
Abstract
Introduction
Cholecystectomy is considered the gold standard treatment for symptomatic gallstone disease. In certain cases, due to technical difficulties, a subtotal cholecystectomy may be performed. Between 1998 and 2015, a total of 1 423 080 laparoscopic cholecystectomies were performed. 10 162 patients who underwent completion cholecystectomy were identified and stratified by age (<50 vs. ≥50 years). This study examines outcomes and risk factors associated with completion cholecystectomy following partial (subtotal) cholecystectomy, with a focus on age and comorbidity burden.
Results
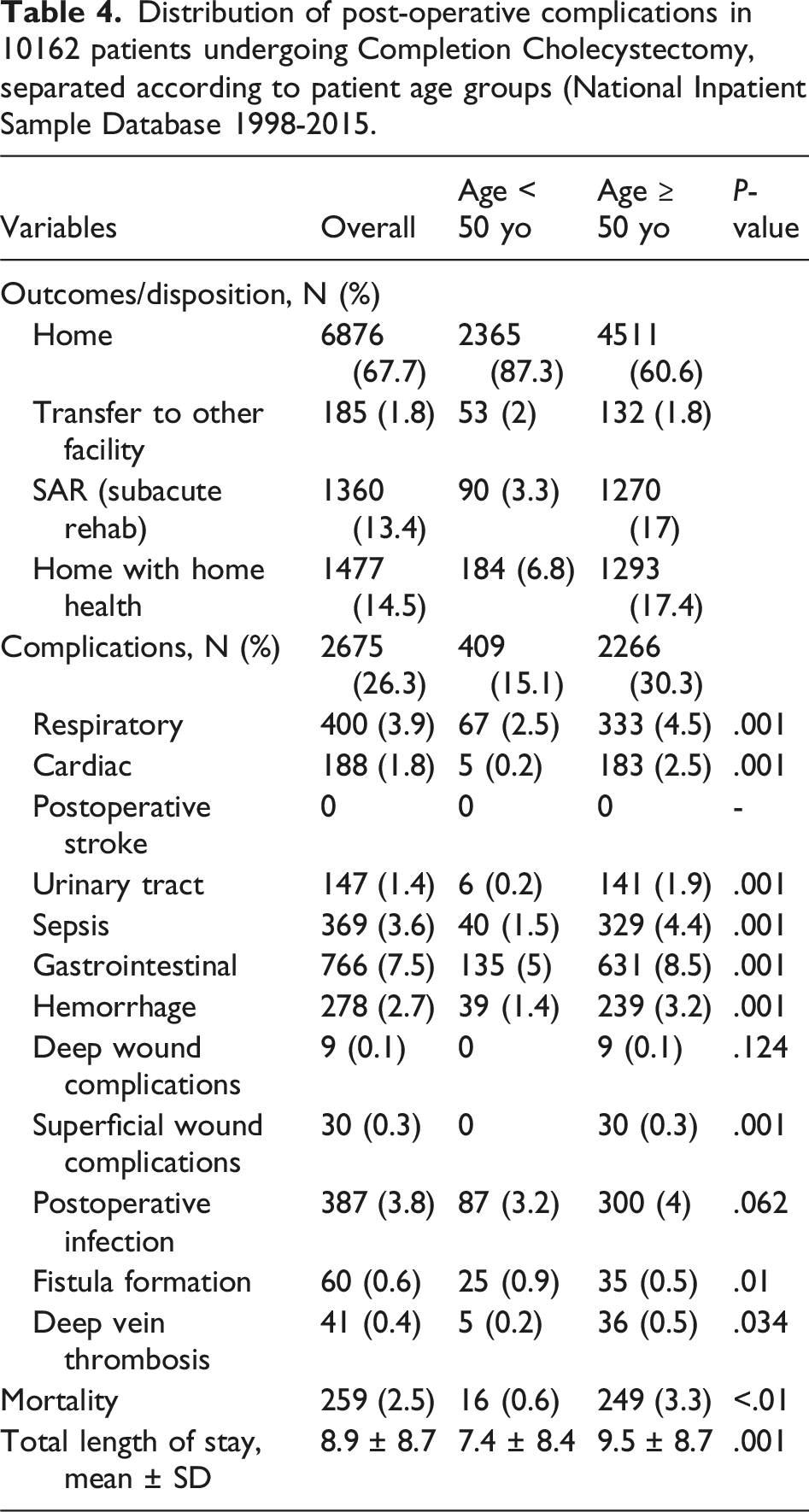
Older patients demonstrated significantly higher comorbidity burdens, as reflected by Charlson Comorbidity Index scores. Overall complication rates were substantial (26.3%), including gastrointestinal, infectious, and cardiopulmonary events. Mortality was 2.5% overall but markedly higher in patients aged ≥50 years (3.3% vs 0.6%). Length of stay was also longer in older patients.
Conclusions
Worse outcomes in older individuals correlated strongly with increased comorbidities rather than age alone. Completion cholecystectomy is frequently performed in complex surgical settings with distorted anatomy, contributing to higher complication rates. However, variability in outcomes across studies suggests that patient selection, operative approach, and baseline health status are key determinants. The study highlights the diagnostic challenge of post-subtotal cholecystectomy cholecystitis and underscores the importance of clinical vigilance. It concludes that careful preoperative risk stratification and patient selection are critical to improving outcomes, as procedural risk is closely tied to underlying health status and case complexity rather than the surgery itself.
Key Takeaways
• Cholecystitis after a partial cholecystectomy is a rare condition and may be difficult to diagnose due to a low initial index of suspicion. • Patients undergoing completion cholecystectomy who have a higher comorbidity burden, more commonly observed in those aged ≥50 years, experience increased morbidity and mortality, suggesting that baseline health status plays a significant role in outcomes. • Completion cholecystectomy is frequently performed in complex clinical settings and is associated with notable complication rates; however, these outcomes appear closely linked to underlying patient risk profiles and case complexity rather than the procedure alone.
Introduction
Acute cholecystitis refers to an inflammation of the gallbladder caused by obstruction of a cystic duct by a gallstone. Approximately 1-4% of the Western population is affected by symptomatic cholelithiasis annually, and 10-15% will experience it during their lifetime. 1 Cholecystectomy is considered a “gold standard” treatment for symptomatic gallstone disease.
In some patients, especially those with multiple prior episodes of inflammation, triangle of Calot’s is too difficult for comfortable and safe dissection. In such cases, a partial cholecystectomy should be considered. Gadiyaram et al reported that 8% of open and 3.3% of laparoscopic cholecystectomies were partial cholecystectomies. 2 Additionally, Ramirez-Giraldo et al reported that partial cholecystectomies accounted for 4-9% of all cholecystectomies performed. 3
Methods
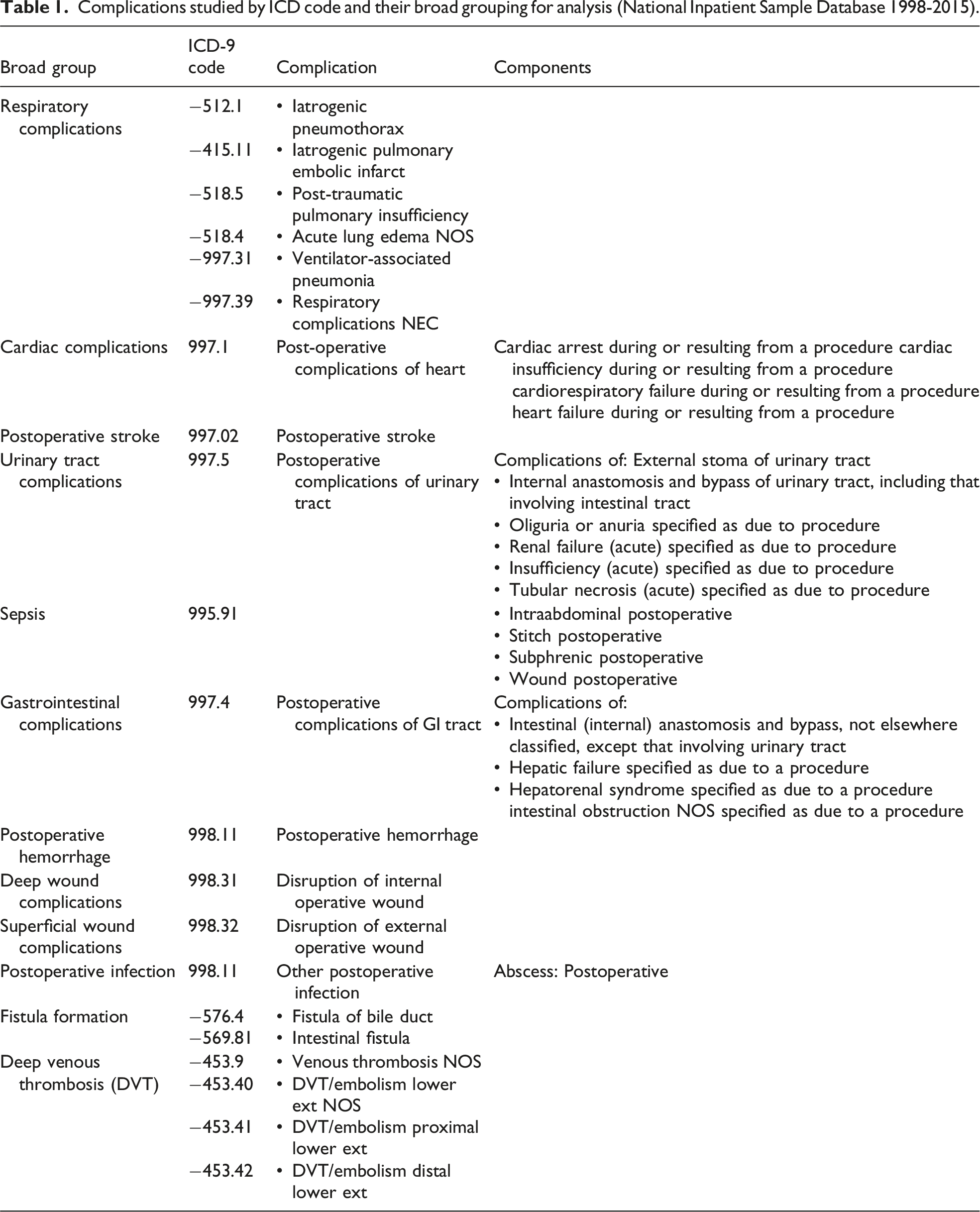
Complications studied by ICD code and their broad grouping for analysis (National Inpatient Sample Database 1998-2015).
Results
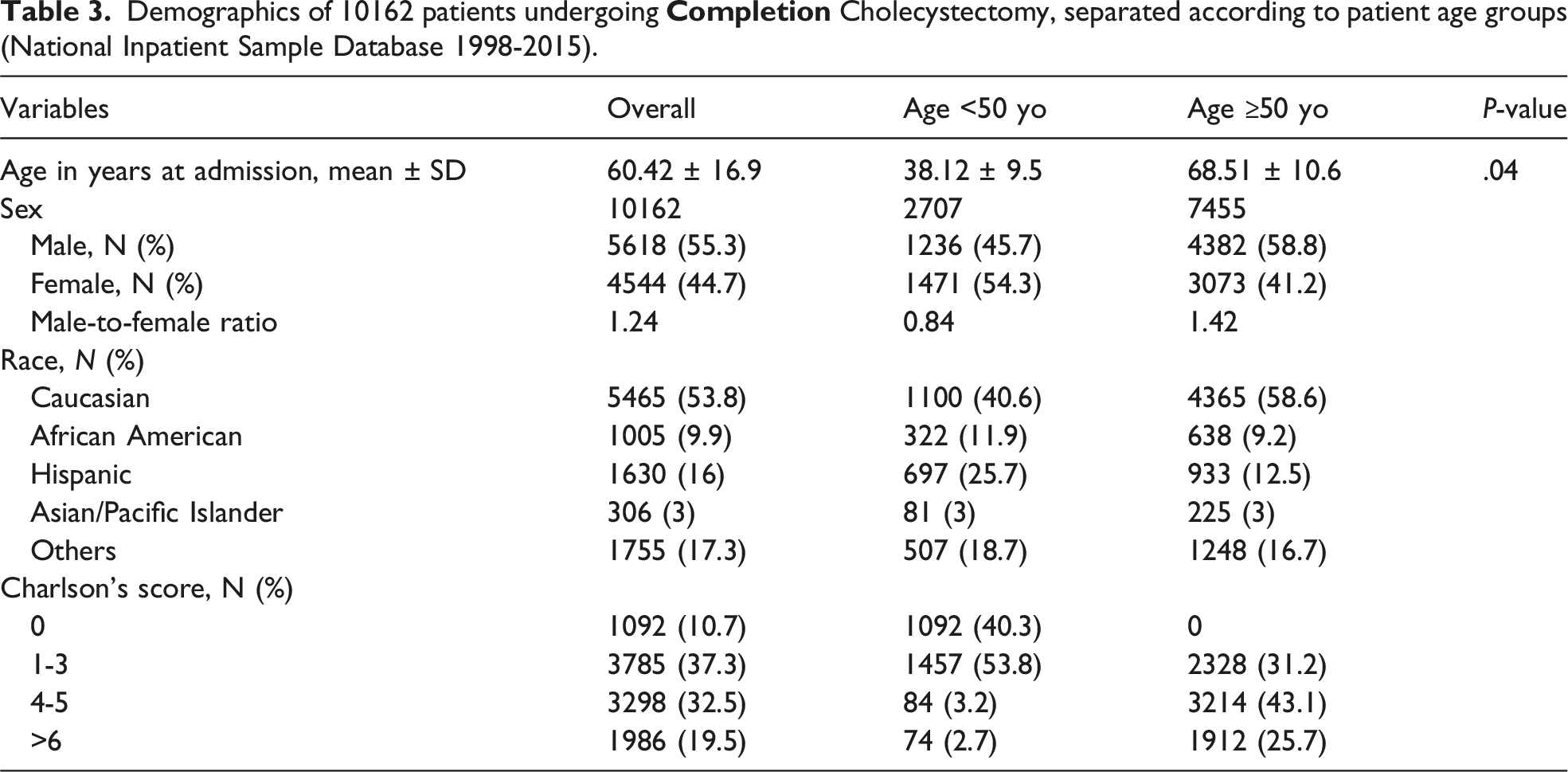
Between 1998 and 2015, a total of 1 423 080 laparoscopic cholecystectomies were performed in the United States. The exact number of partial cholecystectomies could not be determined; however, it is estimated to fall between 42 600 and 128 000. A total of 10 162 patients who underwent completion cholecystectomy were identified in the NIS database. The average age at admission was 60.4 ± 16.9 years. The male-to-female ratio was 1.24:1 (5618 males and 4544 females).
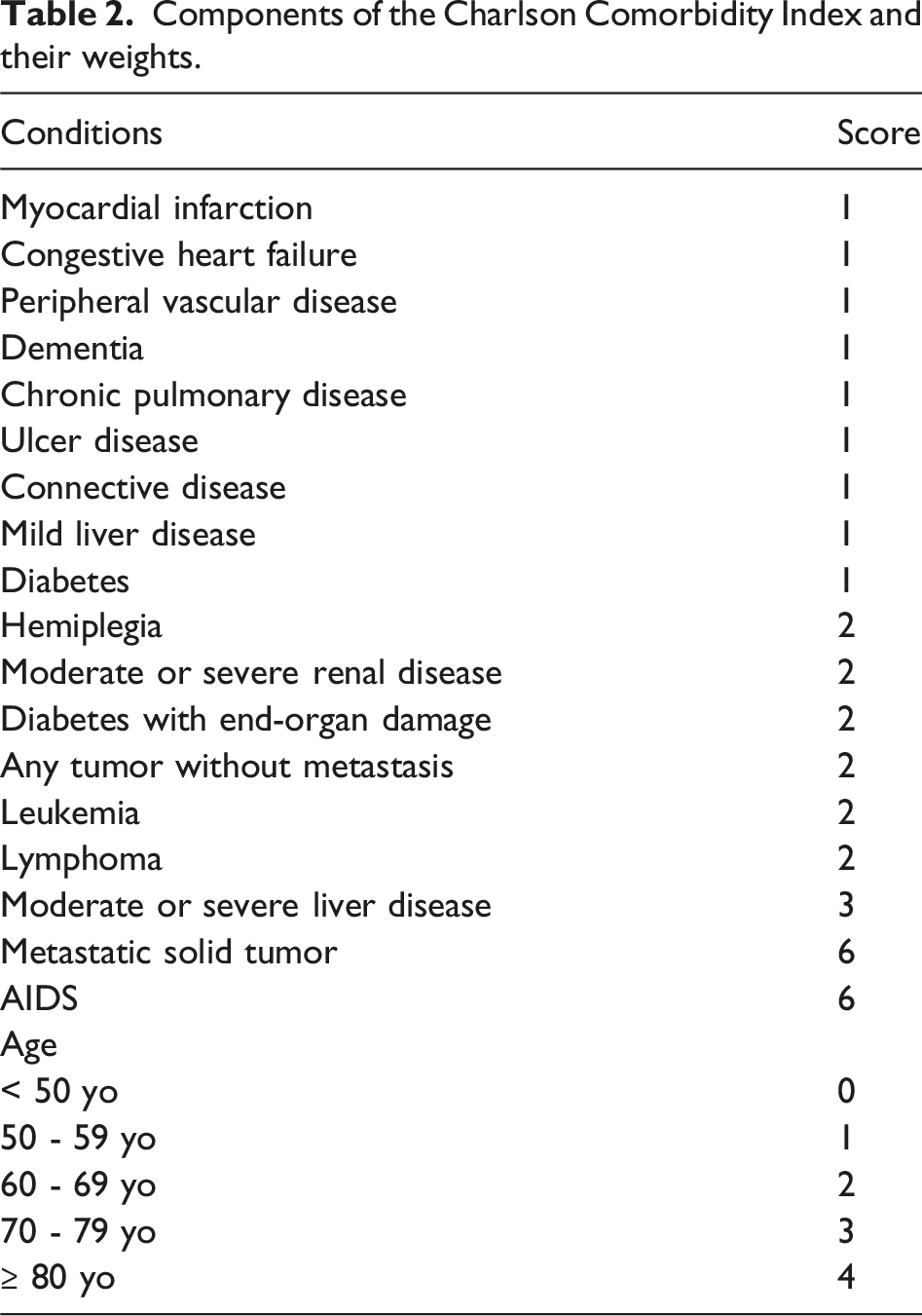
Components of the Charlson Comorbidity Index and their weights.
Demographics of 10162 patients undergoing
Discussion
Anatomical visualization during laparoscopic cholecystectomy may be difficult, especially in patients with recurrent inflammation or extensive surgical history, where adhesions obscure Calot’s triangle. The Nassar grading scale can assist in evaluating technical difficulty. When the critical view of safety, first described by Strasberg et al in 1995 1 , cannot be safely achieved, a bailout technique should be used. The two most commonly used methods are the fundus-first approach and subtotal cholecystectomy. Strasberg et al described two main techniques of partial cholecystectomy: reconstituting and fenestrating. The reconstituting technique involves closing the remnant gallbladder, which decreases postoperative fistula risk but increases the risk of recurrent cholecystitis. The fenestrating technique leaves the remnant open, increasing the risk of bile leak and fistula formation. 1 Patients who undergo a subtotal cholecystectomy remain at future risk for recurrent cholecystitis, potentially requiring completion cholecystectomy. Motter et al reported similar rates of completion cholecystectomy in both groups (2.58% for fenestrating vs. 2.92% for reconstituting). 4
Cholecystitis after partial cholecystectomy is rare and may be challenging to diagnose because of a low initial index of suspicion. Physicians should remain vigilant, especially in patients with a history of subtotal cholecystectomy. Common presenting symptoms include abdominal pain, jaundice, and dyspepsia. 5 Gadiyaram et al reported multiple diagnostic modalities, including ultrasound, MRCP, and CT, that can be used to confirm diagnosis. 2 Alser et al speculated that a gallbladder remnant larger than 2.5 cm increases the likelihood of requiring completion cholecystectomy. 6
Distribution of post-operative complications in 10162 patients undergoing Completion Cholecystectomy, separated according to patient age groups (National Inpatient Sample Database 1998-2015.
In this study, a substantially greater proportion of patients aged ≥50 years had higher Charlson scores compared to younger patients. The observed differences in morbidity and mortality between age groups paralleled this distribution of comorbidity burden, suggesting that baseline health status, rather than age in isolation, may be a key contributor to outcomes. Stefanova et al reported a median Charlson score of 1.9 among patients undergoing robotic completion cholecystectomy, with 36.4% having a score ≥3. 7 This may suggest that healthier patients are more often selected for minimally invasive procedures, potentially influencing morbidity, mortality, and LOS.
Nafea et al described a shorter length of stay with laparoscopic vs open completion cholecystectomy (1 day vs 2 days). 5 Alser et al reported a median length of stay of 3 days for laparoscopic and laparoscopic converted to open cases combined, 6 while Stefanova et al reported a median of 1 day. 7 In contrast, the mean length of stay in our study was 8.9 days, which is much higher than reported in the two aforementioned studies. This could be reflective of older data availability in our study (1998-2015), when minimally invasive approaches were less frequently used for complex cases, but could also be reflecting case selection bias, or differences in coding between various institutions.
Completion cholecystectomy is associated with high complication rates due to the hostile right upper quadrant anatomy that prompted partial cholecystectomy in the first place. In this study, complications occurred in 26.3% of patients. Stefanova et al reported a complication rate of 6.8% after robotic completion cholecystectomy. 7 Alser et al observed a complication rate of 27.3% (three patients), including one patient that experienced a wound infection. 6 Wound infections were the only complications being analyzed in the study by Nafea et al, where they reported an incidence of 20% in the group undergoing open surgery, compared to none in laparoscopic arm. 4 Wound infections were reported infrequently in our study (0.4%). The complexity of cases and the underlying risk profile of the patient population may attribute the variation in complication rates across studies. This may also be attributable, at least in part, to differences in patient selection, comorbidity burden, and operative approach rather than the procedure itself.
Limitations
Although the use of a nationwide database can give useful insights into a large population of patients, it also introduces limitations. A key limitation of this study lies in the inherent constraints of the Nationwide Inpatient Sample (NIS) database. The NIS lacks procedural granularity, precluding differentiation between open, laparoscopic, and robotic approaches to completion cholecystectomy, which may carry distinct risk profiles and outcomes. Additionally, the database does not capture the specific clinical indication for surgery, limiting the ability to distinguish cases performed for stump cholecystitis from those undertaken for other biliary pathologies. Furthermore, reliance on ICD-9 coding introduces the possibility of misclassification, particularly in accurately identifying true cases of “completion cholecystectomy” vs other biliary interventions. Finally, the NIS captures only inpatient data, thereby restricting analysis to in-hospital outcomes and preventing assessment of long-term complications, readmissions, or longitudinal patient trajectories.
Conclusions
Cholecystitis after partial cholecystectomy remains a rare and diagnostically challenging condition due to low clinical suspicion. Completion cholecystectomy is often undertaken in technically complex scenarios characterized by inflammation, adhesions, and altered anatomy. While higher complication rates and worse outcomes were observed in older patients, these differences are more appropriately interpreted in the context of increased comorbidity burden and overall baseline risk rather than age alone.
The findings of this study highlight the importance of careful patient selection and preoperative risk stratification, as outcomes following completion cholecystectomy appear to be strongly influenced by underlying health status and disease complexity. Future studies should focus on refining risk assessment models and optimizing selection criteria to improve patient outcomes, rather than attributing causation primarily to the procedure itself.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.