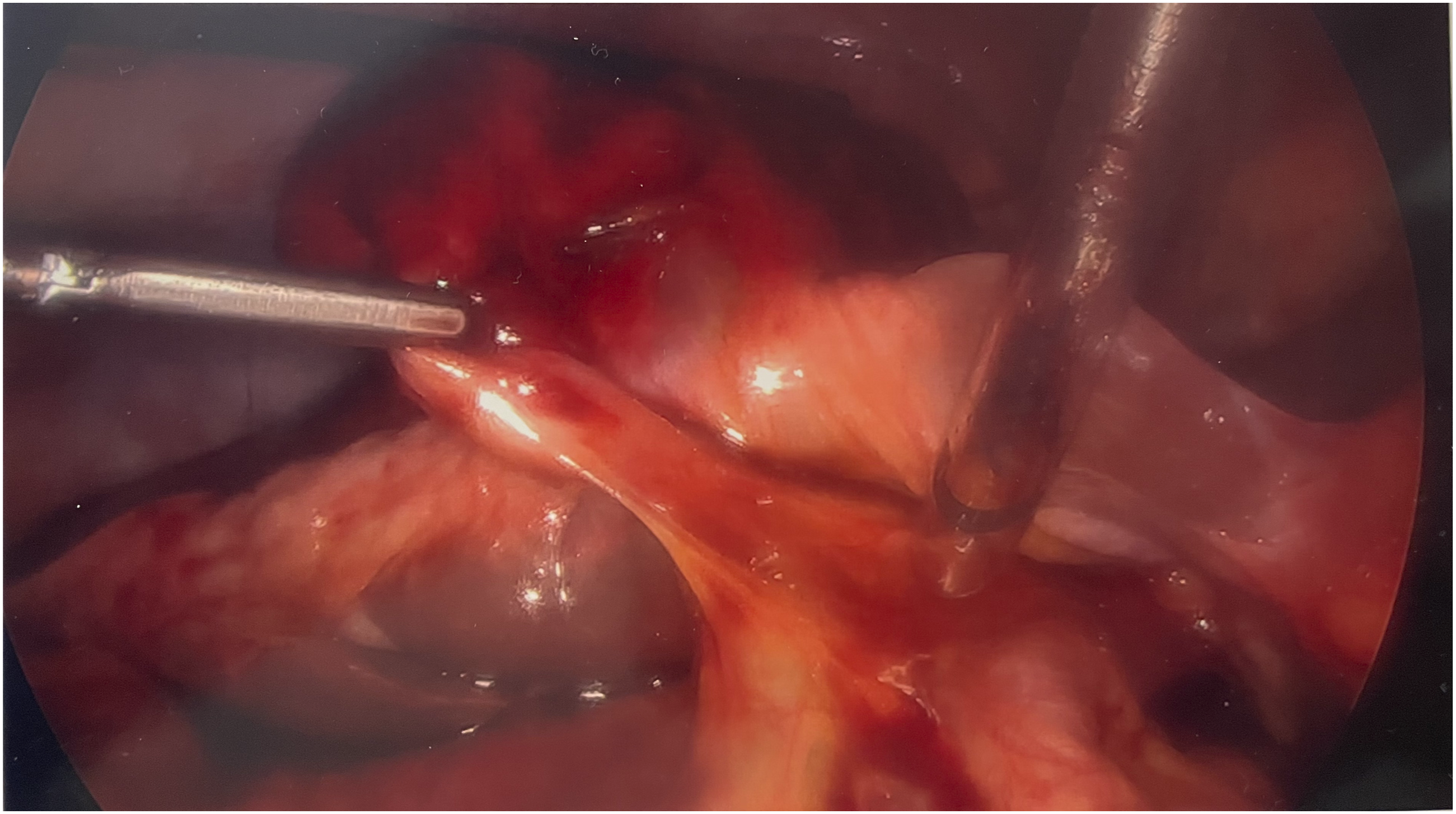
Intraoperatively she was found to have long and lax peritoneal/mesenteric attachments to the liver resulting in volvulus and subsequent ischemia (Figures 2-3). The gallbladder was decompressed and detorsed, and the cholecystectomy was completed in standard fashion after establishing the critical view of safety. Postoperatively the patient recovered without complication. Final pathology of the specimen demonstrated acute and chronic cholecystitis with marked vascular congestion.
Discussion
Gallbladder volvulus is an uncommon but important differential diagnosis in elderly patients presenting with abdominal pain and necessitates prompt surgical intervention. If there is a complete (>180°) torsion of the gallbladder, patients may present with sudden-onset right-sided abdominal pain that may resemble intraabdominal processes such as acute appendicitis or ischemic bowel. In cases of incomplete (<180°) torsion, the signs and symptoms are largely nonspecific and can mimic that of symptomatic cholelithiasis.3-5 Because acute cholecystitis can occasionally be managed nonoperatively with resuscitation and antibiotics or percutaneous drainage, making an early distinction between the 2 diagnoses can be pivotal to patient outcomes. These conservative treatment modalities are not recommended for patients with GV as the condition is not due to an infectious process and neither addresses the underlying pathology. The recommendation for definitive management of GV remains cholecystectomy, with an initial laparoscopic approach favored over open. 6
Several radiographic strategies have been cited as pathognomonic for gallbladder volvulus; however, these findings are unusual and not sensitive enough to be consistently reliable. On ultrasound, the gallbladder wall is typically markedly edematous and can be found positioned outside to the fossa inferior to the liver secondary to the twisted and shortened pedicle. Doppler ultrasound and MRCP with diffusion-weight imaging can be helpful diagnostic adjuncts in demonstrating loss of flow through the cystic artery and gallbladder wall consistent with ischemia. Findings on cross-sectional imaging include a “swirled” appearance along the vascular pedicle and shift in the gallbladder axis from vertical to horizontal, an abrupt tapering of the cystic duct as it transitions from the distended lumen, and reduced enhancement of the gallbladder wall to indicate ischemia.7,8 Delayed diagnosis and subsequently delayed surgery increases risk of complications such as necrosis, perforation, empyema, or multisystem organ failure. 9
Conclusion
In summary, we report a case of gallbladder volvulus initially thought to be acute cholecystitis. On laparoscopy, the patient was found to have torsion of the gallbladder around the cystic pedicle due to loose peritoneal/mesenteric attachments and the gallbladder was ischemic. For patients with concern for GV, prompt surgical treatment is crucial to avoid progression to gallbladder gangrene and rupture which increases morbidity especially in the geriatric population. The judicious use of radiographic markers to establish a preoperative diagnosis of volvulus when there is a high index of suspicion may optimize time to definitive management and overall patient outcomes. Early surgical intervention is essential and remains the cornerstone of treatment for gallbladder volvulus. Computed tomography scan obtained on presentation demonstrating distended gallbladder with significant wall edema. Intraoperative image of gallbladder with significant wall edema and vascular congestion secondary to volvulized cystic vessels. Intraoperative image of gallbladder with long and lax mesenteric attachments allowing for increased mobility leading to torsion.
Footnotes
Consent for Publication
Written informed consent for publication was obtained from the participant. The written document is available in the patient’s hospital record for reference.
Author Contributions
Dai: resident physician, first author.
Myers: resident physician, contributing author.
Zamora: resident physician, contributing author.
Nussbaum: attending surgeon.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.