
Abstract
Background
Trauma patients are at high risk of developing psychiatric disorders such as Post-Traumatic Stress Disorder (PTSD) and depression. The Injured Trauma Survivor Screen (ITSS) is a validated tool designed to identify trauma patients at risk, facilitating early psychiatric intervention. However, there is limited information on the types of psychiatric recommendations given following positive screenings. This study compares the frequency of positive ITSS and treatment recommendations between blunt and penetrating trauma at a Level 1 urban center.
Methods
We conducted a retrospective chart review of trauma patients (n = 727) screened with the ITSS between August 2023-July 2024. Data was extracted including demographics, trauma mechanism, ITSS screen result (positive/negative), positive result (PTSD, depression, or both), personal psychiatric history, and psychiatric recommendations following positive screenings (psychotherapy, medications, inpatient psychiatric transfer, or no intervention) Descriptive statistics were used to analyze the frequency of each recommendation and compare blunt and penetrating mechanisms.
Results
Of the 727 patients screened, 46% screened positive for either PTSD or depression. Among those who screened positive, 65% were seen by psychiatry. The most common recommendations were psychotherapy (64%) and pharmacotherapy (50%). Penetrating trauma had more positive screens (69%), but no difference in psychiatry consultations or recommendations.
Discussion
This study highlights the current practices in psychiatric recommendations for trauma survivors and underscores the importance of early identification using tools like ITSS. Patients with penetrating trauma or those screening positive for PTSD may represent a unique subset that has specific needs for follow-up.
Keywords
Key Takeaways
• Mental health screening is a key component of post-traumatic recovery to identify those at risk of depression and post-traumatic stress disorder. • Psychiatry consultations were obtained and frequently recommended psychotherapy or pharmacotherapy.
Introduction
In the United States, approximately 2.8 million individuals per year experience traumatic injuries requiring hospitalization at a designated trauma center. 1 Trauma survivors are at an increased risk of negative health consequences, including psychological harm. Psychological well-being is a critical aspect of health-related quality of life (HRQoL), a multidimensional concept used to assess how disease and treatment impact overall function and well-being. 2 Mental health outcomes, particularly the development of post-traumatic stress disorder (PTSD) and depression, are among the strongest correlates of poor post-injury HRQoL, with 21% of trauma patients developing chronic PTSD and about 6% developing depression within 12 months of injury. 3 Timely screening and intervention for PTSD and depression can significantly improve health outcomes and quality of life in this high-risk population. Despite the clear need for mental health support, screening for these conditions remains insufficient. In 2014, less than 25% of patients were screened for depression and only 7% for PTSD across Level I and II Trauma Centers in the U.S. 4 As a result, up to 90% of individuals with PTSD or depression symptoms go without adequate care. 5 In response to these alarming statistics, the American College of Surgeons (ACS) published new guidelines in December 2022 requiring Level I and II Trauma Centers to implement protocols for screening high-risk patients and referring them to mental health providers. 6
The Injured Trauma Survivor Screen (ITSS) is a 9-item screening tool to predict the development of PTSD and depression in trauma patients. A score of 2 or higher in either subset indicates a positive screen for PTSD and/or depression. 7 The ITSS can be rapidly administered by any member of the trauma team including social workers, nurses, medical students, residents, and advanced practice providers in 5 minutes. The sensitive nature of the tool, approximately 75%, paired with its ease of administration allows for the identification of at-risk patients and the initiation of treatment. 7
Given the recency of the ACS’s screening mandate, there is limited research on psychiatric recommendations following positive mental health screenings. Furthermore, there is a lack of consistency among trauma centers when responding to positive screenings, which highlights a critical gap in trauma care. This study compares the frequency of positive ITSS assessments and treatment recommendations between traumatic mechanisms at an urban Level 1 trauma center. We hypothesize that penetrating trauma patients will have higher frequency of positive screenings and therapeutic intervention by psychiatry.
Methods
This was a retrospective chart review of adult and pediatric trauma patients admitted to the study hospital between August 1, 2023 and July 31, 2024, who received an inpatient social services consult for mental health screening using the ITSS. The hospital is an ACS-verified and state-designated Level I Adult and Level II Pediatric Trauma Center.
Inclusion and Exclusion Criteria
Inclusion criteria for ITSS screening were age 7 years or older, admitted to the trauma service for at least 48 h, had a Glasgow Coma Scale (GCS) score of 15, or at the provider’s discretion. Patients having self-inflicted injuries, intellectual or cognitive impairments, GCS less than 15, ground-level falls, or enrollment in the G-60 geriatric pathway (age greater than 60 with an isolated femur fracture) were excluded. During this initial year of mental health screening, all patients (adult and pediatric) were screened with the ITSS using the same inclusion and exclusion criteria.
Screening Protocol
For patients meeting the inclusion criteria, a consult was placed into the electronic medical record (Epic) for “Inpatient consult to Social Services for Mental Health Screen for Trauma Patients.” A first attempt at screening eligible patients occurred on hospital day 2 or upon downgrade from the intensive care unit. A social worker conducted the 9-item ITSS questionnaire which evaluates the patient’s subjective experience before, during and after the traumatic event. From the nine yes or no questions, 5 are scored for PTSD and 5 for depression with one overlapping item. A score of 2 or higher indicates a positive screen for PTSD and/or depression. 7 Patients who screened positive were offered resources regarding the Trauma Survivors Network and a psychiatry consult. If the patient accepted a psychiatry referral, a formal consultation was made with the inpatient psychiatry service. For patients under 18, the screening was completed at a similar timepoint (hospital day 2 or upon downgrade from ICU) by a pediatric social worker and positive screens were referred to the child and adolescent psychiatry service.
Data was abstracted from the electronic medical record of trauma patients who had an ITSS ordered. Demographics included age, sex, trauma category (blunt or penetrating), and mechanism. Mental health screening data included: ITSS results (positive or negative for PTSD and depression); whether the patient accepted and received an inpatient psychiatric consultation; and psychiatric recommendations made (pharmacotherapy, psychotherapy, combined pharmacotherapy and psychotherapy, inpatient psychiatric transfer, or no intervention). Psychotherapy included both supportive therapy while inpatient or a referral to continue as an outpatient. Pharmacotherapy was defined as any medication recommendation: initiation of an inpatient regimen only, modification of home medications, or a new discharge prescription. Transfer to an inpatient psychiatry facility, as well as mental health holds and safety sitters were executed when recommended.
Statistical analysis was performed with Stata version 14 (College Station, TX). As trauma mechanism was the primary variable of interest, adult and pediatric data was pooled for analysis. Descriptive statistics were used to calculate the frequency and percentages of positive ITSS screenings; the proportion of psychiatric consultations; the frequency and distribution of types of psychiatric recommendations; and the percentage of discharge documentation containing follow-up instructions. This study was approved by the Institutional Review Board at the study hospital (UMC-2024-556). All data was de-identified following collection to maintain confidentiality in accordance with the approved protocol.
Results
Demographics
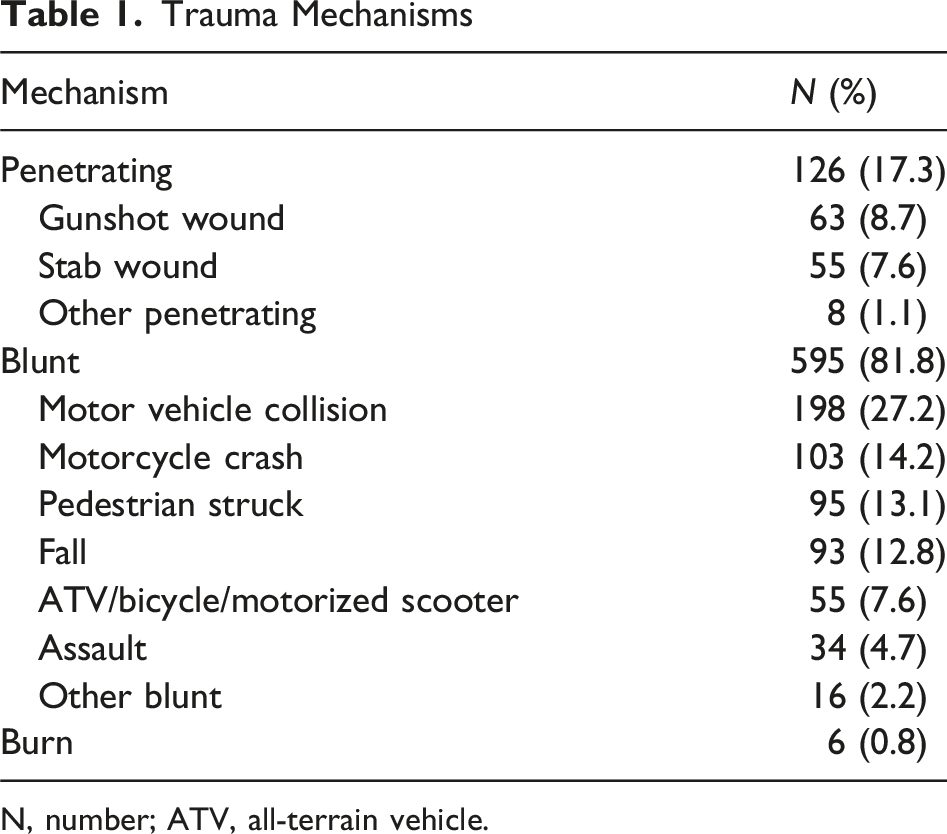
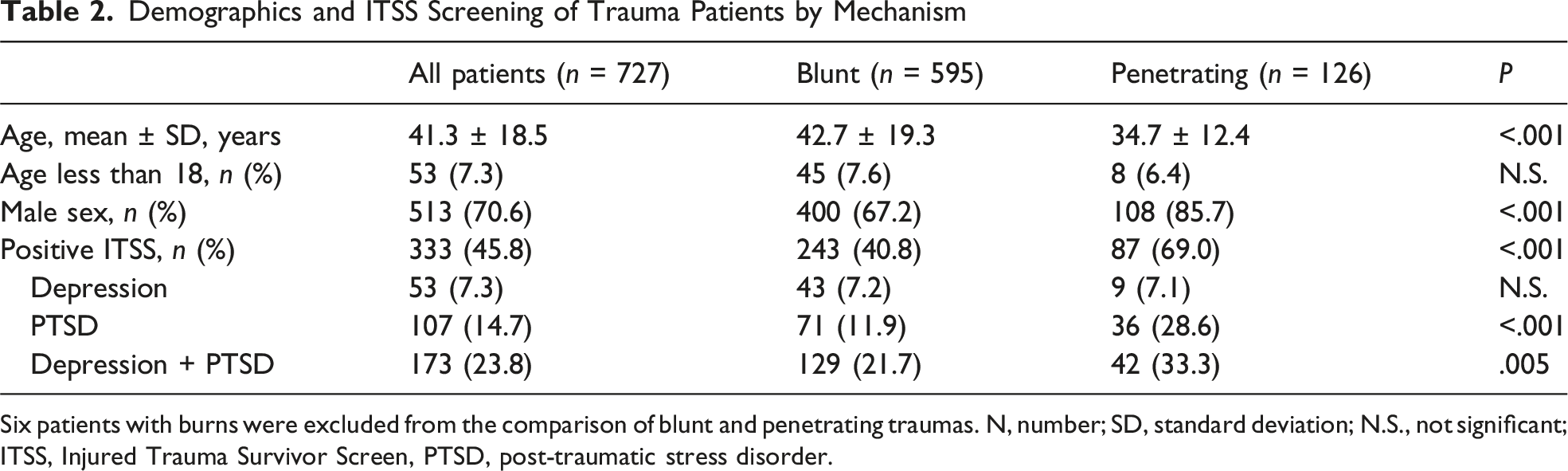
Of 2218 eligible trauma admissions during the study year, 797 (35.9%) were ordered for ITSS screening based on the inclusion criteria. Seventy patients were excluded from analysis (incomplete screening, missing documentation, duplicates) leaving a study cohort of 727 with a screening completion rate of 91.2% (Figure 1). The mean age of the group was 41.3 ± 18.5 years (range 6-91), with 513 males (513/727, 70.6%). Fifty-three patients (53/727, 7.3%) were less than 18 years of age. Most patients had blunt trauma (595/727, 81.8%), with smaller numbers of penetrating injuries (126/727, 17.3%) and burns (6/727, 0.8%). The most common mechanisms were motor vehicle collisions (198/727, 27.2%), motorcycle crashes (103/727, 14.2%), and pedestrians struck by vehicles (95/727, 13.1%) (Table 1). Penetrating trauma patients were younger (mean age 34.7 vs 42.7, P < .001) and more likely to be male (85.7% vs 67.2%, P < .001) (Table 2). Flow diagram of patients included in the study. ITSS, Injured Trauma Survivor Screen, PTSD, post-traumatic stress disorder Trauma Mechanisms N, number; ATV, all-terrain vehicle. Demographics and ITSS Screening of Trauma Patients by Mechanism Six patients with burns were excluded from the comparison of blunt and penetrating traumas. N, number; SD, standard deviation; N.S., not significant; ITSS, Injured Trauma Survivor Screen, PTSD, post-traumatic stress disorder.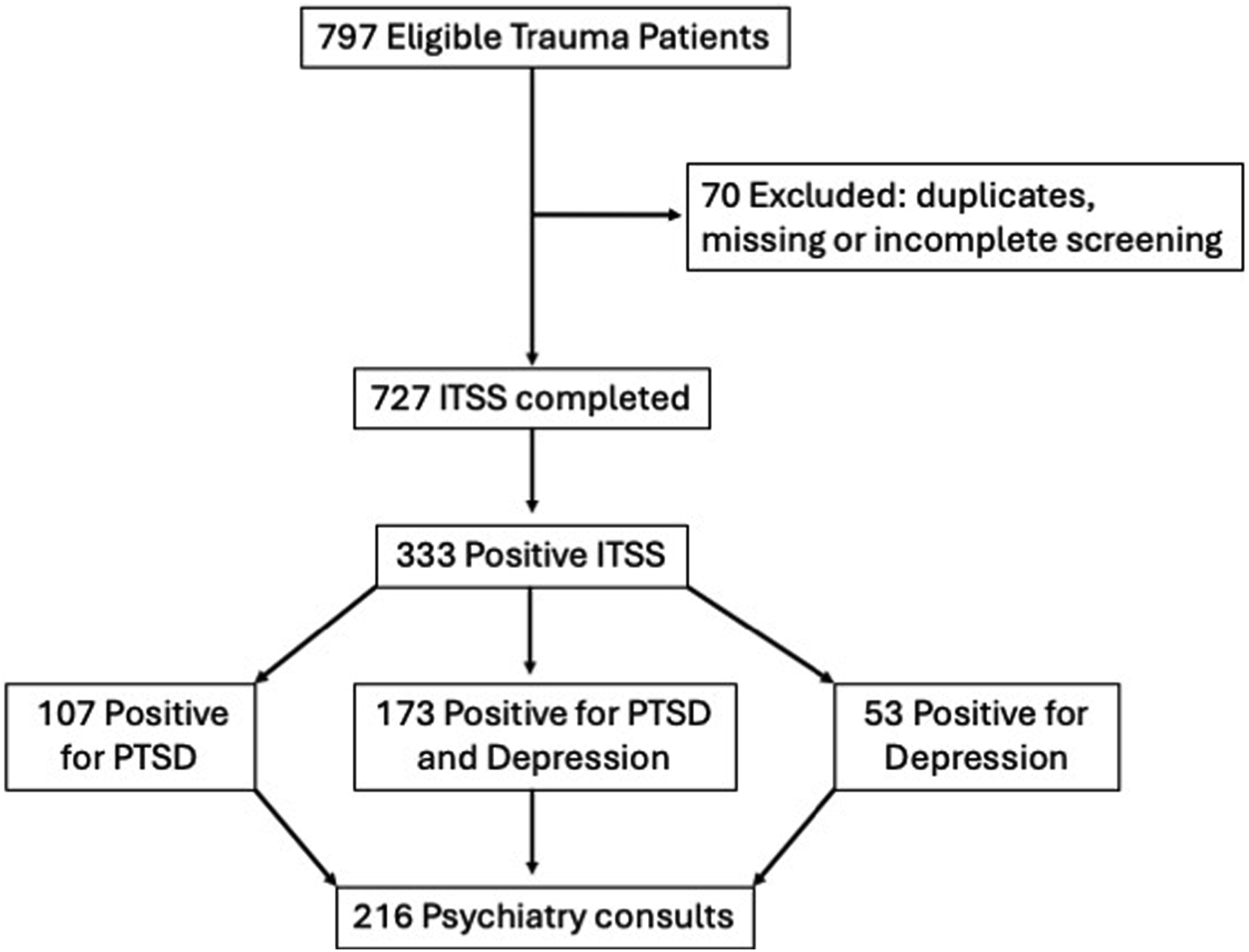
Screening Results
Three hundred thirty-three (333/727, 45.8%) patients had a positive ITSS, with 23.8% (173/727) screening positive for both PTSD and depression, 14.7% (107/727) for PTSD only, and 7.3% (53/727) for depression only. Patients with penetrating trauma had an overall higher frequency of positive ITSS screens (69% vs 40.8%, P < .001) than blunt trauma. Penetrating trauma exhibited a higher frequency of positive screens for PTSD (28.6% vs 11.9% blunt trauma, P < .001) and PTSD plus depression (33.3% vs 21.7%, P = .005) (Table 2).
Intervention
Comparison of Psychiatric Consultation and Recommendations Between Blunt and Penetrating Trauma
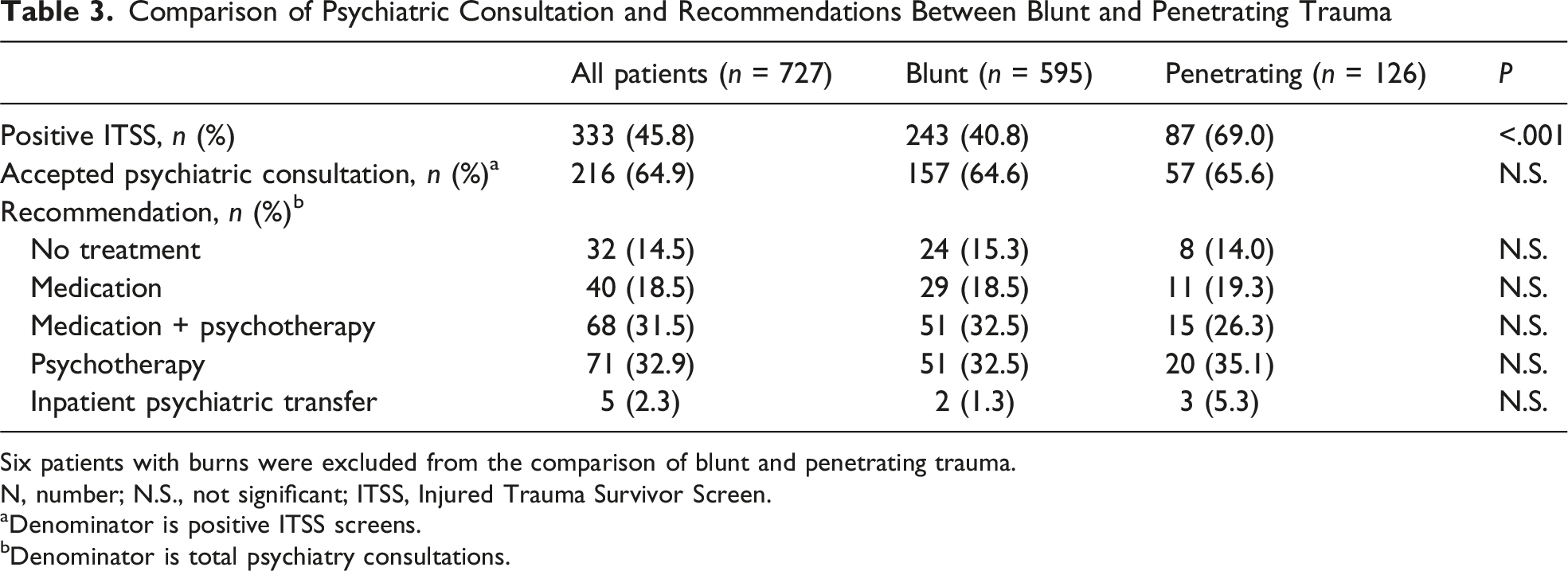
Six patients with burns were excluded from the comparison of blunt and penetrating trauma.
N, number; N.S., not significant; ITSS, Injured Trauma Survivor Screen.
aDenominator is positive ITSS screens.
bDenominator is total psychiatry consultations.
Comparison of Psychiatric Consultation and Recommendations Between ITSS Positive Groups
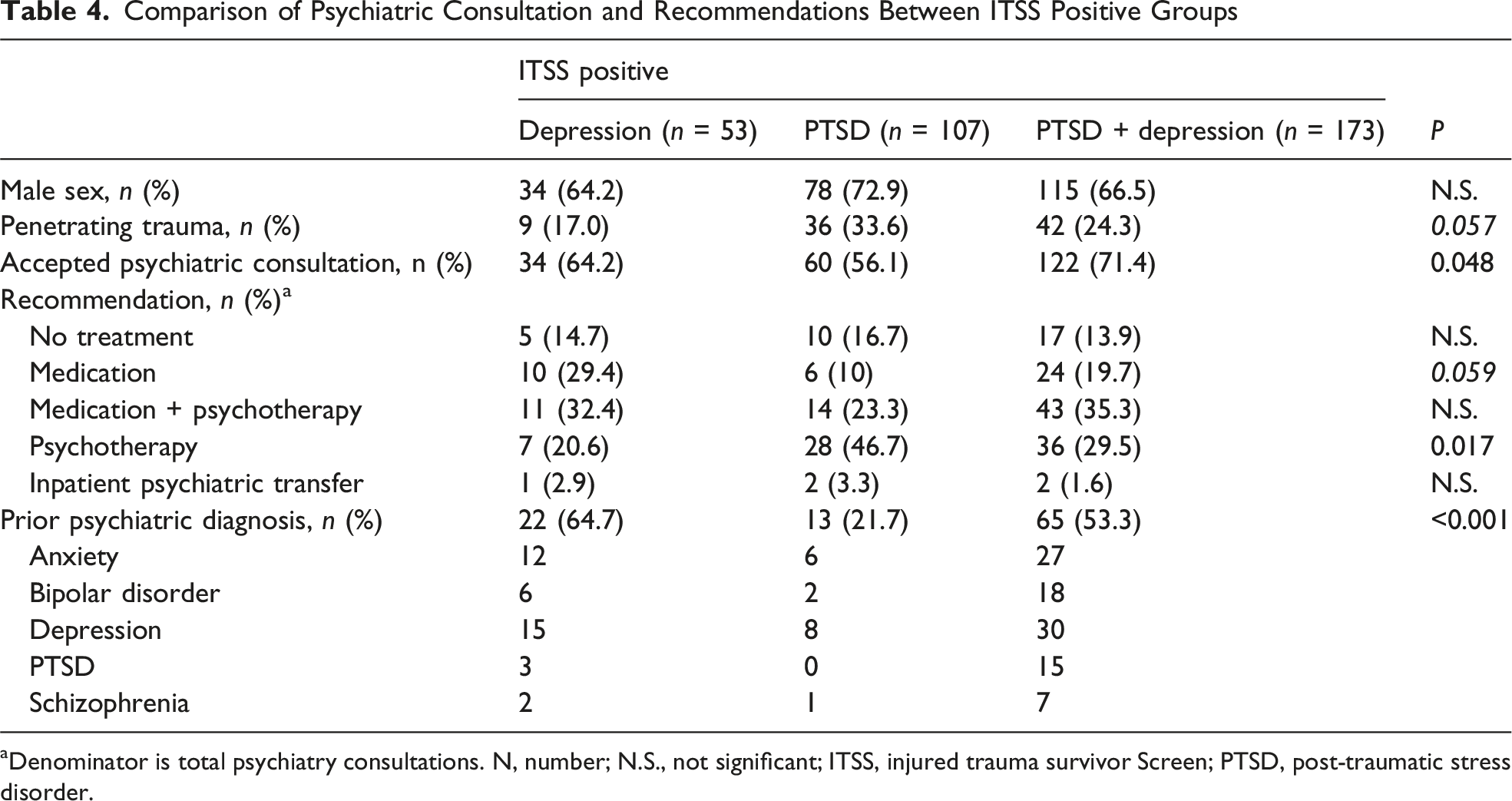
aDenominator is total psychiatry consultations. N, number; N.S., not significant; ITSS, injured trauma survivor Screen; PTSD, post-traumatic stress disorder.
Pediatric Patients
The cohort included 53 patients less than 18 years of age; however, only 19 were less 15 years of age (ACS definition of pediatric trauma patients). Penetrating trauma occurred in 8 of 53 patients (15.1%). Thirty-two (60.4%) have positive ITSS screens with 16 (50%) positive for both PTSD and depression, 3 (9.4%) for depression, and 13 (40.6%) for PTSD. Child and adolescent psychiatry consults were obtained in 20/32 (62.5%), with psychotherapy recommended in 19/20 (95%) and medication in 8/20 (40%).
Discussion
This study evaluated the first-year use of the ITSS tool at a combined adult and pediatric trauma center, with specific attention to differences between trauma mechanisms in the screening positivity and treatment recommendations provided by psychiatry. Of our 727 patients screened, 46% had a positive result, with the majority positive for both PTSD and depression.
Screening for post-traumatic mental health conditions remains challenging but required for trauma centers based on the 2022 update of the American College of Surgeons’ Resources for Optimal Care of the Injured Patient. 6 Recently, the Eastern Association for the Surgery of Trauma (EAST) published a systematic review of PTSD mitigation in trauma and conditionally recommended for screening adult trauma patients during their initial hospitalization. 8 There are many instruments available, which vary in predictive accuracy and functionality in follow-up, although questionnaire-based tools appear to perform better. 9 The Injured Trauma Survivor Screen was first described in 2017, as a brief screening tool to identify trauma survivors at risk for PTSD and depression. 7 In a multicenter longitudinal validation study, the screening tool had a sensitivity of 75.0% and 72.7% for PTSD, and 80.4% and 76.1% for depression during acute and chronic follow-up time points, respectively. 10 Additional work has demonstrated that the ITSS is sufficient to use as a standalone instrument with a positive cutoff of 2 or more for both depression and PTSD. 11
Trauma patients are at a high risk for negative mental health outcomes after injury, which may be under-identified by clinicians. DeRoon-Cassini et al found that 21% of trauma patients developed chronic PTSD and 6% developed depression within 12 months of injury. 3 In a similar research study, Bell et al found that 72% of patients screened positive for depression and 47% screened positive for PTSD at some point in a 12-month post-injury period. 12 This cohort falls in between these two prior results, with 39% of patients screening positive for PTSD and 31% screening positive for depression during their hospitalization. The subset with penetrating trauma (17% of the cohort) had higher rates of positive screening for both depression (40%) and PTSD (62%) compared to blunt mechanisms. Existing literature on outcomes of firearm violence demonstrated elevated risk of both PTSD and depression along with decreased physical functioning at post-hospital follow-up. 13
The second part of the American College of Surgeons mandate for mental health screening 6 is having a “means of referral should a problem or risk be identified during inpatient admission.” Of the group with a positive ITSS, 65% accepted a consultation with our inpatient psychiatry service who recommended supportive psychotherapy in 64% and pharmacotherapy in 50%. Interestingly, a similar screening initiative at a rural Northwest Level II trauma center yielded an 11% rate for inpatient psychiatric consultations, possibly reflecting a difference in the trauma populations. 14 Our overall positive screening rate of 46% in an urban cohort was higher than this rural center’s (30.9-35.7%) as well as a higher percentage of penetrating trauma (17% vs 7%). The authors note a significant lack of access to inpatient psychiatric providers and follow-up resources as a barrier to their care of post-traumatic mental health issues. 14 The provided psychiatric recommendations align with established best practices, as psychotherapy is consistently endorsed as a first-line treatment for PTSD. Techniques such as cognitive behavioral therapy directly address maladaptive thought patterns and provides patients with tools to manage distressing symptoms. 15 The systematic review by EAST strongly recommends cognitive behavioral therapy to decrease the development of PTSD in trauma patients. 8 Many guidelines also support pharmacological interventions, most often in the form of selective serotonin reuptake inhibitors (SSRIs), which work to regulate serotonin levels to alleviate anxiety and depressive symptoms. A meta-analysis of complex trauma intervention suggests that psychological treatment is more effective than pharmacologic in the treatment of PTSD symptoms and improving sleep. 16 Similarly, the American Psychological Association guidelines for treating depression supports the use of psychotherapy and/or pharmacotherapy. 17
This project has several limitations, including its retrospective study design and missing data in the electronic health record. Although the rate of screening was like a previous report, 14 it was impossible to determine the rate of missed screening vs not meeting the inclusion criteria. Information regarding prior mental health diagnoses or medications was inconsistent due to self-reporting. This institution has a robust cadre of inpatient social workers and mental health professionals for both adult and pediatrics, which may not be replicated at other facilities. However, the hospital does not have a comprehensive post-discharge clinic for trauma patients and existing mental health resources are not integrated into the county health system; thus, it was not possible to track outpatient referrals, follow-though with psychiatric recommendations, and long-term mental health outcomes. Our audit of mental health follow-up documentation in the discharge instruction was low (49%), yielding a clear opportunity for improvement. Compliance with documentation was confounded by the psychiatry team frequently providing paper pamphlets, which could not be tracked in the electronic medical record. We are developing processes to improve consistency of follow-up documentation and ensure appointments are scheduled prior to discharge. Since initiating our screening protocol, we have learned that the ITSS is not a validated screening tool in children. Subsequently, we have transitioned to the Child Trauma Screening Questionnaire (CTSQ), a validated tool for the pediatric population. For this transition, the new protocol was distributed to the key stakeholders, including trauma surgeons, pediatric intensivists, pediatric hospitalists, pediatric social workers, and the child and adolescent psychiatry service. The inclusion criteria and screening procedure for pediatrics remained the same and was audited during the transition by the Pediatric Trauma Program Manager. In 2024, the adult inclusion criteria have been expanded to include geriatric ground-level falls, as it is recognized that depressive symptoms are associated with a higher risk of mortality in geriatric hip fracture patients. 18
In conclusion, this study provides valuable insights into the rate of positive screenings for PTSD and depression in an urban cohort of trauma patients, with 46% screening positive, and the subsequent psychiatric recommendations. We found that psychotherapy and pharmacotherapy were the most frequently recommended interventions, aligning with established best practices for treating PTSD and depression. Not surprisingly, patients with penetrating injuries had higher rates of positive screening for both PTSD and depression than those with blunt trauma. Further work should improve longitudinal re-screening and care of mental health conditions to optimize post-traumatic recovery.
Footnotes
Acknowledgments
The authors would like to thank the University Medical Center Trauma Program and Registrars for their contribution to this work, especially Lisa Rogge, Trauma Program Manager and Robert McClaren, Lead Trauma Registrar.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.