
Abstract
Background
Perioperative acute myocardial infarction (POMI) complicates 1-5% of non-cardiac operations, influenced by patient risk factors and surgical complexity. The present study used a contemporary, nationally representative cohort of non-cardiac operation patients to characterize current trends in the incidence and impact of POMI. We hypothesized that POMI remains associated with increased mortality, complications, and resource utilization.
Methods
All adult (>18 years) hospitalizations entailing non-cardiac surgical procedures were identified from the 2016-2022 Nationwide Readmissions Database. Non-cardiac operations included intraabdominal, vascular, orthopedic, thoracic, urinary, gynecology, and otolaryngology procedures. Those experiencing POMI comprised the POMI cohort (others: Non-POMI). Multivariable logistic and linear regression models were developed to evaluate the association of POMI with outcomes of interest including in-hospital mortality, postoperative complications, and non-elective readmissions.
Results
Of an estimated 8 633 451 non-cardiac operations, 66% were elective and 0.92% experienced POMI. Relative to others, POMI were older and had a greater burden of chronic medical conditions. Following comprehensive risk-adjustment, POMI was associated with greater in-hospital mortality. Furthermore, POMI was linked with increased hospitalization duration by 4.25 days and costs by $23 710. Additionally, POMI was associated with increased odds of 30-day non-elective readmissions. A modest increase in POMI incidence was observed over time across operative categories.
Conclusion
The incidence of perioperative acute myocardial infarction following non-cardiac operations remains low (∼1%), with modest increases observed across select operative categories. This complication remains associated with substantial mortality, increased resource utilization, and higher rates of non-elective readmissions, underscoring the critical importance of perioperative cardiac risk stratification and optimization.
Introduction
Each year, >200 million adults undergo major non-cardiac surgery (NCS) worldwide. Among them, ∼10 million experience major cardiac complications that account for 1.5 million deaths. 1 In this population, acute myocardial infarction (AMI) affects approximately 1-5% of patients, while myocardial injury demonstrates a 30-day mortality of ∼10%.2,3 As surgical candidates grow older and become increasingly medically complex, characterizing the burden of perioperative AMI (POMI) following these procedures is particularly relevant. 4
Prior studies have demonstrated POMI to be associated with up to a 6-fold increase in early mortality, higher rates of complications, and greater resource utilization, including prolonged hospitalization, higher costs, and greater rates of readmission.3,5 Specifically, Puelacher and coworkers showed the development of POMI following NCS to be associated with a 2.7-fold increase in the odds of 30-day mortality. 6 Yet contemporary national data characterizing its incidence trajectories, complication profiles, and economic impact remain scarce. Whether the burden of POMI has changed meaningfully over time—in the context of evolving surgical techniques, anesthetic practices, and cardiac risk management—is not well established. While prior studies have examined perioperative myocardial infarction using earlier data sets and focused primarily on management and mortality, contemporary national analyses evaluating its incidence, temporal trends, and health care utilization remain limited.
In the present study, we utilized recent national data, incorporated advanced risk-adjustment techniques, and evaluated temporal trends as well as broader health care utilization outcomes, including readmissions, costs, and length of stay across surgical specialties. We hypothesized POMI to remain independently associated with increased in-hospital mortality and postoperative complications among affected patients, duration of hospitalization, and costs as well as greater odds of 30- and 90-day non-elective readmissions.
Methods
This was a retrospective cohort study of the 2016-2022 National Readmissions Database (NRD). As the largest all-payer national repository of readmissions, the NRD uses validated survey-weighting methodology to provide accurate estimates for ∼60% of all U.S. hospitalizations. Readmissions are tracked across hospitals within each calendar year using linkage numbers.
All adult hospitalizations for non-cardiac (intraabdominal, vascular, orthopedic, thoracic, urinary/gynecology, and otolaryngology) operations were tabulated using previously validated International Classification of Diseases 10th Revision (ICD-10) codes (Supplemental Table 1). 7 International Classification of Diseases 10th Revision codes were used to ascertain the presence of POMI, which included both ST-elevation myocardial infarction (STEMI, I21.0, I21.1, I21.2, I21.3) and non-ST-elevation MI (NSTEMI, I21.4). A history of myocardial infarction was identified using ICD-10 code I25.2 (old myocardial infarction). Records involving inter-hospital transfers or missing key data on age, sex, costs, income, or payer status were not considered for analysis (Supplemental Figure 1). The cohort was stratified based on the presence of POMI (POMI vs Non-POMI). Note throughout the manuscript, italics are used when reporting cohort-based comparisons.
Patient and hospital characteristics including age, primary payer, comorbidities, hospital teaching status, bed size, and for-profit ownership were defined in accordance with the NRD Data Dictionary. 8 The burden of chronic conditions was quantified using the Elixhauser Comorbidity Index, a validated score encompassing more than 30 conditions. Individual comorbidities and postoperative complications were classified according to previously published work. 9 The primary outcome of interest was in-hospital mortality among patients with and without POMI. Occurrence of blood transfusion, infectious, renal, respiratory, and thromboembolic complications, as well as markers of resource utilization including inpatient costs, length of stay (LOS), non-home discharge, and 30- and 90-day non-elective readmissions, was secondarily assessed. Non-home discharge was defined as patient disposition to short-term care or skilled-nursing facilities. Costs were calculated by applying center-specific cost to charge ratios to overall hospitalization charges followed by inflation adjustment to the 2022 Personal Health Care Price Index. 10
Categorical variables are reported as percentages (%) and continuous variables are shown as medians with interquartile range (IQR). Pearson’s chi-square and Mann-Whitney U tests were used for bivariate comparisons, as appropriate. Entropy balancing was used to mitigate intergroup differences. Briefly, this reweighting algorithm generates a balanced distribution of covariates and has been shown to be superior to propensity matching. 11 Following the application of entropy balancing-derived weights, multivariable logistic and linear regressions were developed to characterize the association of various covariates with in-hospital mortality and complications. Covariate selection for all models was guided by Elastic net regularization, an automated technique which optimizes model parsimony while reducing collinearity. 12 Risk adjusted models incorporated age, sex, income quartile, payer status, hospital bed size, non-cardiac operation type, and comorbidities (arrhythmia, neurological disorders, renal disease, liver disease, coagulopathy, obesity, pneumonia, peripheral vascular disease, congestive heart failure, diabetes, and hypertension). Linear and logistic model estimates are reported as beta-coefficients (β) or adjusted odds ratios (AOR), as appropriate, both with 95% confidence intervals (CIs). Temporal trends were evaluated using nonparametric tests for trend across ordered groups.
All statistical analyses were performed using Stata 16.0 (StataCorp, College Station, TX). Due to the deidentified nature of NRD, this study was deemed exempt from full review by the Institutional Review Board at the University of California, Los Angeles.
Results
Patient and Hospital Characteristics
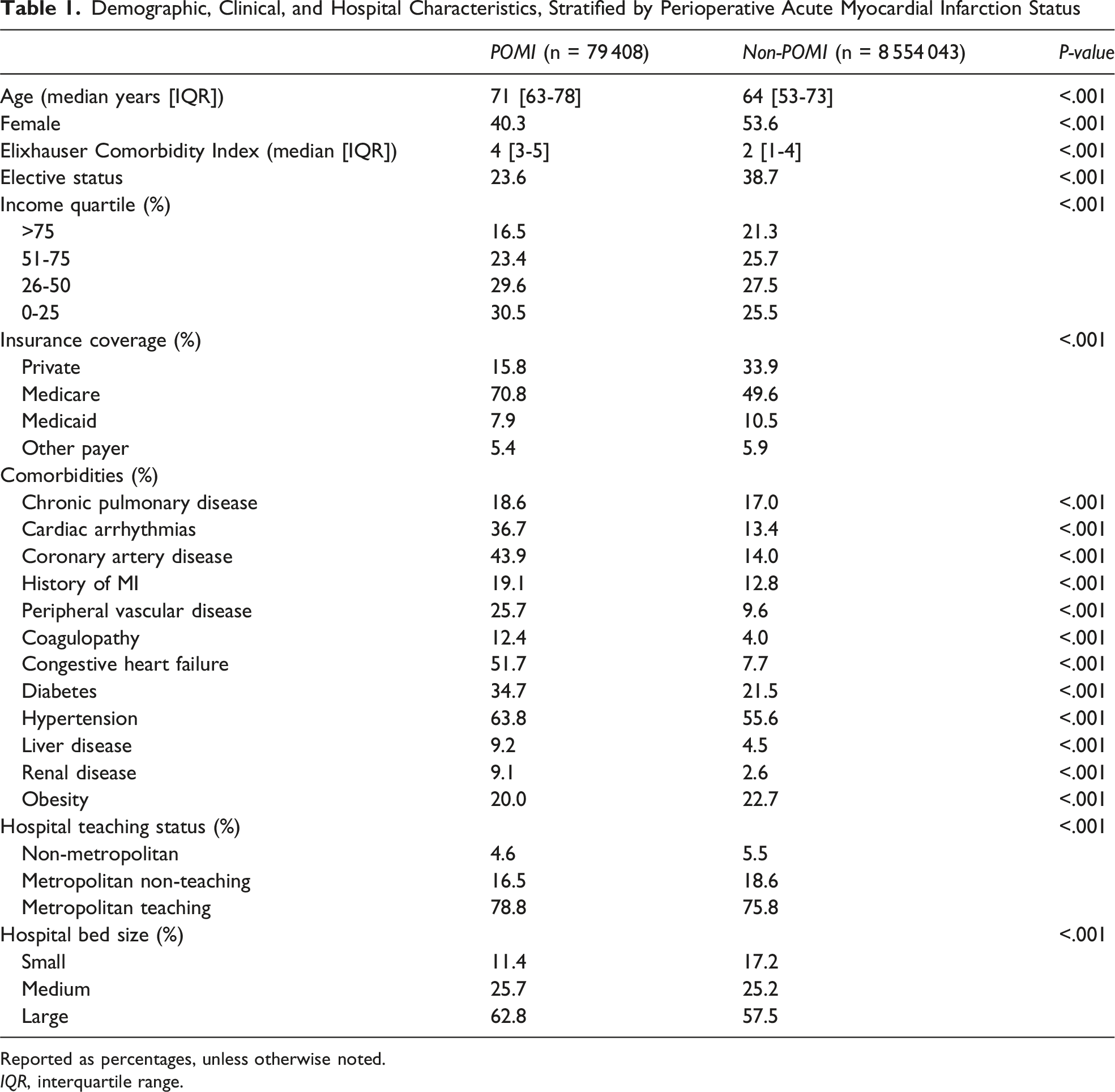
Of an estimated 8 633 451 elective and non-elective patients undergoing non-cardiac operations, 0.92% experienced POMI. The incidence of POMI increased for all operative categories with intraabdominal procedures especially exhibiting a rise from 0.9% in 2016 to 1.2% in 2022 (NP Trend<0.001, Figure 1). Relative to others, POMI were older (71 [63-78] vs 64 [53-73] years; P < .001), less commonly female (40.3 vs 53.6%; P < .001), and more frequently insured by Medicare (70.8 vs 49.6%; P < .001). Perioperative acute myocardial infarction demonstrated higher rates of chronic pulmonary disease (18.6 vs 17.0%; P < .001), hypertension (63.8 vs 55.6%; P < .001), and a history of myocardial infarction (19.1 vs 12.8%, P < .001) but lower rates of obesity (20.0 vs 22.7%; P < .001, Table 1, Figure 2). Temporal trends in the incidence of perioperative acute myocardial infarction across elective and non-elective procedures by surgical specialty. There was a significant difference in distribution across specialties (P < .001) Demographic, Clinical, and Hospital Characteristics, Stratified by Perioperative Acute Myocardial Infarction Status Reported as percentages, unless otherwise noted. IQR, interquartile range. Factors associated with perioperative acute myocardial infarction (POMI). After risk adjustment, diabetes and obesity were linked with greater likelihood of perioperative acute myocardial infarction. However, laparoscopic operations were associated with lowered odds of POMI. *Indicates statistical significance, P < .001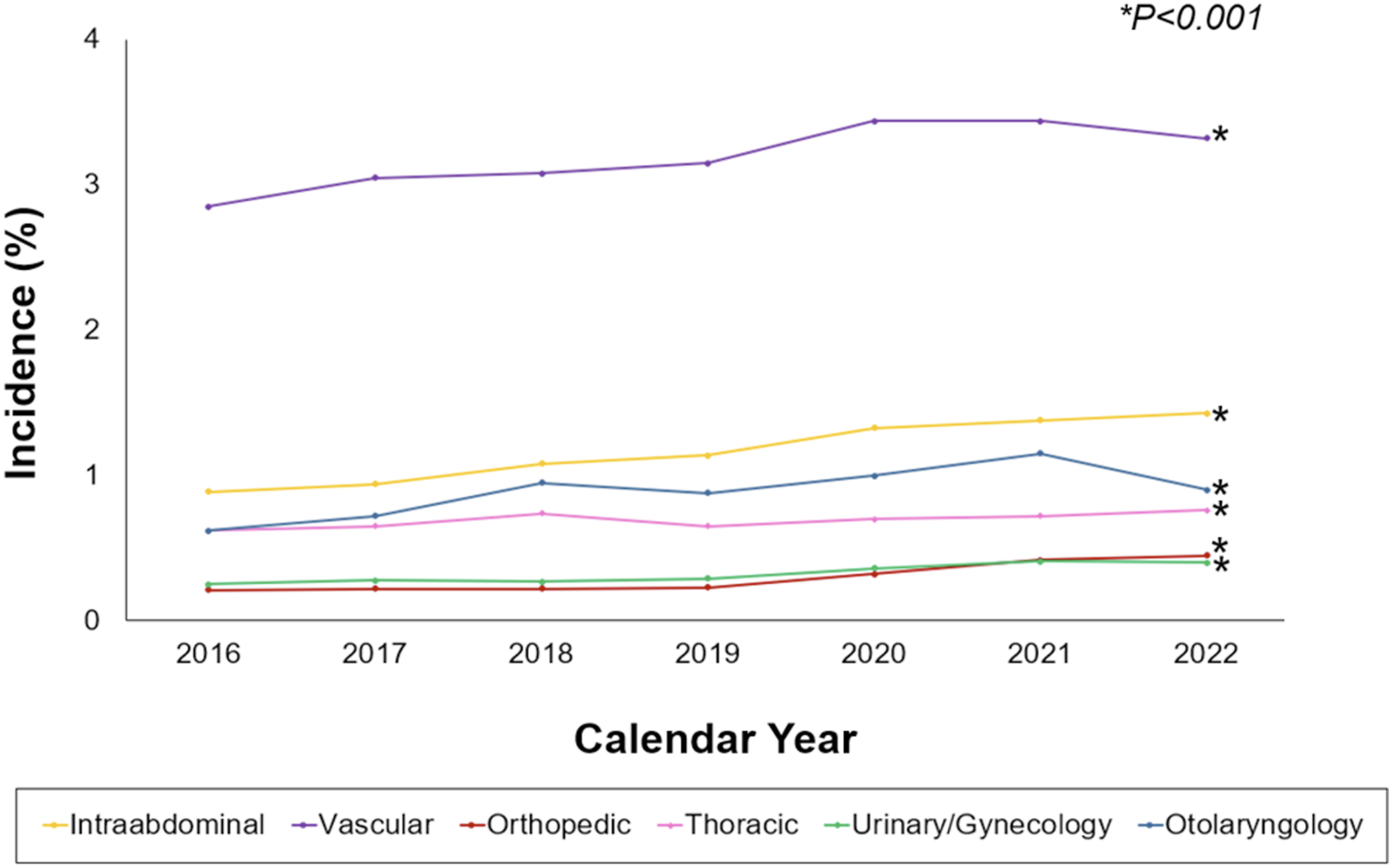
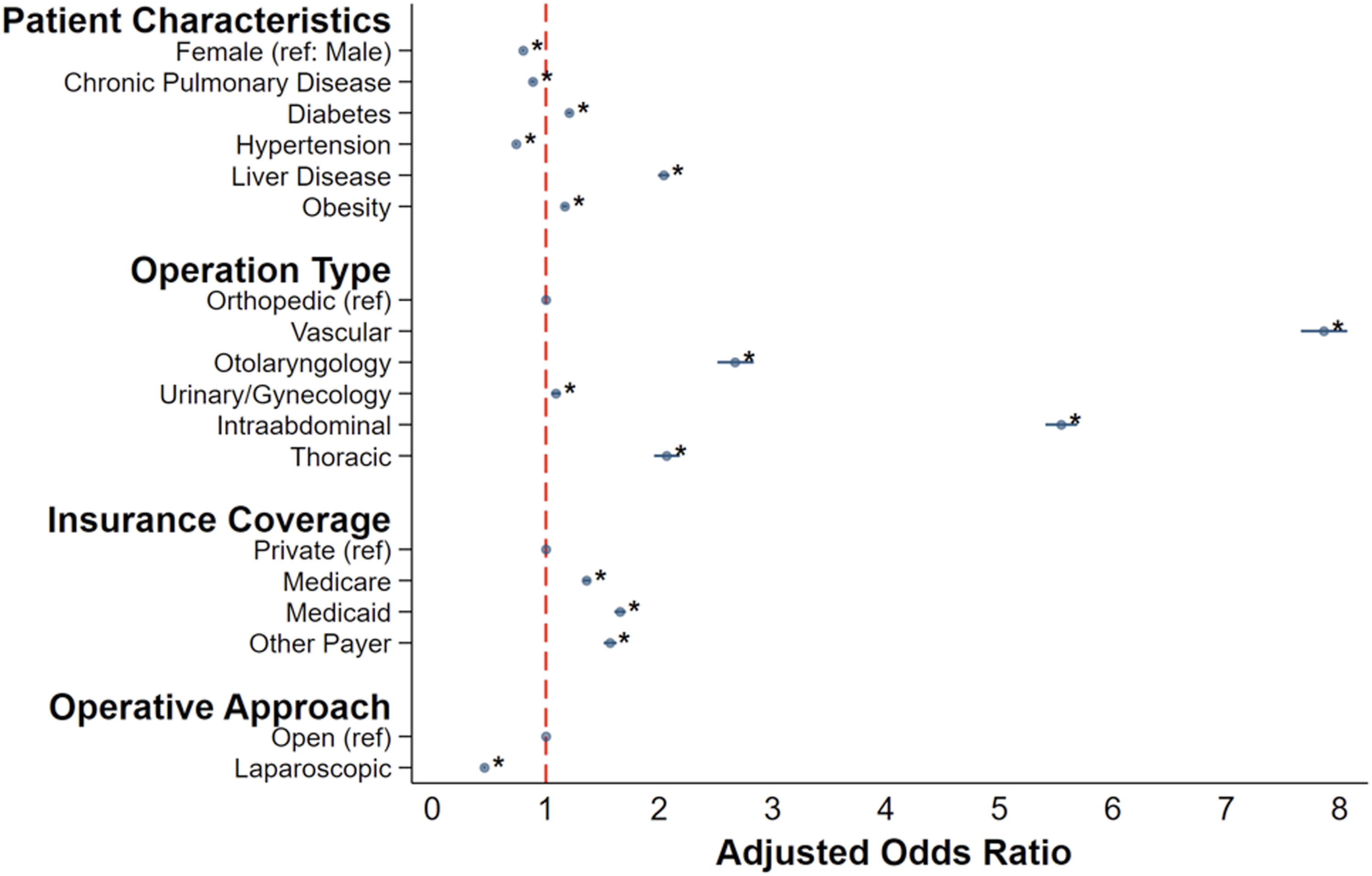
On multivariable analysis, increasing age was associated with higher odds of POMI (AOR 1.04/year, 95% CI: 1.03-1.05), while female sex (AOR 0.80, 95% CI: 0.78-0.81) and elective status (AOR 0.21, 95% CI: 0.20-0.22) were associated with lower odds. Moreover, the lowest income quartile was linked with higher rates of POMI (AOR 1.29, 95% CI: 1.26-1.32, ref: income quartile>75%). diabetes (AOR 1.19, 95% CI: 1.18-1.21), obesity (AOR 1.16, 95% CI: 1.14-1.18), and liver disease (AOR 2.04, 95% CI: 2.00-2.10) were also linked with greater POMI risk, while chronic pulmonary disease (AOR 0.88, 95% CI: 0.86-0.89) was associated with decreased risk. At the hospital level, metropolitan teaching centers (AOR 1.27, 95% CI: 1.22-1.32, ref: non-metropolitan) and private, for-profit hospitals (AOR 1.25, 95% CI: 1.21-1.29, ref: government) demonstrated greater incidence of POMI. Analysis of operative characteristics, using orthopedic procedures as reference (given their high procedural volume and relatively lower baseline risk of perioperative cardiac complications), revealed that vascular (AOR 7.85, 95% CI: 7.65-8.06) and intraabdominal (AOR 5.54, 95% CI: 5.40-5.68) procedures carried the greatest risk. Furthermore, laparoscopic and minimally invasive approaches were found to be protective (AOR 0.46, 95% CI: 0.44-0.47, Supplemental Table 2, Supplemental Figure 1).
Unadjusted Outcomes
Unadjusted and Adjusted Outcomes, Stratified by Perioperative Acute Myocardial Infarction Status
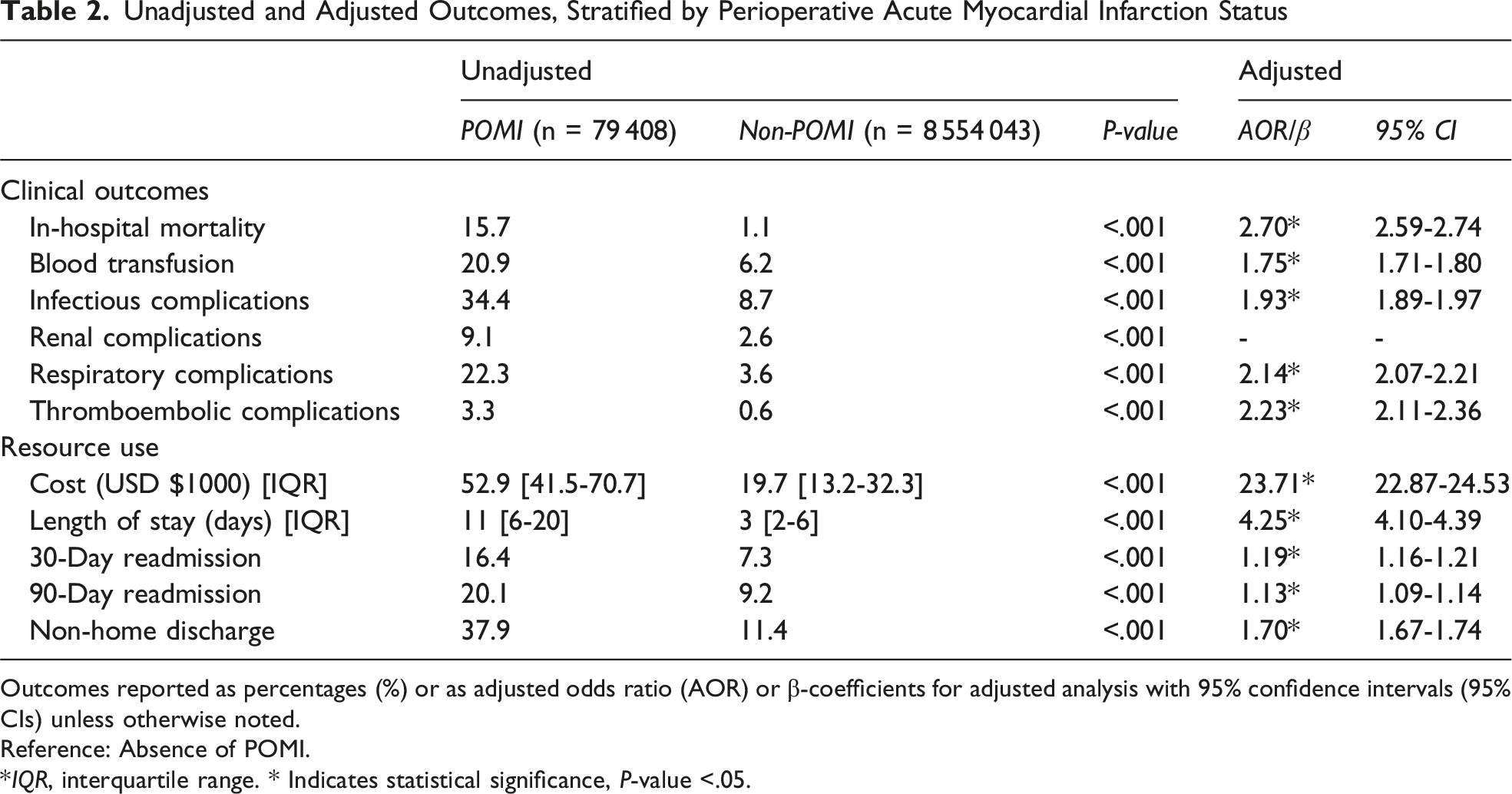
Outcomes reported as percentages (%) or as adjusted odds ratio (AOR) or β-coefficients for adjusted analysis with 95% confidence intervals (95% CIs) unless otherwise noted.
Reference: Absence of POMI.
*IQR, interquartile range. * Indicates statistical significance, P-value <.05.
Risk-Adjusted Outcomes
Adequate balance of patient characteristics and comorbidities was achieved between cohorts using entropy balancing. Following comprehensive risk adjustment, POMI was linked with increased odds of in-hospital mortality (AOR 2.7, 95% CI: 2.59-2.74), blood transfusion (AOR 1.75, 95% CI: 1.71-1.80), and thromboembolic complications (AOR 2.23, 95% CI: 2.11-2.36). Notably, POMI was associated with increased hospitalization costs of $23,710 (95% CI: 22,870-24,530), longer length of stay by 4.25 days (95% CI: 4.10-4.39), and increased odds of 30-day readmission (AOR 1.19; 95% CI: 1.16-1.21, Table 2).
Discussion
Perioperative acute myocardial infarction is a potentially catastrophic complication that carries significant clinical and financial implications for patients and health systems. Notably, the risk of POMI increased slightly across all operative types with vascular and intraabdominal procedures exhibiting the highest odds. Patient characteristics including advanced age, male sex, lower income, and non-elective surgical status were associated with POMI risk. Perioperative acute myocardial infarction remained linked with increased costs of care, prolonged length of stay, and greater readmission rates. Our findings have important clinical implications and warrant detailed examination.
Several patient characteristics were linked to a higher risk of POMI, including older age, male, lower income, and certain comorbidities including obesity and liver disease. These findings identify groups that may benefit from better cardiac monitoring and optimized perioperative surgical management. Our results align with prior work by Smilowitz et al, demonstrating older individuals and those with greater burden of comorbidities to be closely associated with cardiac complications during surgery. 3 Notably, patients in the lowest income group had the highest risk of POMI. This is in agreement with earlier studies reporting a correlation between lower socioeconomic status and inferior surgical outcomes (Haider et al). 13 These gaps may suggest differences in overall health and access to preventive care, revealing opportunities for quality improvement. Additionally, elective surgical status was found to be protective against POMI (adjusted odds ratio [AOR] 0.21), likely reflecting the benefits of comprehensive outpatient risk stratification and preoperative care optimization. In contrast, non-elective procedures remained a significant risk factor for POMI, underscoring the challenges of cardiac risk mitigation in urgent surgical settings. Understandably, opportunities for preoperative optimization are limited in these cases, but this finding still highlights an area for ongoing quality improvement efforts focused on perioperative monitoring, early detection, and postoperative management. Notably, care at for-profit hospitals was independently associated with higher odds of POMI. While prior studies examining hospital ownership and surgical outcomes have yielded mixed results, this finding may reflect differences in perioperative cardiac surveillance protocols or patient case-mix at institutional level.14,15 Given that hospital-level characteristics are incompletely captured in administrative data sets, this association warrants cautious interpretation and represents a potential target for future investigation.
Across the 7-year study period, the overall incidence of POMI following non-cardiac surgery increased, suggesting persistent risk despite advances in perioperative risk assessment tools and monitoring protocols. However, when stratified by operative category, vascular and intraabdominal procedures carried the greatest risk. Of particular concern, intraabdominal surgery was associated with an increase in POMI event rates from 0.9% in 2016 to 1.2% in 2022, potentially reflecting increasing patient complexity or changing perioperative management practices. These findings align with recent work by Thompson et al, who reported an overall increase in the prevalence of cardiovascular risk factors among surgical patients over time, underscoring the need to continually refine perioperative risk assessment. 2 In contrast, orthopedic and urinary/gynecologic procedures were associated with lower odds of POMI. Similar patterns have been observed across other surgical subspecialties, where minimally invasive surgery has been linked to reduced myocardial infarction risk. This association may relate to differences in patient selection, operative technique, and perioperative hemodynamic stability, as well as reduced technical complexity and physiologic stress in minimally invasive approaches.
Notably, patients who experienced POMI demonstrated substantially higher health care resource utilization compared with those without POMI. After risk adjustment, POMI was associated with an additional $23 700 in hospitalization costs and a prolonged length of stay of 4.3 days. Furthermore, elevated 30-day readmission rates and an approximately threefold higher odds of mortality suggest that the consequences of POMI extend well beyond the index hospitalization. These findings emphasize the importance of perioperative cardiac risk mitigation strategies and suggest that investments in preoperative optimization, intraoperative monitoring, and postoperative surveillance may yield meaningful improvements in outcomes while reducing health care costs.
This study has several important limitations. First, it relies on ICD-10 coding, which may be subject to misclassification and may not capture all clinically relevant POMI events. Second, the data set lacks granular clinical detail, including physiologic parameters, perioperative timing of events, perioperative medication use, and laboratory data. As a result, we cannot determine whether POMI precipitated postoperative complications or occurred as a consequence of them, nor can we evaluate mechanistic pathways or symptom burden. Additionally, the NRD does not reliably capture the temporal relationship between perioperative myocardial infarction and subsequent interventions, limiting our ability to evaluate post-POMI management such as percutaneous coronary intervention or coronary artery bypass grafting. Future studies may evaluate differences in outcomes based on POMI subtype (STEMI vs NSTEMI), which may have distinct clinical implications.
In conclusion, POMI following non-cardiac surgery remains uncommon but clinically consequential. While the overall incidence of POMI remains relatively low (∼1%), modest increases were observed over time across certain operative categories. Given the high volume of non-cardiac operations performed annually, even this low incidence translates into a substantial economic and public health burden. Patients undergoing non-elective surgery and those in the lowest income quartile are at particularly elevated risk, underscoring the need for targeted interventions to address socioeconomic disparities and optimize perioperative care in urgent surgical settings. Finally, the observed temporal increase in POMI among non-cardiac procedures warrants further investigation and represents a potential target for future quality improvement initiatives.
Supplemental Material
Supplemental material - Perioperative Acute Myocardial Infarction in Non-Cardiac Operations: A National Analysis
Supplemental material for Perioperative Acute Myocardial Infarction in Non-Cardiac Operations: A National Analysis by Sona Mahrokhi, Konmal Ali, Robert Kropp, Ellis Gao, Kruti Desai, Melissa Justo, Yas Sanaiha, and Peyman Benharash in The American Surgeon™
Supplemental Material
Supplemental material - Perioperative Acute Myocardial Infarction in Non-Cardiac Operations: A National Analysis
Supplemental material for Perioperative Acute Myocardial Infarction in Non-Cardiac Operations: A National Analysis by Sona Mahrokhi, Konmal Ali, Robert Kropp, Ellis Gao, Kruti Desai, Melissa Justo, Yas Sanaiha, and Peyman Benharash in The American Surgeon™
Footnotes
Author Note
This study was presented at the 2026 Southern California Chapter of the American College of Surgeons Annual Meeting in Santa Barbara, CA, January 2026.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
PB reports receiving proctoring fees from AtriCure Inc. This manuscript does not discuss any related products or services. All other authors report no conflicts or disclosures.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.