
Abstract
This systematic review aimed to evaluate and compare the short- and long-term outcomes of different treatment strategies for patients with colorectal adenocarcinoma presenting with synchronous liver metastases. A comprehensive literature search was conducted in PubMed (MEDLINE), Cochrane Central Register of Controlled Trials (CENTRAL), Embase, Ovid, and ScienceDirect to identify relevant studies assessing surgical sequencing strategies in patients without extrahepatic disease. Data were extracted and analyzed using Review Manager software. Pooled dichotomous outcomes were expressed as odds ratios (ORs) with 95% confidence intervals (CIs), while continuous outcomes were reported as mean differences (MDs) with corresponding 95% CIs. Three treatment strategies were evaluated: the classical “colon-first” approach, the “liver-first” approach, and the simultaneous resection approach. Overall survival (OS) at 1, 3, and 5 years was the primary outcome. The pooled results demonstrated no statistically significant differences in survival outcomes among the three strategies. When compared with the colon-first approach, simultaneous resection showed comparable 1-year (90.1% vs 87.9%), 3-year (66.5% vs 56.2%), and 5-year survival rates (48% vs 40.7%). Similarly, comparisons between colon-first and liver-first approaches revealed no significant differences in 1-, 3-, or 5-year overall survival. These findings indicate that no single surgical sequencing strategy confers a clear survival advantage. Accordingly, treatment decisions should be individualized, taking into account patient characteristics, hepatic tumor burden, primary tumor features, and institutional expertise within a multidisciplinary framework. Further high-quality randomized controlled trials are needed to better define optimal management strategies for this complex and heterogeneous patient population.
Introduction
Colorectal adenocarcinoma (CRC) is defined as cancer arising from glandular tissue of the large intestine from the cecum to the rectum. According to latest Global Cancer Observatory (GLOBOCAN) reports, CRC is the 3rd most prevalent form of cancer and is the 2nd most common cause of cancer related deaths worldwide. 1
The reliance of the large bowel on the portal system for venous drainage has led to the liver being the first and most common site for metastatic disease with up to 25-30% of patients developing liver metastasis during the course of their disease. 2 Diagnosis of metastatic disease is best established by axial imaging such as contrast enhanced computed tomography (CT) or Magnetic Resonance Imaging (MRI).
Liver metastases are described as either synchronous, that is, diagnosed before or with the primary tumor, or metachronous, that is, diagnosed 6 months or more after primary removal. The importance of this classification lies in the poorer prognosis, and its implications on choice of further treatment in patients with synchronous metastatic disease. 3
Surgical resection represents the only treatment modality aiming at cure for metastatic colorectal cancer. Classically patients with synchronous liver metastases without extrahepatic disease undergo colonic resection for primary tumor, followed by a course of chemotherapy. Hepatectomy was then only considered in patients who showed no disease progression. Rationale of this approach was to avoid complications related to primary tumor, such as bleeding, obstruction or perforation, and by elimination of primary source to slow progression of metastatic disease. 4 This approach had a 5-year Overall Survival (OS) rate of 53% and a 5-year Disease Free Survival (DFS) of 10%. 5 However, studies over the past years have demonstrated that only a small percentage of patients with asymptomatic lesions suffer any primary related complications. Furthermore, studies comparing patients with similar metastatic tumor burden suggest no benefit of primary resection on long-term survival. Another proposed disadvantage of this regimen is delay in initiation of systemic therapy in form of chemotherapy, especially if complications related to colorectal surgery should arise. 4
In view of controversy surrounding traditional strategy to treatment of colorectal cancer with synchronous liver metastasis, a new strategy was proposed called: liver-first approach. This involves resection of liver metastasis, with or without neoadjuvant chemotherapy, followed by adjuvant systemic chemotherapy and later resection of primary colon tumor. Main advantages of this approach are avoiding postponing liver resection which could lead to disease progression beyond respectability, as well as early administration of systemic chemotherapy. 6 This method had 5-year OS rate of 36% and 5-year DFS of 9%. 5
Another seemingly attractive option is simultaneous resection of both lesions in same session. Proposed advantages of this procedure are removal of all macroscopic lesions and initiation of systemic chemotherapy with minimal delay, as well as single hospital admission and single dose of general anesthetic. 7 Yet, this approach has been argued to be associated with increased morbidity and risk of post-operative complications making it only available for a highly select cohort of patients 6 simultaneous strategy had 5-year OS of 63% and 5-year DFS of 28%. 5
Due to the lack of consensus regarding the optimum sequence for resection in CRC patients with synchronous liver metastasis, a systemic review and meta-analysis of literature comparing different modalities was conducted.
Methods
The current study was designed and performed according to the protocol agreed by all participating authors and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 8 The study was conducted over the period September 2023 to June 2024.
Database Search
A systematic review of literature was conducted in the following databases: PubMed (Medline), Cochrane Central Register of Controlled Studies (CENTRAL), Embase, Ovid, and Science Direct for articles on the management of patients with CRC suffering synchronous liver metastasis without extrahepatic disease using “classical” colon-first strategy, “reverse” liver-first strategy and simultaneous resection. Articles published from the year 2000-2023 were included with the last search conducted in August 2023. Search was conducted according to the strategy used by Gumiero et al 9 using the following key words: (colectomy) OR (colectomies) OR (hemicolectomy) OR (hemicolectomies) OR (large bowel resection) OR (colon resection) OR (proctocolectomy) OR (coloproctectomy) OR (rectosigmoidectomy) OR (sigmoidectomy) AND (rectal cancer)) AND (colorectal) OR (rectal) OR (rectum) OR (colon) AND (cancer) OR (neoplasm) OR (tumor) OR (adenocarcinoma) OR (carcinoma) AND (Liver-first) OR (colon-first) OR (simultaneous) OR (synchronous) OR (staged) OR (delayed).
Subsequently search was repeated using keywords used in the metanalysis conducted by Kelly et al 7 : “colorectal liver metastasis surgery,” “resectable synchronous colorectal liver metastasis,” “synchronous colorectal liver metastasis surgery,” “liver first approach surgery synchronous colorectal liver metastasis,” “staged surgery synchronous colorectal liver metastasis,” and “combined surgery synchronous colorectal liver metastasis.”
Study Selection
Three reviewers conducted the search and subsequently study selection based on previously defined inclusion and exclusion criteria.
Inclusion criteria were articles written in English, published between 2000 and 2023, conducted on human participants including patients with CRC and isolated synchronous liver metastasis.
Exclusion criteria were animal trials, articles published in language other than English, abstracts, letters to editors, systematic review and meta-analysis, patients with metachronous metastatic liver disease, and patients with extrahepatic metastatic disease at time of diagnosis.
Records were imported to EndNote Desktop Software, 21.2 Version (EndNote, 2024 Clarivate Philadelphia, PA), which was used for managing the records, as well as in-text citations and creating bibliography though its Cite-While-You-Write (CWYW) tool. Using the advanced search tools of EndNote, duplicates (232 records) and non-English (399) records were identified and removed from the library before screening.
Outcomes
Primary outcomes included OS 1, 3-, and 5-year survival in each modality. Secondary outcome parameters in each modality included perioperative morbidity, operative time, blood loss, length of hospital stay, and 30-day postoperative mortality.
Statistical Analysis
We analyzed data from the included studies using Review Manager (RevMan – version 5.4.1, The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark, 2021). A formal meta-analysis was conducted for all outcomes if the data were sufficient. We expressed pooled dichotomous data as odds ratio (OR) with the 95% confidence intervals (95%CI); while pooled continuous effect measures was expressed as the mean difference (MD) with 95%CI. For studies reporting mean and interquartile range (IQR), we estimated the SD by dividing the IQR by 1.35 (Cochrane handbook of systematic reviews of interventions, version 6.2, 2021). For one study reported the mean and standard error (SE), we calculated the SD by the equation SD = SE × SQRT (n); where “n” is the group size. We explored and quantified between-study statistical heterogeneity using the I2 test. By default, we used the fixed effect model in all analyses. If heterogeneity was statistically significant (P < 0.05) or I2 was >50%, we used the Der Simonian and Laird random-effects model instead. 10 We considered 2-sided statistical analysis testing setting the α-error level at 0.05.
Results
Database Searching and Screening
Initial search of the aforementioned data bases using agreed keywords yielded 3722 articles. After excluding irrelevant records according to inclusion and exclusion criteria, only 26 records had survival data comparing different treatment modalities, which matched the intended primary outcome of this metanalysis and were therefore included.11-36 Studies included observational studies, matched observational studies, one randomized controlled trial. Three reports compared all surgical strategies; colon first, liver first, and simultaneous resection, four reports compared colon first to liver first, and the remaining 19 articles compared colon first to simultaneous resection (Figure 1). PRISMA flow diagram for searching and screening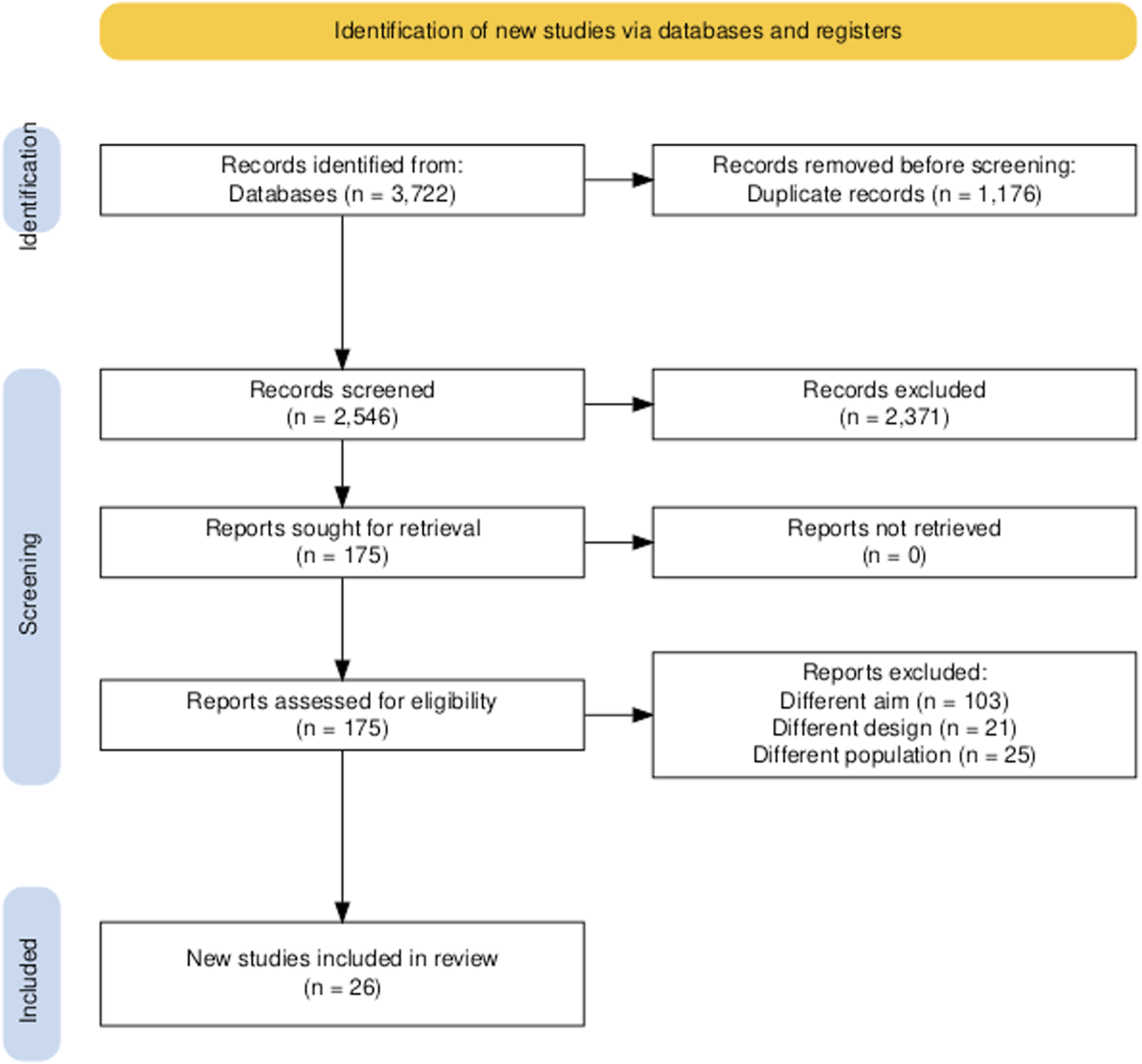
Baseline Characteristics
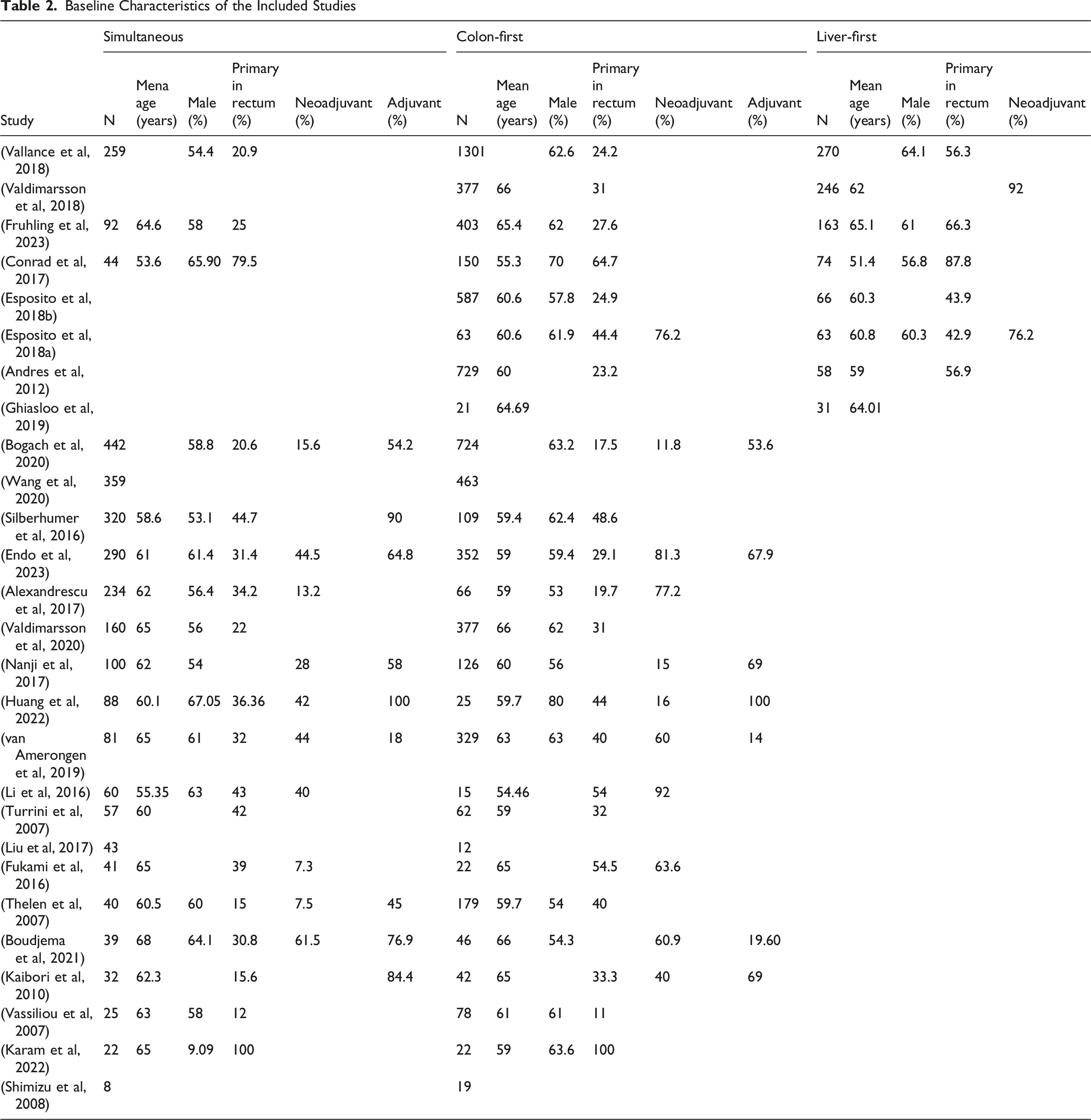
Analysis was performed on 10 644 patients, of which 6699 underwent bowel-first (classical) strategy, 971 had Liver-first (reversed) approach, 2974 underwent simultaneous resections. Age and gender distribution was found to be similar in different strategies, with a male predominance, percentage exceeding 50% in all included records, and a population age ranging between 50 and 70 years of age. Patients subjected to Liver first approach were more likely to have rectal primaries, representing almost half the population in most reports, whereas percentage of rectal primaries were lower in both colon-first and simultaneous groups, reaching as low as 11% in some studies in simultaneous approach, and 12% in colon-first group.
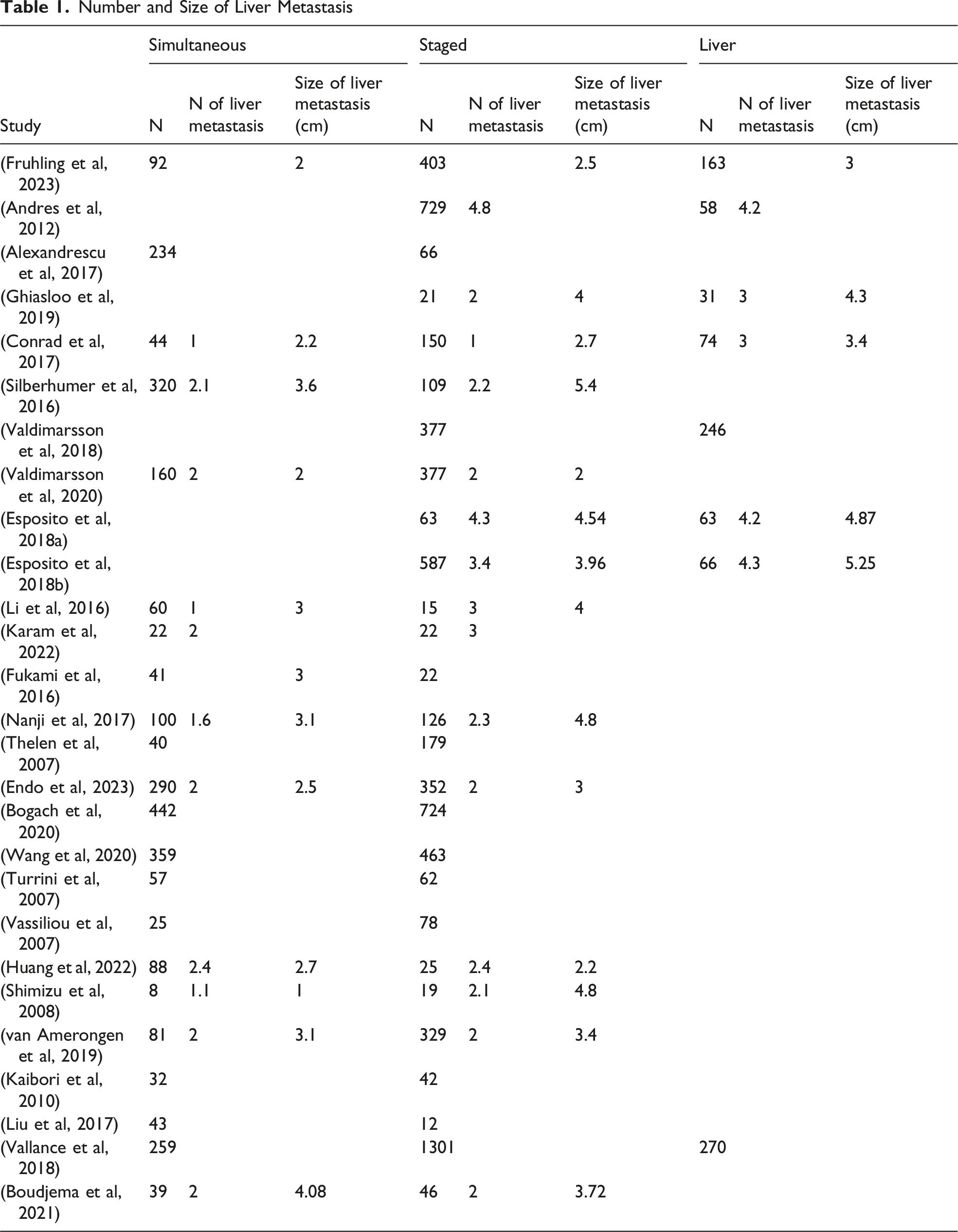
Number and Size of Liver Metastasis
Protocols for neoadjuvant and adjuvant chemotherapy showed immense variation, two studies out of 4 on liver-first approach reported chemotherapeutic administration, 92% of participants receiving neoadjuvant chemotherapy in one, and 76% in the other. Rates of chemotherapy use in the other two study groups was similar with a slightly higher tendency toward adjuvant chemotherapy use in simultaneous approach, where only 7 studies administered adjuvant treatment in colon first group, compared to 9 studies in the simultaneous group.
Baseline Characteristics of the Included Studies
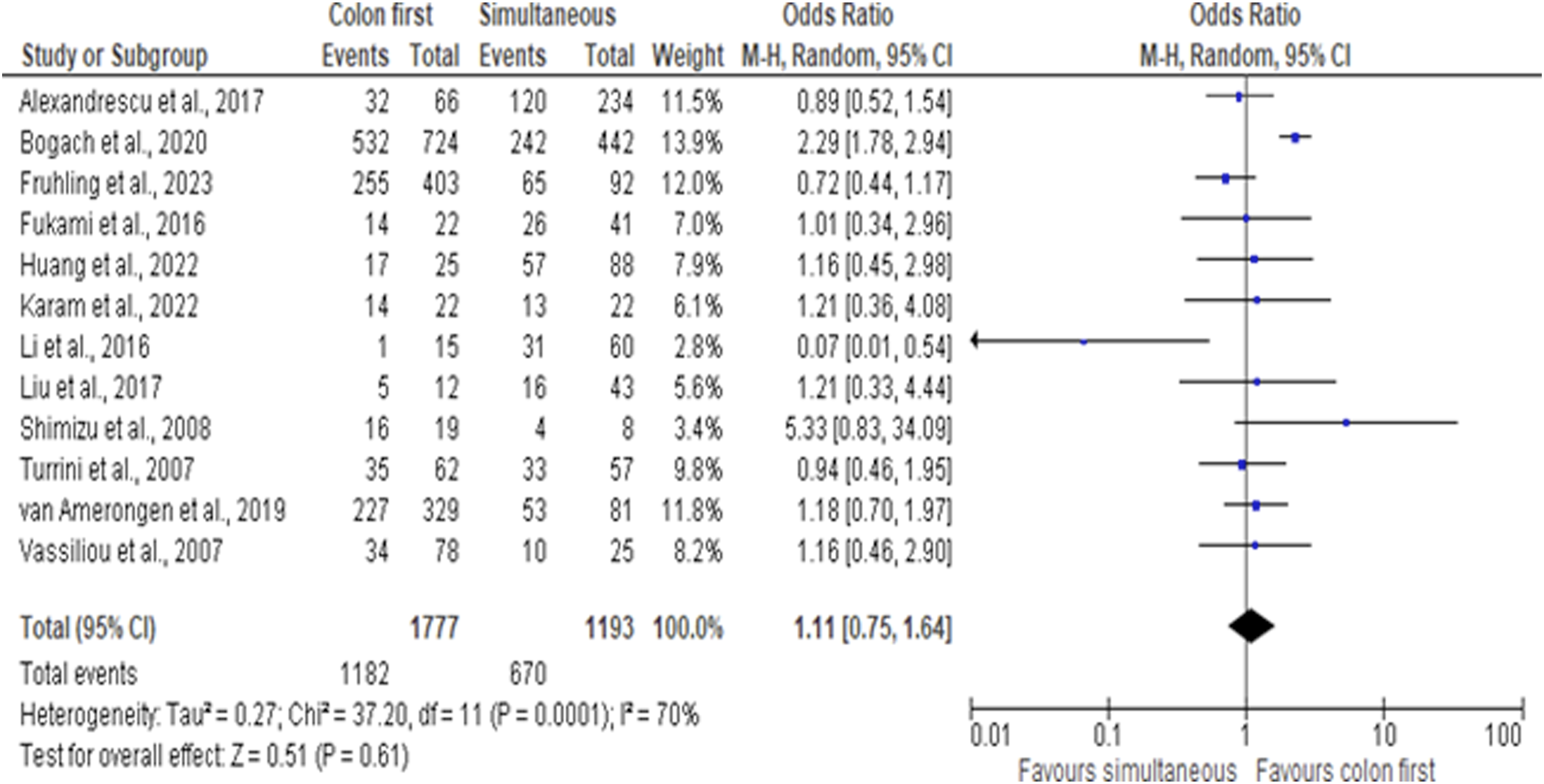
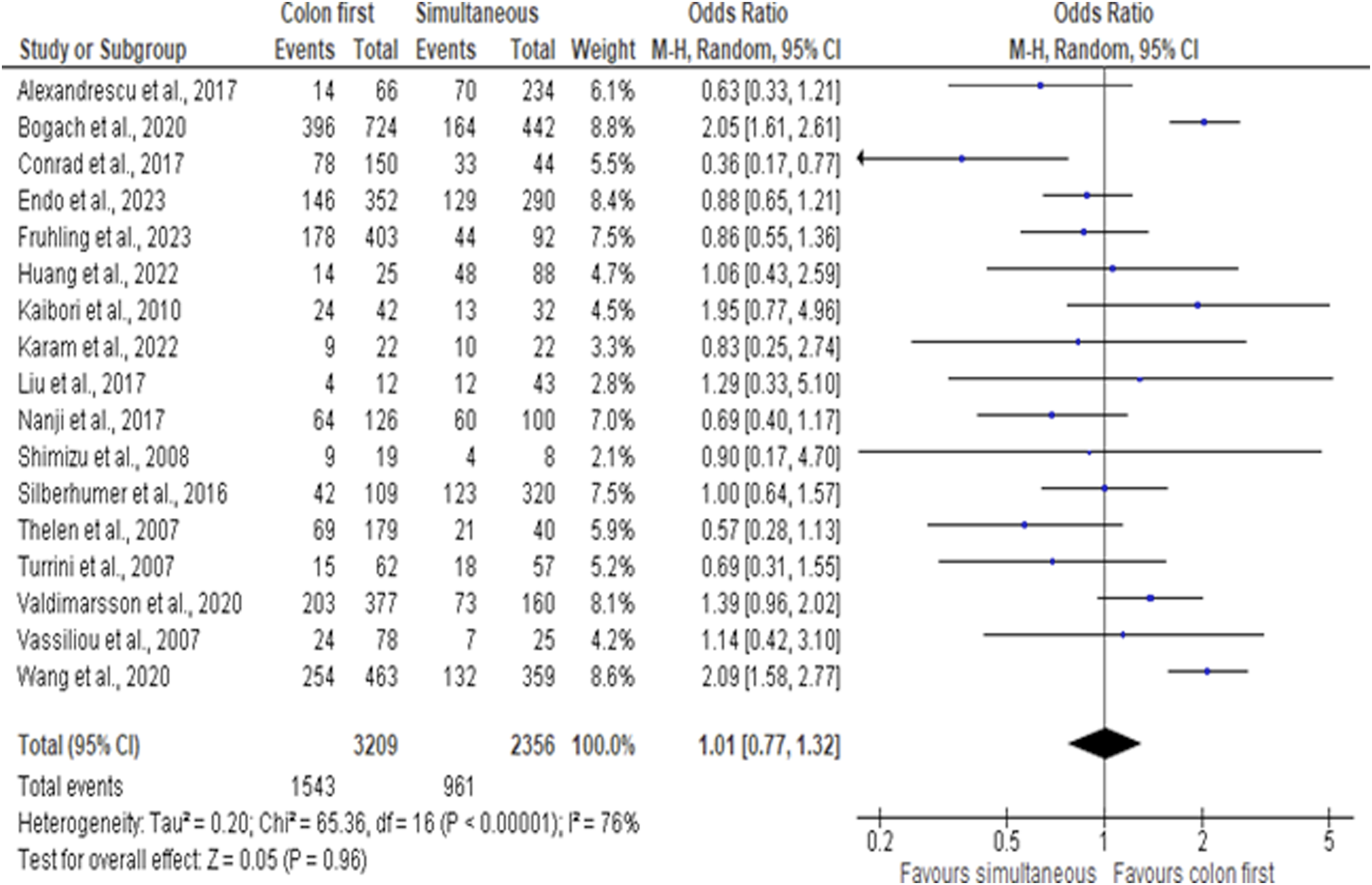
Metanalysis of survival outcomes of the three treatment modalities showed no statistically significant difference in 1, 3- and 5-year OS rates. Considering colon first the “classical” approach, this group was used as a reference for pair-wise comparison of different modalities. Data was unfortunately insufficient to compare liver first with simultaneous group.
Colon first vs simultaneous 1-year OS was 90.1% vs 87.9% (OR 1.14, 95%CI: 0.81, 1.61), 3-year OS: 66.5% vs 56.2% (OR 1.11, 95%CI 0.75, 1.64), 5-year OS 48% vs 40.7% (OR 1.11, 95%CI: 0.77, 1.32) (Figures 2-4). 1y OS colon first vs simultaneous 3y OS colon first vs simultaneous 5y OS colon first vs simultaneous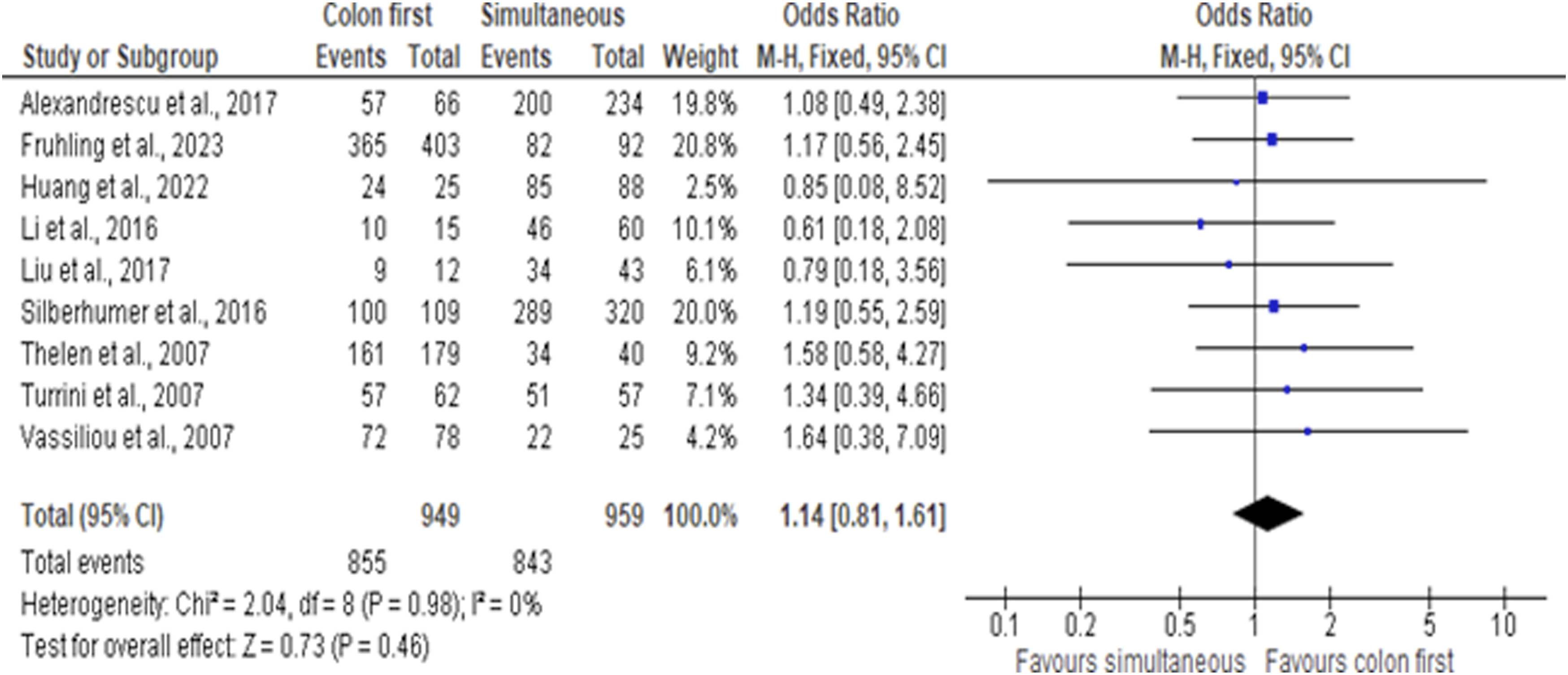
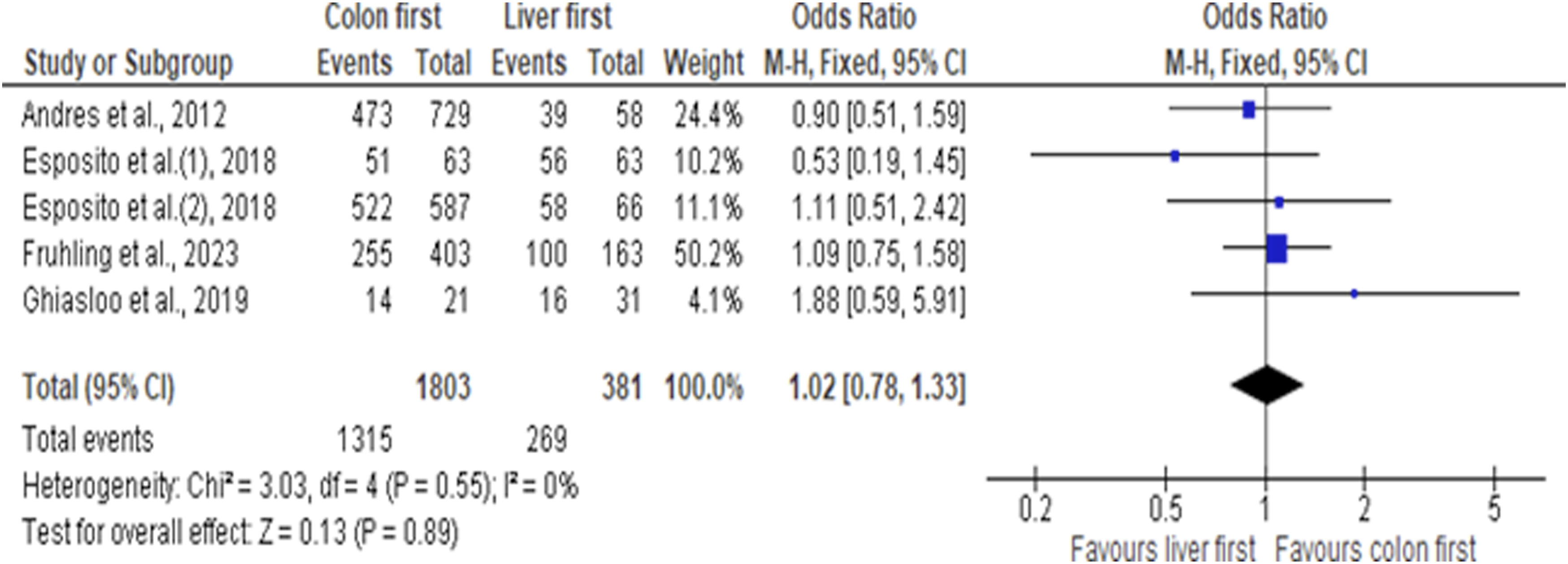
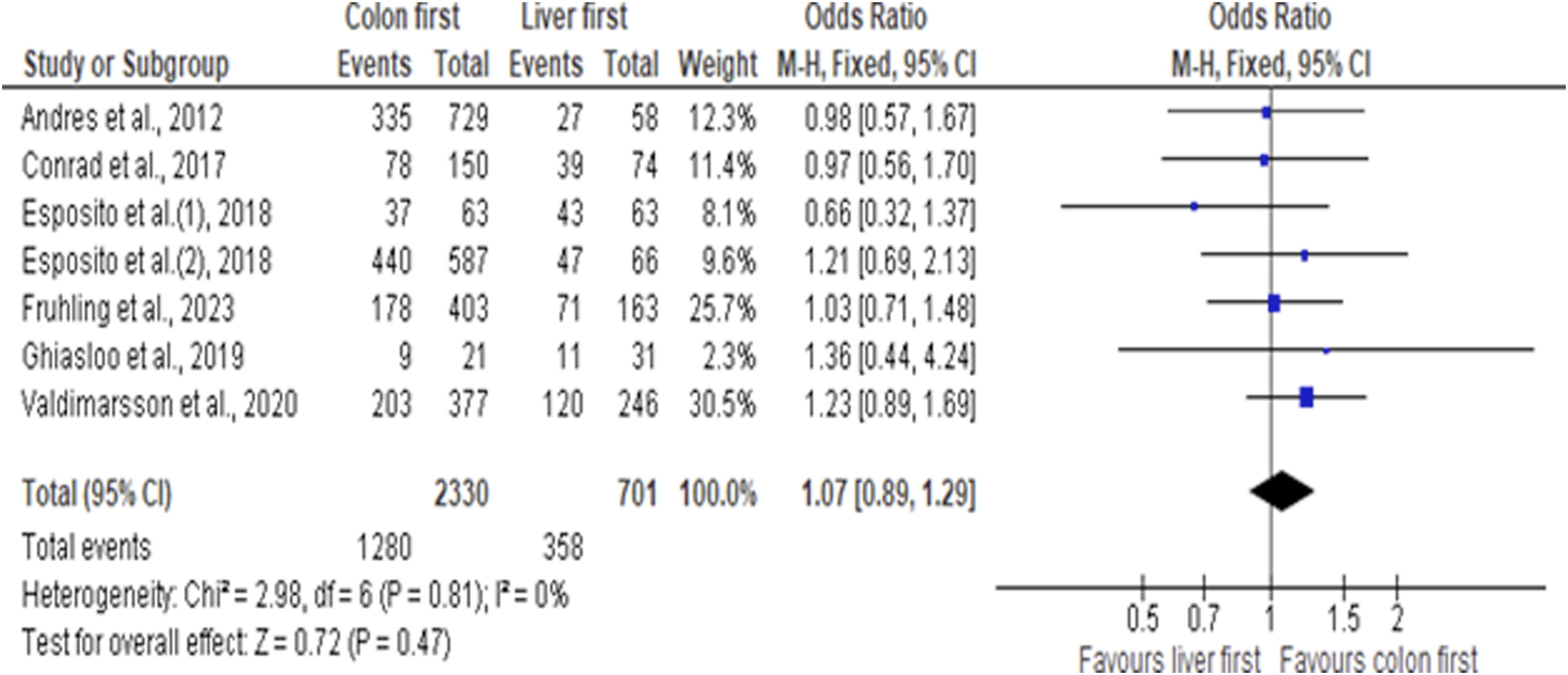
Colon first vs liver first 1-year OS 94% vs 93% (OR 1.0. 95%CI 0.62, 1.60), 3-year OS 72% vs 70% (OR 1.02, 95%CI 0.78, 1.33), 5-year OS 55% vs 51% (OR 1.07, 95%CI 0.89, 1.29) (Figures 5-7). 1y OS colon first vs liver first 3y OS colon first vs liver first 5y OS colon first vs liver first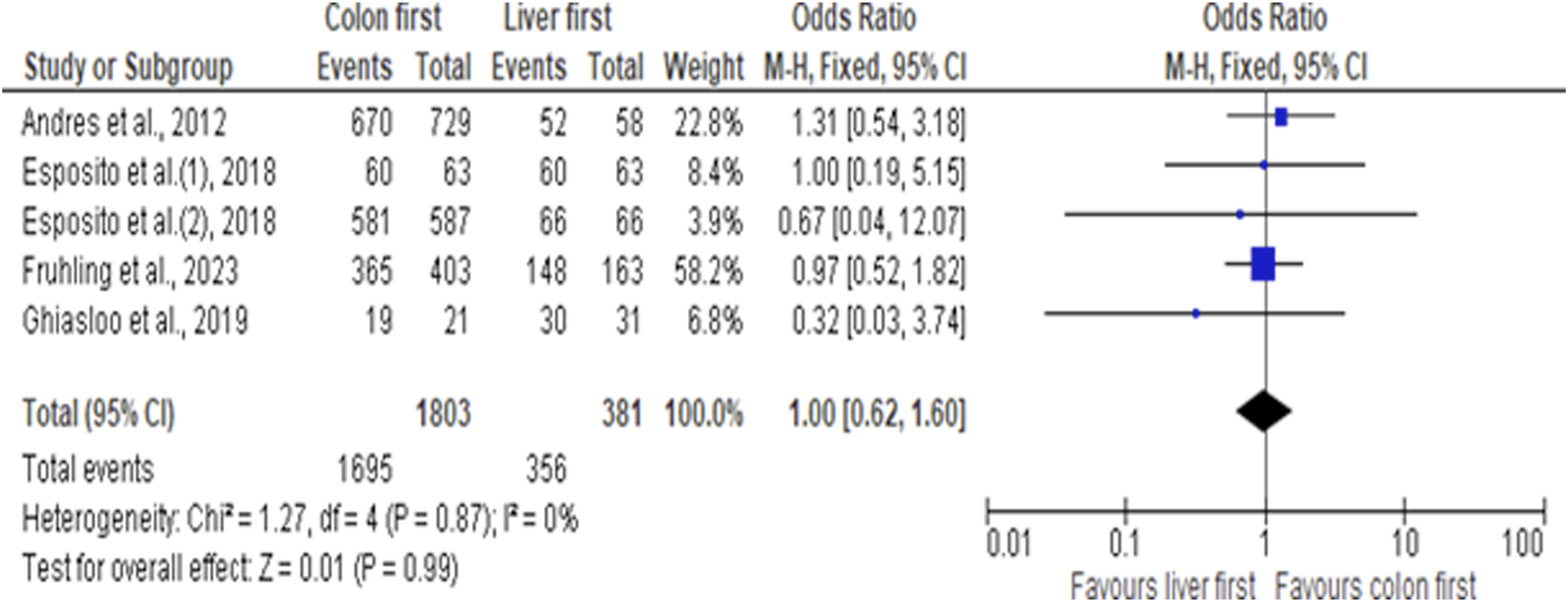
Major hepatectomy was less common in simultaneous strategy, rates not exceeding 40%, while several colon-first studies reported rates reaching 70% in their study cohorts. Forrest plot comparing rates of major hepatectomy in these two approaches. Supplemental Figure 1 shows a higher rate in colon first 60.2% vs 24.1% (OR 4.61, 95% CI 2.79, 7.64) difference is statistically significant P = 0.00001.
Meanwhile major hepatectomy was more common in liver-first approach as compared to colon-first 46% vs 41.6% (OR 0.86, 95%CI 0.7, 1.05), though this difference was not statistically significant P = 0.13 (Supplemental Figure 2).
Operative time seemed slightly but not significantly longer in staged procedures compared to simultaneous resections 766 vs 539 min (MD 24.35, 95% CI −50.51, 99.21) P = 0.52. Operative time in colon-first strategy was calculated as the sum of both procedures (Supplemental Figure 3).
Amount of blood loss showed marked heterogenicity among studies comparing the same approach; however, mean blood loss was higher in colon-first approach compared to simultaneous 950 vs 707 mL (MD 41.35, 95% CI −104.24, 186.94) P = 0.58 (Supplemental Figure 4).
Transfusion rates were equal on comparing simultaneous to colon-first approach (Supplemental Figure 5).
Combined length of hospital stay following both procedures of a staged approach, calculated by summation of duration of hospital admission after each stage of the treatment protocol, was on average longer, exceeding a total of 15 days in most cases, while most studies on simultaneous approach reported hospital stay below 10 days, this difference was found to be statistically significant (MD 4.49, 95% CI 2.13, 6.85) P = 0.0002 (Supplemental Figure 6).
Perioperative morbidity rates are comparable between different groups. Simultaneous resection has a slightly though not statistically significant-higher complication rate than colon-first resection 30.5% vs 24.1% (OR 0.76, 95% CI 0.58, 1.01) P = 0.06 (Supplemental Figure 7), while liver-first approach had a significantly higher morbidity compared to colon first 45% vs 32.5% (OR 0.58, 95% CI 0.38, 0.88) P = 0.01 (Supplemental Figure 8).
On comparing postoperative mortality, simultaneous approach has a significantly higher mortality rate compared to colon-first approach 5% vs 1% (OR 0.22, 95%CI 0.08, 0.56) P = 0.002 (Supplemental Figure 9), with highest percent reaching up to 10% in one simultaneous study cohort versus 5% as the highest value attained in colon-first group. Difference in postoperative mortality was not significant between liver-first and colon-first cohorts (Supplemental Figure 10).
Discussion
This systematic review includes 26 studies conducted over the past two decades, including a total of 10 644 patients, of whom 6699 underwent colon-first resection (63%), 971 liver-first resection (9%), and 2974 simultaneous resection (28%). Although advances in systemic therapy and surgical techniques have expanded the available treatment options, pooled analyses demonstrate no significant differences in 1-, 3-, or 5-year overall survival among the three sequencing strategies. These findings suggest that survival alone may not be the principal determinant of strategy selection and support a more individualized, decision-oriented approach when determining operative sequencing.
In 2015, Sabbagh et al 37 retrospectively reviewed 52 patients with metastatic rectal cancer who underwent curative-intent surgery using colon-first, liver-first, or simultaneous approaches and found no significant difference in long-term survival among the three groups (P = 0.5). Beyond reinforcing the absence of survival superiority, these findings suggest that operative sequencing in this setting may be guided more appropriately by disease characteristics, technical considerations, and patient-specific factors rather than expectations of differential long-term survival.
Frühling et al 12 conducted a larger and more recent analysis including 658 patients with both colon and rectal primaries who underwent colon-first, liver-first, or simultaneous resection. Five-year overall survival following simultaneous resection (48.9%) was not inferior to staged approaches (44.2% for colon-first and 43.6% for liver-first; P = 0.455), findings that are consistent with our results. These comparable outcomes further support the concept that operative sequencing should not be selected on the expectation of superior long-term survival, but rather tailored according to tumor burden, primary tumor characteristics, operative complexity, and overall patient condition.
Similarly, a meta-analysis conducted by Kelly et al 7 comparing colon-first, liver-first, and simultaneous resections demonstrated no significant long-term survival advantage for any single strategy (P = 0.93 for combined vs colorectal-first; P = 0.37 for liver-first vs colorectal-first; P = 0.41 for liver-first vs combined), further reinforcing the absence of clear oncologic superiority among approaches.
In contrast, Boudjema et al 35 published in 2021 the first prospective randomized controlled trial comparing simultaneous and colon-first resection. At two years after randomization, overall survival was higher in the simultaneous group (87.2%) compared with the colon-first group (69.6%) (P = 0.05), differing from our findings. However, the authors acknowledged that the study lacked sufficient statistical power to recommend simultaneous resection universally and did not specifically evaluate outcomes in the context of major hepatectomies or complex colorectal procedures. This limitation underscores that operative sequencing decisions must consider procedural complexity and patient selection rather than relying solely on short-term survival differences.
Conversely, a large population-based study from Ontario, Canada, including 2738 patients, conducted by Wang et al 27 reported a higher 90-day postoperative complication rate and lower 5-year overall survival (37%) in patients undergoing simultaneous resection compared with those treated with a colon-first approach (55%) (P < 0.001). The authors attributed these differences, relative to prior retrospective reports demonstrating survival equivalence, to the population-based design of their study, which may more accurately reflect real-world practice beyond high-volume tertiary centers. These findings highlight the importance of institutional expertise and case selection in determining sequencing strategy, suggesting that outcomes associated with simultaneous resection may be highly context-dependent rather than universally generalizable.
One of the more surprising and novel observations in this meta-analysis is that simultaneous resection was associated with significantly higher 30-day postoperative mortality compared with the colon-first approach (P = 0.002), despite patients in the simultaneous group having fewer and smaller liver lesions and undergoing fewer major hepatectomies (P < 0.00001). At first glance, this finding is counterintuitive: if simultaneous patients have lower hepatic tumor burden and less extensive liver surgery, why would their perioperative mortality be higher?
While our pooled data cannot definitively explain this finding, several hypotheses merit consideration based on our review of the included studies. First, simultaneous resection combines two major abdominal procedures in a single operative setting, which may prolong physiologic insult and increase systemic inflammatory response, even if each individual component is less extensive. Second, patients selected for simultaneous resection may have unmeasured comorbidities—such as poor nutritional status, occult cardiopulmonary disease, or higher ASA class—that are not captured in the pooled data set but predispose to postoperative death. Third, the higher mortality may reflect institutional or operator factors: simultaneous resections are technically demanding and may have worse outcomes in lower-volume centers or when performed by less experienced teams. The population-based study by Wang et al 27 supports this interpretation, as real-world outcomes differed substantially from high-volume center reports. Fourth, the definition of “postoperative mortality” varied across studies (30-day vs in-hospital), and some studies may have included deaths from anastomotic leakage or septic complications that are more common after combined colorectal and liver surgery. Finally, it is possible that selection bias worked in the opposite direction: surgeons may have offered simultaneous resection to patients who appeared fit but actually harbored occult frailty, whereas higher-risk patients were intentionally staged, creating a paradoxical finding.
We encourage future studies to report cause-specific postoperative mortality and to stratify by major vs minor hepatectomy, extent of colorectal resection (eg, low anterior resection vs right colectomy), and center volume. In the meantime, we caution that simultaneous resection—even for limited hepatic disease—should not be viewed as a low-risk procedure. Careful preoperative risk assessment, including cardiopulmonary evaluation and nutritional optimization, is essential.
In more than one study, hepatic tumor burden has been reported to be lower in patients selected for simultaneous resection compared with staged approaches. In the analysis by Frühling et al, 12 the majority of patients undergoing simultaneous resection had only one to two liver lesions, whereas those treated with a liver-first strategy more frequently presented with five or more metastases (P = 0.018). Consequently, the simultaneous cohort underwent fewer and less extensive major hepatectomies than patients managed with staged resections. These differences likely reflect deliberate patient selection, whereby individuals with limited hepatic disease and lower operative complexity are preferentially considered for single-stage surgery, reinforcing the need to interpret comparative outcomes within the context of baseline tumor burden and procedural risk.
Similarly, our analysis demonstrated that patients undergoing simultaneous resection had a lower hepatic tumor burden and a significantly lower rate of major hepatectomy compared with those treated with a colon-first approach (P < 0.00001). In contrast, patients selected for a liver-first strategy were more likely to present with a greater number and larger size of hepatic lesions, as also reported in the meta-analysis by Kelly et al. 7 These findings are consistent with the conceptual rationale proposed by Mentha et al 38 in which the liver-first approach prioritizes early control of extensive hepatic disease to reduce the risk of progression and potential loss of resectability. Together, these observations reinforce that sequencing strategies are frequently determined by baseline metastatic burden and technical considerations, rather than by expectations of inherent survival superiority.
Regarding operative time, our analysis showed that simultaneous resection was associated with a shorter operative duration compared with staged approaches; however, this difference did not reach statistical significance (P = 0.52). This finding is consistent with Alexandrescu et al 16 who reported significantly shorter operative times with the simultaneous approach (P < 0.0001), and with the meta-analysis by Yin et al 39 which also demonstrated a modest but significant reduction in operative time for simultaneous procedures compared with staged resections (P = 0.05). In contrast, Frühling et al 12 observed the longest operative times in the simultaneous group (320 minutes), followed by liver-first (217 minutes) and colon-first strategies (195 minutes) (P < 0.001). These discrepancies likely reflect differences in case selection, extent of hepatectomy, and institutional practice patterns, further underscoring that operative metrics are closely linked to procedural complexity and patient characteristics rather than the sequencing strategy alone.
Regarding intraoperative blood loss, Yin et al 39 reported significantly lower blood loss in patients undergoing simultaneous resection (P = 0.04). Our analysis observed a similar trend, although the difference did not reach statistical significance (P = 0.58). These findings are supported by Valdimarsson et al 36 who documented lower intraoperative blood loss in the simultaneous group compared with colon-first resections (600 vs 700 mL; P = 0.003). In contrast, Alexandrescu et al 16 reported higher blood loss in simultaneous procedures compared with staged resections (300 vs 225 mL), though this difference was not statistically significant (P = 0.3498). Taken together, these data suggest that intraoperative blood loss is influenced not only by the sequencing strategy but also by patient selection, tumor burden, and the extent of hepatectomy, emphasizing the importance of individualized surgical planning.
There was general agreement across studies regarding length of hospital stay, which in our analysis was significantly shorter for patients undergoing simultaneous resection compared with colon-first resections. This finding aligns with reports by Alexandrescu et al 16 (P < 0.0001), the randomized trial by Boudjema et al 35 the meta-analysis by Gumiero et al 9 and Yin et al. 39
Postoperative complication rates, however, were more variable. In our study, complications were higher in the simultaneous group compared with colon-first resections, though this difference did not reach statistical significance (P = 0.06). Liver-first resections, in contrast, were associated with a significantly higher complication rate than colon-first approaches (P = 0.01), consistent with Esposito et al 15 who reported postoperative morbidity of 45% for liver-first versus 32.9% for colon-first (P = 0.04), and with Bogach et al 28 who also found higher morbidity following simultaneous resections. Boudjema et al 35 observed a slightly higher complication rate in the simultaneous group (49%) compared with colon-first (46%), though this difference was not statistically significant (P = 0.08). Frühling et al 12 reported that major complications were lowest in the liver-first group (9.8%), followed by colon-first (10.2%), and highest in the simultaneous group (15.4%) (P = 0.334). These results highlight that postoperative risk is influenced by both patient selection and sequencing strategy, underscoring the need for individualized operative planning.
Perioperative mortality in our analysis did not differ significantly between colon-first and liver-first approaches (P = 0.99), consistent with findings reported by Esposito et al. 15 In contrast, 30-day postoperative mortality was significantly higher in patients undergoing simultaneous resection compared with the colon-first group (P = 0.002), in agreement with the meta-analysis by Gumiero et al. 9 These observations indicate that while survival outcomes are broadly comparable, simultaneous resections may carry increased short-term risk, reinforcing the need for careful patient selection and consideration of physiologic reserve when planning single-stage surgery.
Sutton et al 40 similarly reported no significant differences in overall survival among colon-first, liver-first, and simultaneous resections, but noted a higher rate of major postoperative complications following simultaneous procedures. They also highlighted potential concerns with the liver-first approach, particularly the risk of tumor progression or seeding from an untreated primary tumor, especially in patients with rectal primaries. This risk may be mitigated in the context of total neoadjuvant therapy, as the primary tumor remains in situ while hepatic disease is addressed surgically. Sutton et al 40 further observed a higher proportion of rectal primaries in the liver-first group. Given that total neoadjuvant therapy is now well established for rectal cancer, intervening on liver metastases during this treatment window may help prevent disease progression, particularly since hepatic tumor burden remains the principal determinant of survival in patients with synchronous colorectal liver metastases.
Lakha et al 41 reported no significant differences in 3- and 5-year overall survival among colon-first, liver-first, and simultaneous resections, but found higher postoperative morbidity in the simultaneous group. These results support the principle that simultaneous resections should be reserved for carefully selected patients with sufficient physiological reserve to tolerate increased surgical stress. Notably, their analysis included only prospective propensity score-matched studies to reduce selection bias, which aligns with our observation that liver-first strategies are often chosen for patients with higher hepatic tumor burden, whereas those undergoing simultaneous resections generally present with more favorable disease characteristics.
One theoretical advantage of simultaneous resection is the ability to remove both the primary tumor and hepatic metastases in a single operative session, potentially reducing the risk of disease progression beyond resectability. However, most studies show that patients selected for simultaneous procedures generally have a lower hepatic tumor burden compared with those undergoing staged approaches. While this selection bias is clinically justifiable, it may artificially confer a perceived survival advantage to the simultaneous group, thereby limiting the interpretability of comparative outcomes. 42
Although no significant differences in overall survival were observed between staged and simultaneous strategies, simultaneous resections were associated with higher postoperative mortality despite lower rates of major hepatectomy. This highlights the need for future studies to stratify outcomes according to the extent of hepatic resection—major vs minor—within simultaneous approaches to better define their respective risk profiles. 43
Overall, while simultaneous resection provides the advantage of comprehensive oncologic clearance in a single procedure and reduces the risk of missing the surgical window, it carries an increased risk of postoperative morbidity and mortality, even among patients undergoing less extensive liver resections. Until further evidence becomes available, simultaneous resection should be considered non-inferior to staged approaches only in carefully selected patients with limited hepatic disease and adequate physiological reserve.42,43
Given the considerable heterogeneity among patients with synchronous colorectal liver metastases, determining an optimal surgical strategy remains challenging. However, to make this meta-analysis useful for the practicing surgeon, we offer the following specific, scenario-based recommendations derived from our findings and the reviewed literature.
For patients with limited hepatic disease (one to three small metastases, less than 30% liver involvement) and good performance status without significant comorbidities, simultaneous resection may be appropriate, particularly if the colorectal resection is not an ultralow anterior resection or abdominoperineal resection. Evidence from Frühling et al 12 and others supports this approach in carefully selected patients. However, the patient must be counseled that postoperative mortality is higher with the simultaneous approach (approximately 2-4% vs 1% for colon-first in our pooled analysis), even though long-term survival is equivalent.
For patients with extensive hepatic involvement—particularly those with five or more metastases or requiring major hepatectomy—a liver-first strategy should be strongly preferred, regardless of primary tumor symptoms. This approach prioritizes control of the dominant prognostic site (the liver) and reduces the risk of hepatic progression during a colon-first delay. This recommendation is supported by Kelly et al, 7 Mentha et al, 38 and our observation that liver-first patients had significantly higher hepatic tumor burden yet achieved comparable long-term survival.
For patients with locally advanced rectal cancer requiring neoadjuvant therapy, a liver-first strategy following systemic treatment (or during total neoadjuvant therapy) may be appropriate, as hepatic disease remains the principal determinant of prognosis. 44 The primary tumor remains in situ and is treated with chemoradiation while liver metastases are addressed surgically, avoiding the morbidity of a combined low pelvic dissection plus hepatectomy. This approach should be reserved for high-volume centers with multidisciplinary expertise.
For elderly or frail patients, those with increased bleeding risk or anemia, or those with advanced age, staged colon-first approaches may be preferred. Reports of greater intraoperative blood loss associated with simultaneous resections 16 and our finding of a trend toward higher complication rates (P = 0.06) support this cautious approach. Staging the operations allows for physiologic recovery between procedures. Likewise, liver-first strategies may be prioritized for patients with marginally resectable liver metastases to reduce the risk of disease progression while the primary tumor is being treated. 45
In situations involving impending bowel obstruction or severe, uncontrolled bleeding from the primary tumor, an initial colon-first approach—often limited to palliative diversion followed by systemic therapy—may be necessary.46,47
Finally, institutional resources and capabilities matter significantly. Simultaneous resection and liver-first strategies should be performed only in centers with high-volume hepatobiliary and colorectal surgical expertise, as well as interventional radiology and intensive care support. The population-based study by Wang et al 27 showed worse survival for simultaneous resection outside tertiary centers, whereas randomized and high-volume series show equivalence or benefit. We therefore recommend that surgeons refer patients with complex synchronous disease (especially those needing major hepatectomy or low pelvic anastomosis) to specialized centers.
More randomized controlled trials are needed to establish a clear consensus regarding the optimal treatment sequence. In the meantime, it is evident that surgical sequencing decisions must be individualized, taking into account critical factors such as the location and extent of the primary tumor and liver metastases, patient performance status, symptom burden, and underlying comorbidities.
Limitations
A major limitation of this meta-analysis is the limited number of randomized controlled trials, with only one included study, while the remainder of the literature consisted primarily of observational studies. This restricts the strength of causal inferences that can be drawn from the pooled analysis. Additionally, substantial heterogeneity existed among the included studies regarding therapeutic strategies, including variations in chemotherapy regimens, timing of systemic therapy, and the use of open versus minimally invasive surgical techniques. These differences may have introduced confounding factors and contributed to between-study variability. Well-designed randomized controlled trials are therefore warranted to provide more robust and definitive evidence to guide surgical sequencing decisions. Regarding adherence to PRISMA 2020 guidelines, we acknowledge several important deficiencies. First, no formal risk of bias assessment was performed. The included studies were almost entirely observational, and validated tools such as ROBINS-I for non-randomized studies or the Cochrane Risk of Bias 2 tool for randomized controlled trials were not applied. This limits our ability to determine the internal validity of the individual studies and may introduce bias into the pooled estimates. Second, we did not assess publication bias using funnel plots or Egger’s regression test. Because most comparisons in this meta-analysis included fewer than 10 studies, statistical tests for publication bias would have been unreliable. Third, we did not apply GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) methodology to assess the certainty of evidence for each outcome. Fourth, this meta-analysis was not prospectively registered on PROSPERO or any other registry, which introduces the risk of reporting bias and is a deviation from PRISMA 2020 recommendations.
A summary of PRISMA 2020 compliance, including items followed and items not followed, is provided as a Supplemental Figure 11.
Conclusion
This meta-analysis demonstrates that no single surgical sequencing strategy—colon-first, liver-first, or simultaneous resection—provides a definitive overall survival advantage for patients with synchronous colorectal liver metastases. However, a novel and counterintuitive finding is that simultaneous resection is associated with significantly higher postoperative mortality despite lower hepatic tumor burden and fewer major hepatectomies. This observation warrants further investigation and clinical caution. Rather than endorsing a uniform approach, the findings highlight the importance of individualized treatment selection based on patient- and disease-specific factors. Considerations such as hepatic tumor burden, primary tumor location (colon vs rectum), anticipated extent of liver resection, response to neoadjuvant therapy, and institutional expertise should inform clinical decision-making within a multidisciplinary framework. For the practicing surgeon, we offer specific scenario-based recommendations: simultaneous resection for fit patients with limited disease; liver-first for extensive hepatic burden or rectal cancer requiring neoadjuvant therapy; and colon-first for elderly, frail, or symptomatic patients.
In this context, surgical sequencing should be regarded as a tailored strategy rather than a fixed algorithm. Although survival outcomes appear comparable across approaches, variations in perioperative risk profiles and patient selection indicate that optimal management depends on aligning the surgical strategy with the biological and technical characteristics of each case. This study provides a contemporary evidence-based framework to support individualized decision-making and underscores the need for future randomized and subgroup-focused trials to refine strategy selection and optimize patient outcomes.
Supplemental Material
Supplemental material - Different Surgical Strategies in Colorectal Cancer Patients With Synchronous Liver Metastasis: A Meta-Analysis
Supplemental material for Different Surgical Strategies in Colorectal Cancer Patients With Synchronous Liver Metastasis: A Meta-Analysis by Haitham M. Azmy, Ali A. Shafik, Ahmed Hussein Ahmed, Catherine Emad Saweeres and Osama El Refaie in The American Surgeon™
Footnotes
Ethical Considerations
The study was approved by the Research Ethics Committee of Cairo University (Number MS-337-2023).
Author contributions
All Authors have contributed to the conception or design of the work; interpretation of data for the work; Drafting the work or revising it critically for important intellectual content; final approval of the version to be published and Agreement to be accountable for all aspects of the work.
Funding
Funding and acknowledgment goes directly to the Faculty of Medicine of Cairo University, Egypt who completely funded and supported this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.