
Abstract
Background
Barrier-coated meshes were developed to minimize adhesion formation between the PM and adjacent viscera. However, prior data has shown an increased infectious risk associated with rapidly absorbable coated PM vs uncoated PM in open preperitoneal AWR (OPPAWR). This study evaluated differences in wound and mesh infection rates between coated and uncoated PM in patients undergoing OPPAWR.
Materials and Methods
A prospectively maintained, tertiary hernia center database was queried for patients undergoing OPPAWR with PM in CDC class 1/2 wounds. Using 1:1 propensity-score matching (PSM), coated and uncoated groups were matched on factors known to influence outcomes. Multivariable regression models determined independent predictors of wound and infectious complications.
Results
Of 1450 patients with coated and uncoated PM, 382 pairs were well-matched. Propensity-score matching covariates were similar (all P > 0.05). The coated group had higher rates of wound infection (6.3% vs 3.1%), postoperative IV antibiotics (8.6% vs 4.7%), percutaneous drain placement (6.8% vs 3.1%), and mesh infection (2.4% vs 0.0%) (all P < 0.05), but no significant difference in composite wound complications (20.4% vs 16.5%; P = 0.162). Multivariable regression showed panniculectomy (OR: 1.87, 95% CI: 1.25-2.82; P = 0.003) and BMI (OR: 1.05, 95% CI: 1.02-1.08; P = 0.002) were independent predictors of wound complications, but coated mesh was not (OR: 0.78, 95% CI: 0.53-1.15; P = 0.211). In the infectious model regression, panniculectomy remained an independent predictor (OR: 2.01, 95% CI: 1.24-3.25; P = 0.005), while coated mesh again was not (OR: 0.65, 95% CI: 0.41-1.04; P = 0.074).
Discussion
In the largest reported cohort, following complex OPPAWR, multivariable regression demonstrated that coated PM did not independently predict wound or infectious complications.
Introduction
Ventral hernia repair is among the most commonly performed procedures in general surgery. 1 Mesh reinforcement has been well-established to reduce hernia recurrence rates as compared with primary suture repair.2,3 However, the long-term success of hernia repair depends not only on durable fascial closure but also on minimizing postoperative wound and mesh-related complications, as wound morbidity has been shown to increase recurrence risk by up to 7-fold.4–7
Barrier-coated meshes were introduced to reduce adhesion formation between the mesh and adjacent viscera, aiming to prevent certain dreaded complications, such as enterocutaneous fistulae and adhesive bowel disease.8–10 Despite these potential advantages, several studies have reported an increased risk of infection with barriers made of nonporous, solid polytetrafluoroethylene (PTFE) or solid, slowly absorbing omega-3 fatty coating, as barrier coatings themselves may elicit a more prolonged inflammatory response than uncoated alternatives and prevent proper tissue incorporation.8,9
Our institution previously compared coated polypropylene mesh with uncoated polypropylene mesh in open preperitoneal abdominal wall reconstruction (OPPAWR), finding higher rates of wound and mesh infections in the coated group. 11 The present study sought to evaluate these findings in a larger patient cohort to further define the impact of coated mesh on postoperative wound morbidity in OPPAWR.
Materials and Methods
Patient Population
Following Institutional Review Board approval, a prospectively maintained institutional database at a tertiary hernia center was queried for patients who underwent elective open AWR with preperitoneal polypropylene mesh reinforcement from 2007 to 2025. Throughout this time period, evidence-based patient prehabilitation protocols were implemented and shown to improve postoperative outcomes, with an emphasis on glycemic control, smoking cessation, weight loss, and consultation with the geriatric medicine service.12,13
Operative Technique
All surgeons were members of Carolinas Advanced Laparoscopic and Advanced Surgery Program and were fellowship-trained in minimally invasive surgery and abdominal wall reconstruction, with consistent overall practices and technique. Each surgeon placed mesh in the preperitoneal plane, which is the preferred approach at this institution due to the ability to achieve large mesh overlap in an extraperitoneal location without the need for component separation. This anatomic space separates the mesh from direct contact with intra-abdominal contents and allows for minimal fixation as the mesh is completely extraperitoneal.6,14
Propensity-Score Matching and Outcomes
Comorbidities included in the number of comorbidities variable include alcoholism, anxiety, arrhythmia, asthma, atrial fibrillation, congestive heart failure, cirrhosis/liver disease, COPD, coronary artery disease, cerebrovascular accident, depression, diabetes, chronic kidney disease, gastroesophageal reflux disease, history of cancer, history of deep vein thrombosis or pulmonary embolism, history of myocardial infarction, history of MRSA infection, HIV, hyperlipidemia, hypertension, hypotension, hyperthyroidism, hypothyroidism, illicit drug use, preoperative anemia, previous intra-abdominal surgery or trauma, pulmonary hypertension, peripheral vascular disease, and sleep apnea.
Panniculectomy, a factor known to be associated with an increase in wound complications, was excluded from the PSM because its inclusion reduced match quality. Instead, panniculectomy was controlled for in the subsequent multivariable regression rather than during the matching process. The primary outcomes were composite wound complications and mesh infection. To distinguish overall wound morbidity from infection-specific outcomes, two composite variables were defined. The composite wound complications variable included cellulitis, wound breakdown, superficial or deep wound infection, seroma requiring intervention, hematoma, and mesh infection. The composite infectious complications variable included wound infection, intra-abdominal abscess, postoperative intravenous (IV) antibiotics, percutaneous drainage, and mesh infection. The secondary outcomes were the need for postoperative IV antibiotics, percutaneous drainage, 30-day reoperation, and mesh explantation. The Carolinas Equation for Determining Associated Risks (CeDAR), a validated risk-stratification tool developed from prior institutional data to estimate postoperative wound complication risk, was used to determine whether there was a difference in predicted wound complication rate between the coated and uncoated mesh cohorts. 18
Data Entry and Statistics
Trained research analysts entered demographic, operative, and postoperative data into a standardized institutional database based on information available in the electronic medical record. Attending surgeons did not have access to the data and were not involved in data entry or analysis.
Standard statistical methods were applied. Descriptive statistics were reported as means with standard deviations for continuous variables and as frequencies with corresponding percentages for categorical variables. Comparisons between categorical variables were performed using the chi-square or Fisher’s exact test, as appropriate. Continuous variables were analyzed using the Wilcoxon rank-sum test for nonparametric data. Multivariable logistic regression models were constructed to identify independent predictors of composite wound complications and infectious complications after adjusting for clinically relevant covariates. Statistical significance was defined as a two-tailed P-value of <0.05. All analyses were performed using Statistical Analysis Software (SAS) version 9.4 (SAS Institute, Inc., Cary, NC) by a trained statistician.
Results
Propensity-Score Match Analysis
PSM Covariates and Demographic Information for Coated vs Uncoated PM
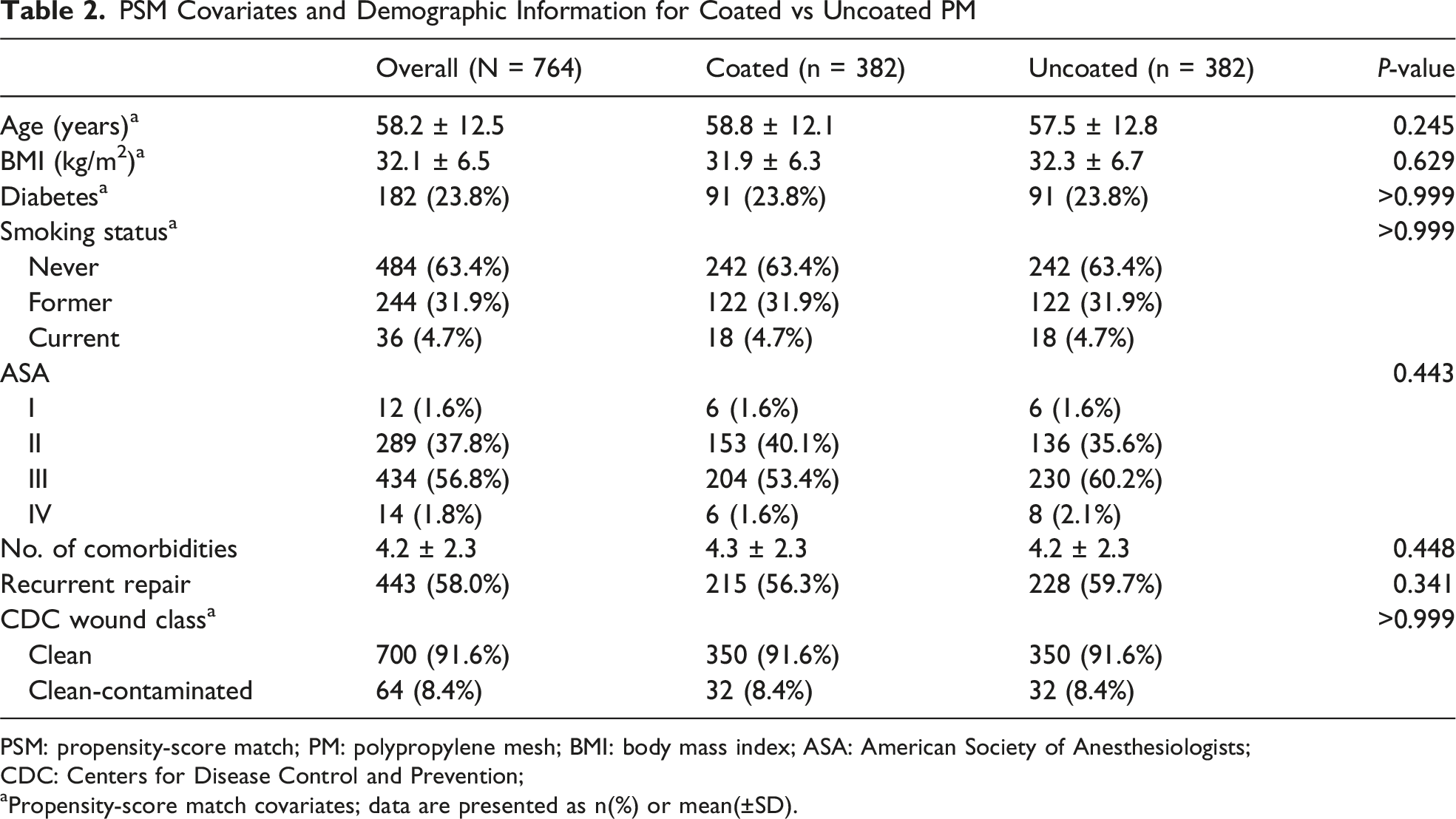
PSM: propensity-score match; PM: polypropylene mesh; BMI: body mass index; ASA: American Society of Anesthesiologists;
CDC: Centers for Disease Control and Prevention;
aPropensity-score match covariates; data are presented as n(%) or mean(±SD).
Intraoperative Details of Coated vs Uncoated PM
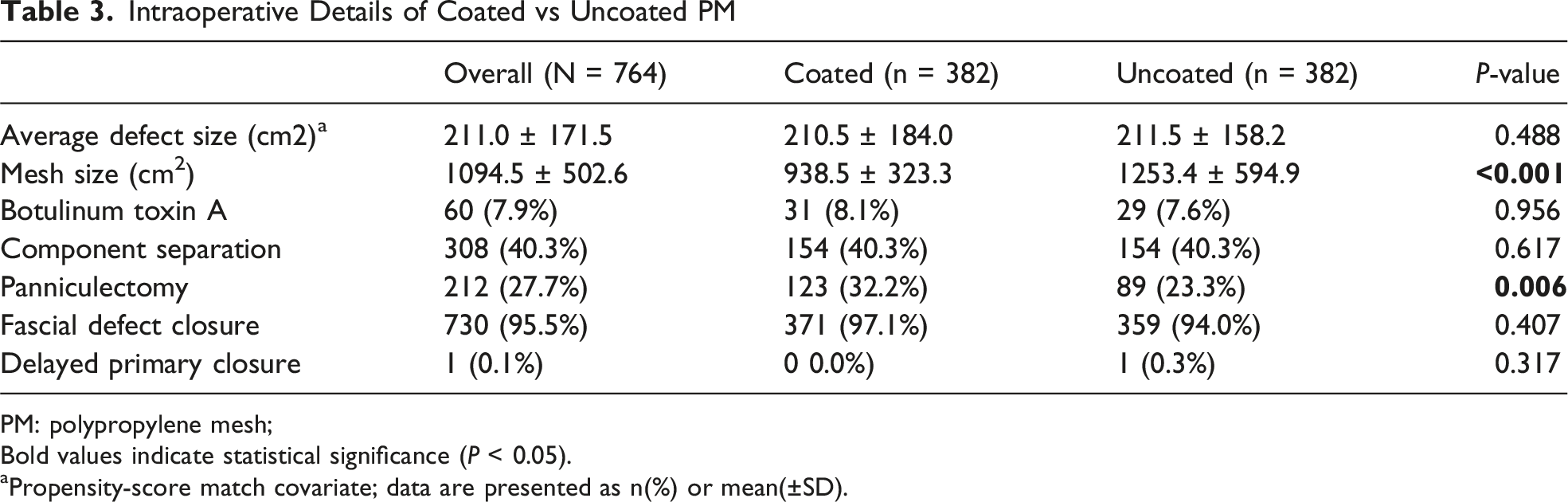
PM: polypropylene mesh;
Bold values indicate statistical significance (P < 0.05).
aPropensity-score match covariate; data are presented as n(%) or mean(±SD).
Length-of-stay was longer in the coated group (5.4 ± 3.4 vs 4.3 ± 3.0 days; P < 0.001). There was no significant difference in composite wound complications (20.4% vs 16.5%; P = 0.162), but the coated group had higher rates of wound infection (6.3% vs 3.1%; P = 0.040), postoperative IV antibiotics (8.6% vs 4.7%; P = 0.039), percutaneous drain placement (6.8% vs 3.1%; P = 0.026), and mesh infection (2.4% vs 0.0%; P = 0.004). Of the nine total mesh infections, all of which were in the coated mesh group, five ultimately required mesh excision; the rest required prolonged antibiotics. One of these patients had developed multiple colocutaneous fistulae following their mesh infection and underwent fistulae takedown at the time of mesh excision with primary suture repair of the recurrent hernia. The other four patients underwent biologic mesh repair following mesh excision. Four patients underwent successful conservative management of their mesh infection with antibiotics and percutaneous drainage. There were no significant differences in cellulitis (5.8% vs 4.5%; P = 0.411), wound breakdown (5.0% vs 2.4%; P = 0.054), seroma requiring intervention (10.5% vs 8.1%; P = 0.262), hematoma (3.7% vs 3.1%; P = 0.720), fistula (0.3% vs 0.0%; P > 0.999), or bowel obstruction (2.1% vs 1.6%; P = 0.596). Within the coated mesh group, Proceed had significantly higher composite wound complications than Ventralight (42.9% vs 17.7%; P < 0.001). There were no differences in composite wound complications among the different uncoated mesh types (Marlex, Prolite, Prolene) (15.2% vs 16.6% vs 20.0%; P > 0.999). There was no statistical difference in unplanned 30-day reoperations (1.6% vs 1.8%; P = 0.780) or 30-day readmissions (5.8% vs 2.9%; P = 0.050). In the coated mesh cohort, indications for reoperation included hematoma evacuation (n = 3) and wound-related complications (n = 3). In the uncoated mesh cohort, reoperations were performed for hematoma evacuation (n = 5) and wound-related complications (n = 2).
Postoperative Outcomes of Coated vs Uncoated PM
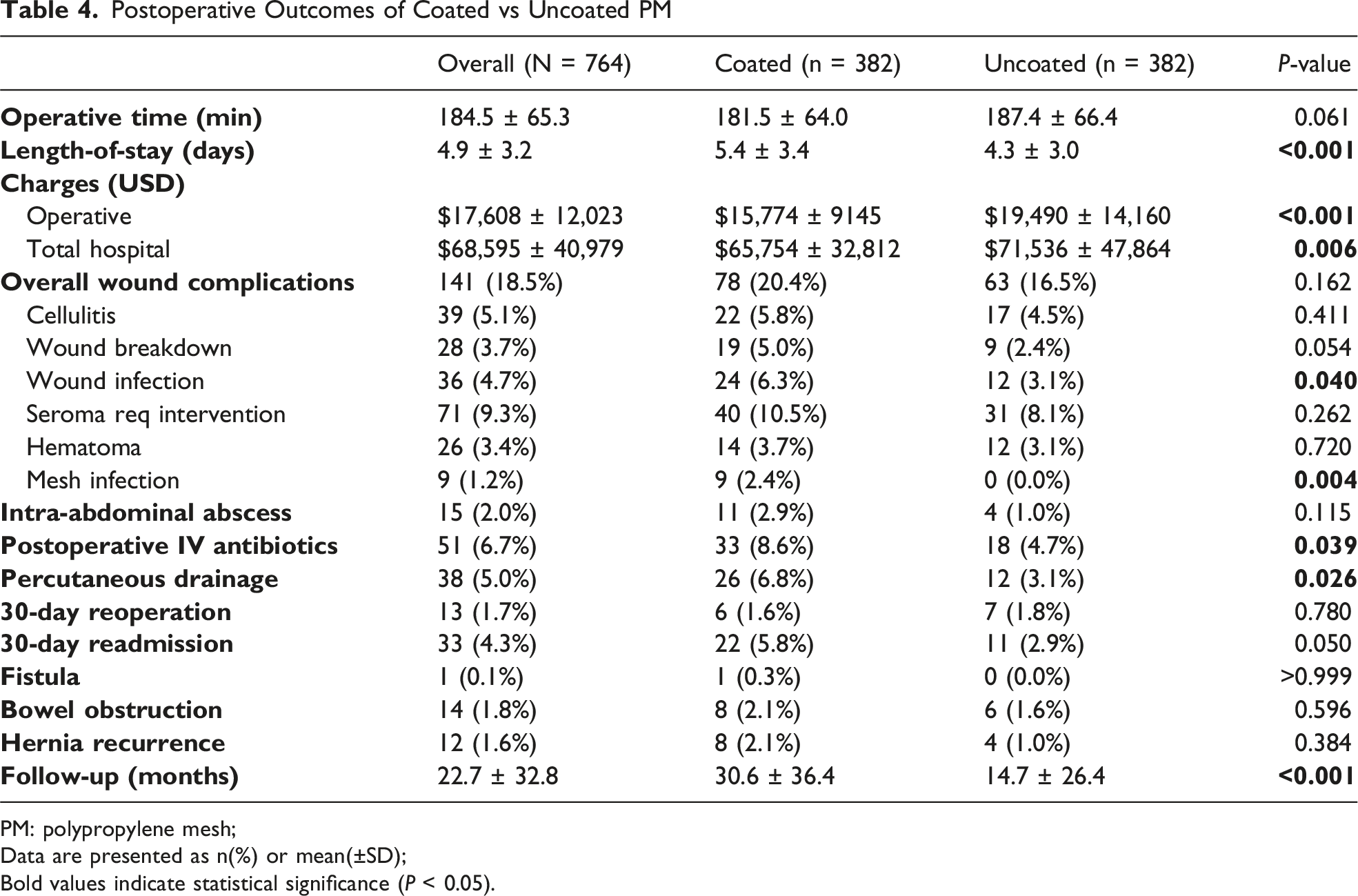
PM: polypropylene mesh;
Data are presented as n(%) or mean(±SD);
Bold values indicate statistical significance (P < 0.05).
Multivariable Regression for Wound Complications
Multivariable Regression for Composite Wound Complications
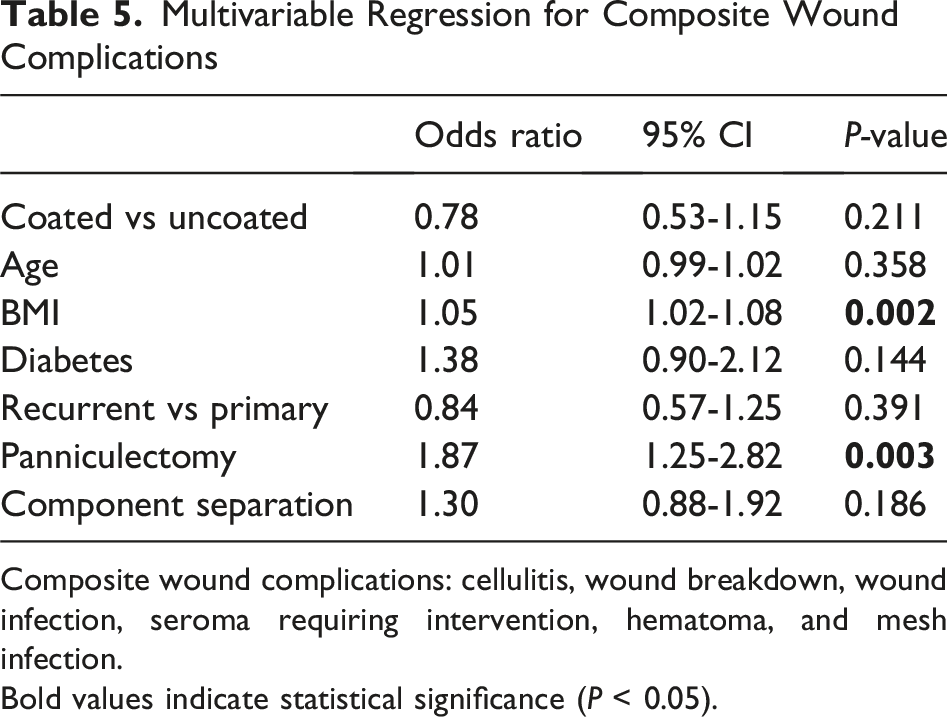
Composite wound complications: cellulitis, wound breakdown, wound infection, seroma requiring intervention, hematoma, and mesh infection.
Bold values indicate statistical significance (P < 0.05).
Multivariable Regression for Infectious Complications
Multivariable Regression for Composite Infectious Complications
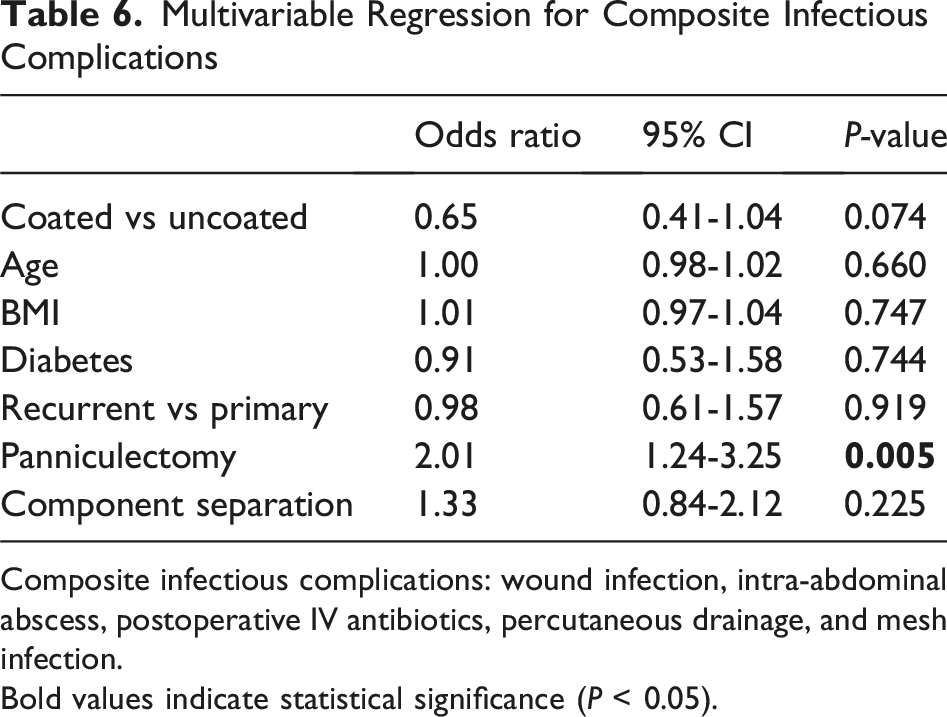
Composite infectious complications: wound infection, intra-abdominal abscess, postoperative IV antibiotics, percutaneous drainage, and mesh infection.
Bold values indicate statistical significance (P < 0.05).
Discussion
In this propensity-matched cohort of elective OPPAWR in CDC class 1/2 wounds, coated polypropylene mesh was associated with higher rates of several infectious postoperative events on univariate analysis, including wound infection, postoperative IV antibiotic use, percutaneous drainage, and mesh infection. However, when evaluating the broader composite wound-complication endpoint in an adjusted multivariable model, coated mesh was not an independent predictor of wound complications; instead panniculectomy and BMI drove risk. These findings suggest that the observed excess wound morbidity with coated mesh may be confounded by patient- and procedure-level factors and may not reflect a direct causal effect of coating alone. This makes sense; the wound is not impacted by mesh choice, but mesh infection is.
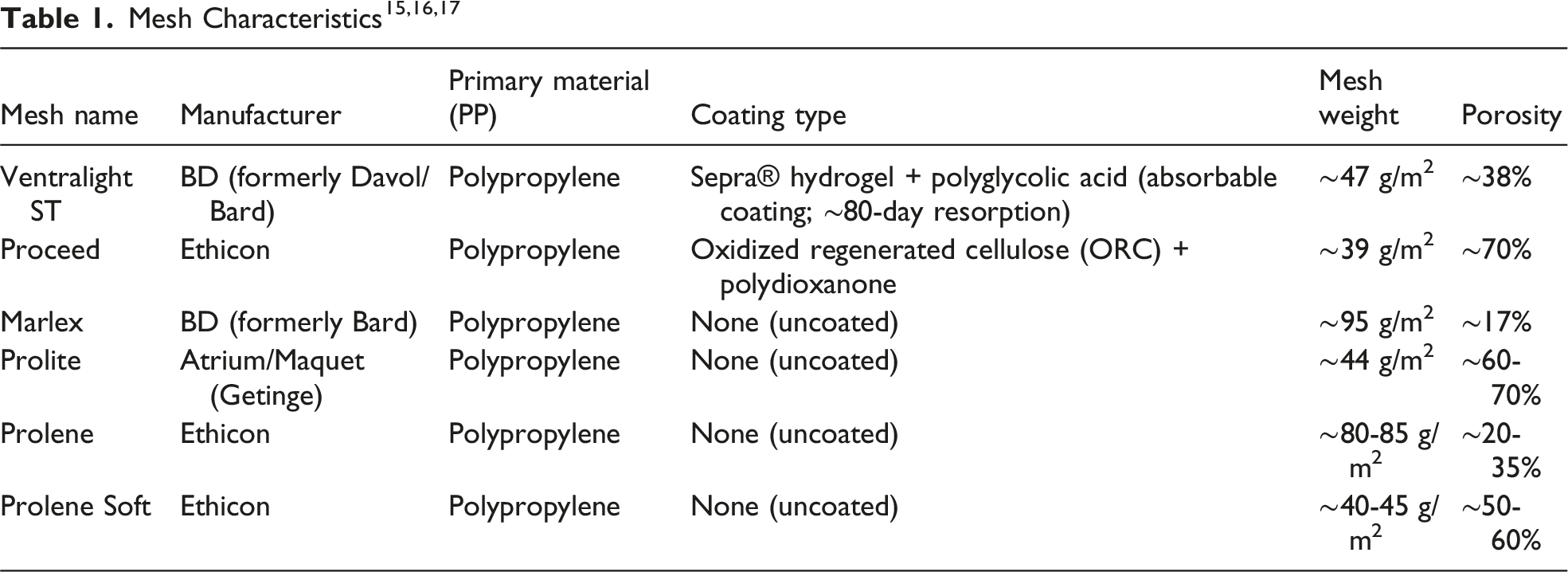
Barrier-coated meshes were originally developed to reduce adhesion and fistulae formation with intraperitoneal mesh placement.8–10 However, previous literature has demonstrated that certain coatings, particularly solid PTFE or slowly absorbing, nonporous omega-3 fatty acid barriers, can provoke a heightened inflammatory state and increased bacterial accumulation relative to uncoated polypropylene mesh.4,14,19 Ventralight and Proceed mesh, the two coated meshes evaluated in this study, are both midweight, macroporous polypropylene prostheses with absorbable anti-adhesion barriers, such as ST hydrogel for Ventralight and oxidized regenerated cellulose (ORC) for Proceed. 20 In Ventralight mesh, the absorbable barrier is generally resorbed by 80 days, exposing the permanent polypropylene layer, while the ORC component of Proceed mesh is degraded within one month. 21 Interestingly, although both are coated polypropylene meshes, Proceed had over twice the wound complication rate as Ventralight suggesting an impact of the ORC barrier.
Multiple studies have supported the safety and efficacy of these meshes when used in laparoscopic intraperitoneal onlay mesh (IPOM), demonstrating favorable recurrence rates and low postoperative surgical site infections.15,16,22 While their performance in the extraperitoneal space remains poorly studied, it is known that the very properties that limit visceral adhesions also reduce early-phase integration, impeding tissue incorporation when placed in the sublay location. 23 This amplifies local inflammation and increases the potential space for fluid collections and infection. 24 Indeed, a prior Americas Hernia Society Quality Collaborative (AHSQC) analysis demonstrated increased seroma formation with coated mesh in the retrorectus space. 23 However, this study did not take patient prehabilitation into consideration, which is a factor known to influence postoperative outcomes, meshes were not in the same anatomical space as in this study, and it may be biased by surgeon-reported outcomes. 12 As mentioned previously, standardized, evidence-based prehabilitation strategies were implemented throughout the timeframe of the current study, focusing on glycemic control, smoking cessation, and weight loss.12,13
A previous institutional propensity-score matched study demonstrated higher rates of wound dehiscence, wound infection, and mesh infection with Proceed and Ventralight meshes compared with uncoated polypropylene alternatives. 11 The current, larger matched cohort reinforces this increased wound and mesh-related morbidity among patients with coated mesh, with all mesh infections occurring exclusively in the coated cohort. Although the absolute number of events was small, mesh infection represents a particularly consequential complication that often necessitates prolonged antibiotics, procedural intervention, or mesh explantation, and it is strongly associated with repair failure and increased healthcare utilization. Despite this, with the addition of multivariable regression, coated mesh itself was not an independent predictor of wound complications. This suggests that there may be additional clinical factors driving wound risk.
Although defect sizes were similar between groups in this current study, coated mesh cases used significantly smaller mesh sizes. This finding likely reflects differences in the manufactured size options for each mesh type. While smaller mesh size can contribute to repair failure, at least 5 cm of overlap on each side of the hernia defect was maintained in all cases to minimize risk of recurrence, with a mesh to defect area ratio of over 4 in the coated group. While this study did not demonstrate a statistically significant difference in recurrence rates between groups, the coated mesh group did have a higher recurrence rate than the uncoated mesh group, which may in part reflect the significantly longer duration of follow-up. However, this is likely multifactorial, as wound infections are known to increase repair failure by 3- to 7-fold. 6
Concomitant panniculectomy and elevated BMI are recognized risk factors for wound morbidity in AWR. 25 In the current study, panniculectomy was performed more frequently within the coated mesh cohort and was shown to be independent predictor of both wound and infectious complications on multivariable regression. While this may partially explain the observed outcomes, a previous institutional study demonstrated a significant reduction in wound complications associated with concomitant panniculectomy over time (50.5% vs 25.0%; P < 0.001), reflecting improvements in prehabilitation, surgical technique, and postoperative wound management, particularly with the use of an incisional VAC. 26 Although BMI was well-matched between cohorts in the present study, it also remained an independent predictor of wound complications on multivariable regression. These findings underscore the importance of careful patient selection and prehabilitation. Identifying patients who may benefit from weight loss prior to AWR is essential, especially when planning concomitant procedures. Tailoring operative strategies to individual risk profiles may help improve overall outcomes for patients undergoing AWR.
Despite these limitations, there are practical reasons as to why our surgeons choose coated polypropylene mesh for preperitoneal AWR. Potential benefits include lower risk of mesh to bowel contact in complex cases where peritoneal integrity is tenuous. In these cases, the absorbable coating may offer an additional layer of protection during the early healing period, minimizing potential visceral exposure to the mesh. However, it is important to note that there were no statistical differences in the rates of fistula or bowel obstruction between the coated and uncoated mesh cohorts in the current study. Other factors include availability of products based on hospital contracts in the operating room and patient preference.
This study has several limitations. First, despite the use of propensity-score matching to control for factors known to influence outcomes, unquantified confounders may still influence the observed outcomes. Second, the analysis was conducted at a single, high-volume tertiary hernia center where all meshes were placed in the preperitoneal plane. Although this may limit generalizability to centers using different techniques or mesh locations, it also serves as a strength by providing a uniform operative approach and reducing heterogeneity in mesh placement. It may be deduced that these results would also be applicable in the retrorectus plane, which is the other extraperitoneal plane that is commonly utilized by general surgeons. Additionally, certain potentially relevant intraoperative variables, such as episodes of hypotension and temperature fluctuations, are not captured in our data set and may contribute to postoperative wound morbidity. Mesh infection, which was an infrequently observed outcome in this study, may indeed be impacted by mesh type; however, its effect is not amenable to a regression analysis due to the small number of events observed. Finally, a notable limitation of this study is the difference in follow-up duration between the coated and uncoated mesh cohorts, with the uncoated mesh group having significantly shorter follow-up. This may influence the assessment of long-term outcomes, particularly mesh infection and hernia recurrence. As a result, the lower observed rates of these complications in the uncoated mesh group may partially reflect this shorter follow-up period rather than true clinical differences. Longer and more similar follow-up duration across groups is necessary to further evaluate the safety and durability of coated vs uncoated mesh in AWR.
Although the propensity score-matched analysis demonstrated higher rates of wound and mesh infections in the coated polypropylene mesh cohort, multivariable regression identified panniculectomy and BMI, not mesh type, as independent predictors of wound complications. These results suggest that patient- and procedure-specific factors play a more significant role in wound morbidity than the choice between coated and uncoated polypropylene mesh, supporting the judicious use of absorbable coated polypropylene mesh in the preperitoneal plane, once all patient and operative factors have been considered.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work did not receive any external funding; it was funded solely by the Carolinas Laparoscopic and Advanced Surgery Program.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Heniford receives surgical and research education grants and honoraria from W. L. Gore and Medtronic, an educational grant from Intuitive, and a research grant from Merck. Dr. Augenstein receives speaking honoraria from Allergan, Pacira, and Medtronic. Dr. Ayuso receives education funding, is a speaker, and consultant for Boston Scientific. Dr. Kerr, Dr. Walker, Dr. Hinton, and Mr. Scarola have no disclosures to report.