
Abstract
Objective
This study developed an artificial intelligence (AI)-based hand hygiene assessment system to improve low-supervision monitoring, enhance compliance in operating rooms, standardize procedures, and reduce the risk of intraoperative infections.
Methods
This system installed high-definition cameras, faucets, and hand sanitizer sensors in the operating room handwashing area to collect real-time data on handwashing videos, water flow sounds, duration of water usage, and hand sanitizer consumption. The system automatically identified health care personnel and monitors compliance with surgical handwashing protocols step-by-step, assessing whether procedures were standardized and duration requirements were met. Upon detecting omissions, sequence errors, or insufficient duration, immediate corrections were provided through visual and auditory prompts on the screen. The system automatically recorded all data throughout the process without requiring on-site supervision, ensuring stable adaptation to both routine operating room scenarios and emergency surgical procedures.
Results
Experimental findings demonstrated that the system achieved a handwashing step recognition rate of 94.57%, an assessment accuracy rate of 93.25%, and a handwashing duration compliance rate of 92.68%. When deployed in clinical environments, including surgical and emergency departments, the system significantly improved handwashing compliance, increasing the adherence rate to 94.2%. Additionally, the average handwashing duration was reduced to 45.7 seconds, accompanied by a substantial decrease in non-compliant behaviors.
Conclusion
The AI-based hand hygiene assessment system substantially enhanced the standardization and efficiency of handwashing procedures in operating rooms, significantly improved hand hygiene compliance and standardized practice, and demonstrated strong clinical applicability. Future research should focus on optimizing the model and incorporating feedback mechanisms to further improve the accuracy and user experience of the system.
Keywords
Introduction
Hand hygiene in the operating room is a cornerstone of perioperative patient safety, with a direct impact on surgical site infections (SSIs), health care-associated infections (HAIs), and postoperative outcomes. 1 Surgical site infections remain among the most frequent and costly complications of surgery, accounting for up to 31% of all HAIs and contributing to prolonged hospitalization, increased health care costs, and higher mortality. 2 To mitigate these risks, international guidelines mandate standardized surgical handwashing protocols, specifying key steps, minimum duration (≥40 seconds per WHO recommendations), and appropriate antiseptic use, as outlined by the WHO, CDC, and health care quality initiatives such as The Joint Commission’s National Patient Safety Goals.2,3 Compliance is therefore both a regulatory requirement and an essential component of efficient surgical workflow, as deviations may delay procedures or compromise sterility.
Despite strong evidence supporting hand hygiene, real-world adherence in operating rooms remains suboptimal. Conventional supervision relies on manual observation by infection control staff or peers, which is subjective, labor-intensive, and susceptible to bias and error. 1 These limitations are amplified in high-pressure surgical environments characterized by time constraints, emergency cases, and complex scheduling. Consequently, incomplete handwashing steps, shortened duration, and improper antiseptic use continue to occur, increasing the risk of pathogen transmission and SSIs.4,5 Moreover, manual monitoring lacks real-time feedback, reducing opportunities for immediate correction and limiting data-driven quality improvement and regulatory reporting.
Health care institutions are required to document hand hygiene adherence as part of accreditation processes and public health surveillance; however, manual data collection is frequently incomplete or inaccurate, resulting in compliance gaps and potential regulatory penalties. 6 Within surgical teams, inconsistent hand hygiene practices can also disrupt workflow continuity. Delays caused by rework, such as repeated handwashing following observed non-compliance, or disagreements regarding protocol adherence may impair team communication and efficiency, particularly during time-critical situations such as trauma or emergency surgeries. 7 These clinical, regulatory, and operational challenges have driven growing interest in automated and intelligent hand hygiene assessment systems in perioperative care.3,8
Recent advances in artificial intelligence (AI), especially deep learning, provide a strong technical foundation for such systems. Convolutional neural networks (CNNs) have shown excellent performance in image and video analysis by effectively extracting spatial features and recognizing complex hand movements.4,7 This makes CNN-based models well suited for monitoring surgical hand hygiene practices and overcoming the subjectivity and inefficiency of manual supervision. In parallel, multimodal data fusion technologies enable the integration of heterogeneous data sources, including video streams, audio cues, and sensor-based inputs such as hand sanitizer dispenser usage or water flow data. By combining visual recognition with objective behavioral measurements, these approaches improve the accuracy and completeness of hand hygiene assessments and better align with the quantitative requirements of infection prevention programs. 9
Despite these technological advances, current hand hygiene monitoring systems remain limited in their ability to adapt to the complex operating room environment. Many systems can only perform coarse classifications (eg, “washing” vs “not washing”) and cannot reliably identify specific steps of the surgical handwashing protocol or verify compliance with duration and antiseptic use standards. 10 Environmental challenges, including variable lighting, occluded camera views, and rapid hand movements, further reduce system stability and accuracy.9,11,12
In this context, the present study develops an AI-driven, multimodal intelligent system to accurately assess standardized hand hygiene practices among operating room personnel. By enabling precise step recognition, duration verification, and timely feedback, the system aims to bridge gaps between infection control standards, clinical workflow demands, and regulatory compliance, ultimately supporting SSI prevention and data-driven quality improvement.
Methods
Study Design and Clinical Setting
This study was conducted in a multi-center clinical environment encompassing the operating rooms and emergency departments of three tertiary hospitals. The primary research sites included standard surgical operating rooms (for elective surgeries), emergency operating rooms (for trauma and urgent procedures), and a simulated surgical training laboratory (for supplementary data collection and model pre-calibration). The clinical setting was selected to reflect real-world conditions, including variable lighting, personnel movement dynamics, and workflow pressures, ensuring the system’s adaptability to high-demand medical environments.
Data Set Characteristics
Data Collection
The data set comprised clinical and simulated hand hygiene practice data. A total of 386 high-definition videos (1920 × 1080 pixels, 30 fps) of surgical and emergency handwashing procedures were collected from 52 health care professionals, including surgeons, nurses, anesthesiologists, and surgical assistants with 2-15 years of experience, reflecting diverse skill levels and practice patterns. Each video was annotated according to the WHO Surgical Hand Hygiene Guidelines, covering 10 standardized handwashing steps (eg, palm rubbing, finger interlacing, thumb cleaning, and wrist washing). Annotations were performed by two certified infection control nurses and one senior surgical educator, achieving an inter-annotator agreement exceeding 95%. In addition, synchronized audio data (eg, water flow and sanitizer dispensing) and sensor data (water flow duration and sanitizer volume) were collected to support multimodal data fusion and enhance assessment accuracy.
Data Partitioning
The data set was stratified and randomly divided to ensure balanced clinical characteristics across the training, validation, and test sets. Stratification was performed according to study site, professional role, years of experience, and clinical environment to maintain comparable demographic, professional, and environmental characteristics among subsets. Participants were mutually exclusive across subsets to ensure independent evaluation. A strict participant-level separation was implemented: individuals in the test set were completely unseen during model training and validation. The training set included 270 videos (70%), representing 36 participants and 2700 annotated handwashing step sequences, and was used for model training. The validation set comprised 77 videos (20%) from 10 participants (770 sequences) for hyperparameter tuning and interim performance assessment, while the test set contained 39 videos (10%) from 6 previously unseen participants (390 sequences) to evaluate generalizability. Validation data were mainly collected in real operating room settings, supplemented by standardized simulated environments to ensure clinical relevance and robust model evaluation.
AI-Based Hand Hygiene Assessment System
The core of the system was an enhanced CNN integrated with multimodal data fusion technology, designed to recognize handwashing steps, monitor compliance, and provide real-time feedback. Key components included video/audio data acquisition, feature extraction, step recognition, and compliance assessment. Detailed technical implementations and corresponding algorithms (eg, network architecture parameters and mathematical formulas for convolution operations) are provided in the Supplementary Materials and Supplemental Figure 1.
Multimodal Data Fusion
The system integrated three data modalities: (1) Video data: Captured by wide-angle HD cameras installed in handwashing areas, used to recognize hand movements and step execution. (2) Audio data: Synchronized with video to capture environmental sounds (eg, continuous water flow indicating active handwashing), processed via recurrent neural networks to supplement motion recognition. (3) Sensor data: Collected from pressure sensors in faucets and hand sanitizer dispensers to record water flow duration and sanitizer usage, ensuring objective verification of protocol adherence.
All three participating hospitals adopted the same WHO-standard surgical hand hygiene protocol and used the same brand and formulation of alcohol-based surgical hand rub to eliminate variability in antiseptic type, dispensing volume, and application steps across centers. Uniform sensor calibration and threshold settings were applied at all sites to ensure consistent data collection and standardized model training and validation across institutions.
System Operating Process
(1) Identity verification: Health care personnel were identified via facial recognition or staff ID cards, and role-specific handwashing protocols (eg, surgeon vs nurse) were loaded. (2) Real-time monitoring: Cameras and sensors continuously collected data, with the AI model analyzing video frames to recognize steps and synchronize with sensor data. (3) Feedback provision: Real-time visual feedback was displayed on a 21-inch screen mounted 1.5 meters above the scrub sink, showing the current step, progress bar, and remaining required duration. Audio feedback used gentle, non-intrusive prompts (50-60 dB, similar to normal conversation volume) to alert staff of missed steps, incorrect sequence, or insufficient duration. The feedback was non-blocking and non-interruptive: staff could continue handwashing without disruption, and alerts could not be disabled during active handwashing to ensure compliance. Immediate on-screen correction guided staff to complete missing steps within the same session, while post-hoc automated reports were generated daily for infection control teams to review trends and provide targeted education. This combination of real-time guidance and post-session data effectively standardized behavior and improved long-term adherence without disrupting surgical workflow.
Outcome Measures
Recognition Accuracy
Recognition accuracy is defined as the percentage of handwashing steps correctly identified by the system relative to annotated steps. Calculation: (Number of correctly recognized steps/Total number of annotated steps) × 100%. A “correctly recognized step” required the system to identify the step type and its start/end time within ±2 seconds of the annotated timeline.
Compliance Rate
It is a composite measure of adherence to hand hygiene protocols, including: (1) Step compliance: Completion of all 10 mandatory steps without omissions or out-of-sequence execution. (2) Duration compliance: Total handwashing duration ≥40 seconds (per WHO guidelines). (3) Sanitizer compliance: Proper use of antiseptic hand sanitizer (verified via sensor data). Overall compliance rate = (Number of handwashing events meeting all three criteria/Total number of handwashing events) × 100%.
Handwashing Duration
It is defined as the total time from the start of water flow (or sanitizer application) to the end of the final handwashing step, recorded automatically by the system via sensor and video data synchronization.
Comparative Model Selection
To assess the performance of the enhanced CNN model, four comparative algorithms were selected based on prior use in hand hygiene and motion recognition research. A traditional CNN served as the baseline to evaluate the added value of architectural enhancements. Support Vector Machine-Back Propagation and Random Forest-Back Propagation models were included for their established application and robustness in health care motion classification under variable clinical conditions. K-Nearest Neighbor was used as a simple, interpretable reference to highlight the advantages of deep learning for high-dimensional video data. All models were trained and evaluated on the same data set using identical metrics to ensure comparability, with technical details provided in the Supplementary Materials.
Ethics Approval, Consent, and De-identification of Video and Sensitive Data
This study was conducted with approval from the Ethics Committee of the hospital (Approval Number: XJS20242281-C-1, Approval Date: October 6th, 2024). The study was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. Participants were informed that video and audio data would be collected for hand hygiene monitoring purposes, and that their identity would be protected through the measures described below.
To protect health care personnel privacy, the AI hand hygiene assessment system applied a multi-layer de-identification strategy. All videos underwent automated AI-based facial blurring before storage or training, obscuring faces, name tags, and other identifying features; analyses retained only hand and arm regions, with backgrounds cropped or blurred. Video and audio files were stripped of metadata and assigned random identifiers, with any linkage to personal information stored separately in an encrypted, access-restricted database. Data collection was limited to hand hygiene-related movements and sounds, excluding conversations and clinical procedures. De-identified data were retained for up to 12 months for quality assurance. The system complies with HIPAA and GDPR, balancing effective monitoring with robust privacy protection.
Experimental Design and Analysis
Experimental Data Preparation
The primary data sources consist of HD videos capturing handwashing operations in operating rooms, complemented by audio data. This combination enables the multimodal fusion model to comprehensively assess the standardization and completeness of handwashing practices. The hardware and software configurations used in the experiments are detailed in Supplemental Table 1.
Experimental Results and Analysis
A total of 892 valid hand-scrubbing events were included in the final analysis (denominator for all compliance estimates). They were collected from real clinical settings and controlled simulation scenarios, ensuring diversity across professional roles, skill levels, and environments. Model performance was evaluated by comparing accuracy and recall among five algorithms: the proposed improved CNN, traditional CNN, SVM-BP, RF-BP, and KNN (Figure 1). Evaluation and comparison of the performance of various models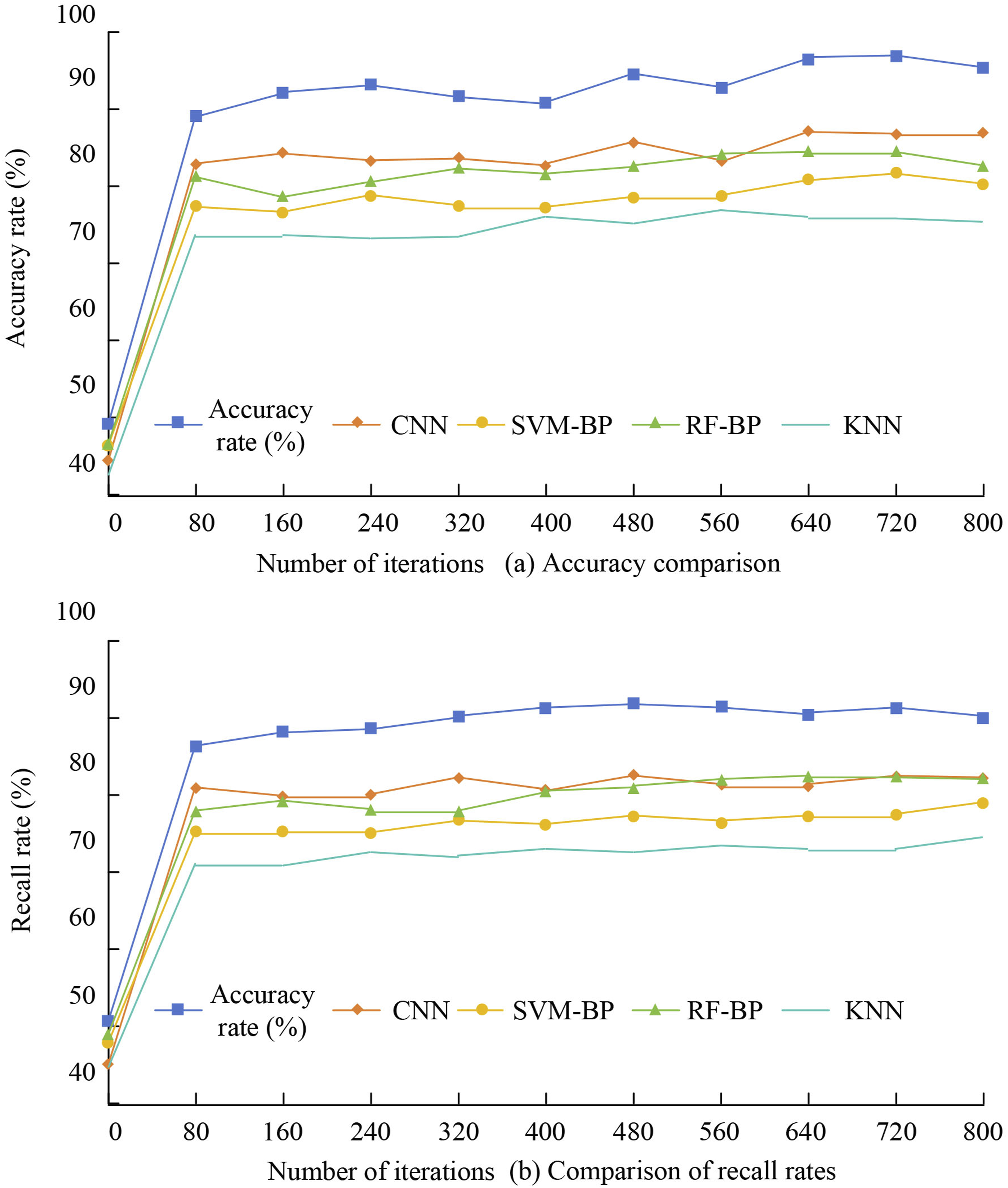
As shown in Figure 1A, the improved CNN consistently outperformed all comparison models across training iterations. Accuracy increased rapidly from 50.78% to a peak of 91.91% at 480 iterations and remained above 90% thereafter, indicating strong convergence and stability. In contrast, the traditional CNN plateaued at approximately 85%, SVM-BP peaked at 87.12%, RF-BP at 80.81%, and KNN remained below 75%. Similarly, Figure 1B demonstrates that the improved CNN achieved the highest recall throughout training, while SVM-BP and RF-BP showed slower improvements and lower final recall. These results indicate superior accuracy, recall, and robustness of the proposed model.
As shown in Supplemental Figure 2, the improved CNN exhibits superior computational efficiency, with training time decreasing from 20.87 s to 17.79 s by 80 iterations and remaining stable thereafter, indicating rapid convergence. In comparison, the traditional CNN demonstrates longer training times and slower convergence, while the SVM-BP model shows lower initial time but reduced convergence efficiency.
Figure 2 presents the confusion matrix for handwashing step recognition. The model achieves high accuracy across most steps; however, misclassifications occur between visually similar actions, particularly between “back-of-hands rubbing” and “finger interlacing rubbing.” Overall, the results demonstrate strong efficiency and robust classification performance, with limitations mainly related to subtle motion distinctions. Confusion matrix of an enhanced Convolutional Neural Network (CNN) model for handwashing step recognition in operating rooms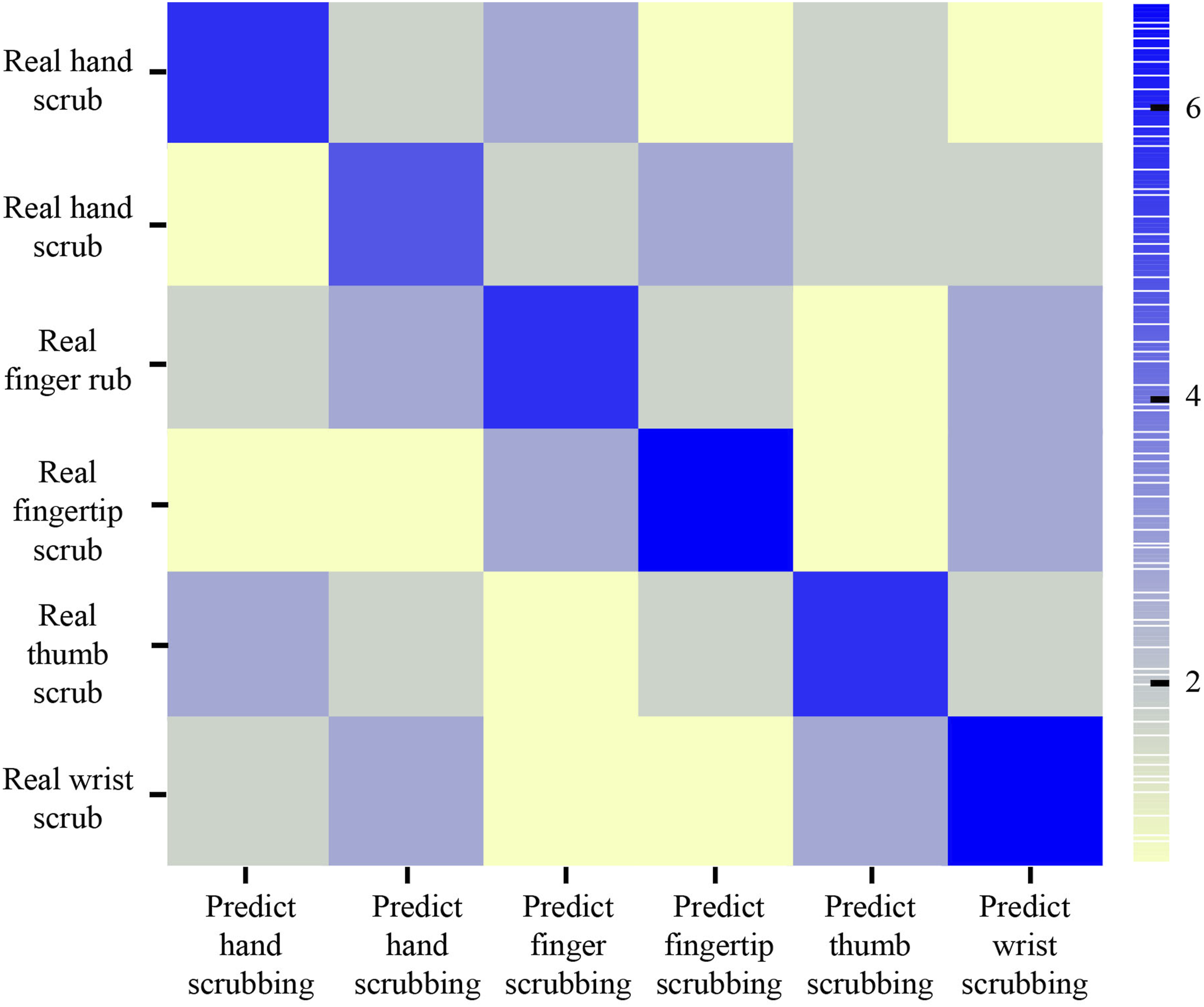
The enhanced CNN model achieved a handwashing step recognition rate of 94.57% (95% CI: 92.81%-95.93%), an assessment accuracy of 93.25% (95% CI: 91.30%-94.76%), and a handwashing duration compliance rate of 92.68% (95% CI: 90.64%-94.31%). All estimates were derived using generalized estimating equations (GEEs) with robust standard errors to account for clustering within participants and hospitals (three tertiary centers). In clinical deployment, the AI monitoring system significantly increased overall hand hygiene compliance to 94.2% (95% CI: 92.1%-95.8%) compared with 83.5% (95% CI: 80.6%-85.9%) in the control group (difference: 10.7%, 95% CI: 7.3%-14.1%, P < 0.001). Average handwashing duration was 45.7 seconds (95% CI: 44.3-47.1 s) in the intervention group vs 58.3 seconds (95% CI: 56.5-60.1 s) in the control group (mean difference: −12.6 s, 95% CI: −14.8 to −10.4 s, P < 0.001). Subgroup analyses were performed to evaluate the effects of clinical environment (elective OR vs emergency OR vs simulated lab) on system performance and compliance. Recognition accuracy remained high across all settings: 94.1% (elective OR), 93.6% (emergency OR), and 95.2% (simulated lab), with no statistically significant difference between environments (P for interaction = 0.32). Similarly, compliance rates were consistent across centers and environments (all P > 0.05), indicating the system was robust to variation in lighting, workflow pressure, and clinical setting.
Empirical Analysis
Qualitative Interview Feedback Data Table
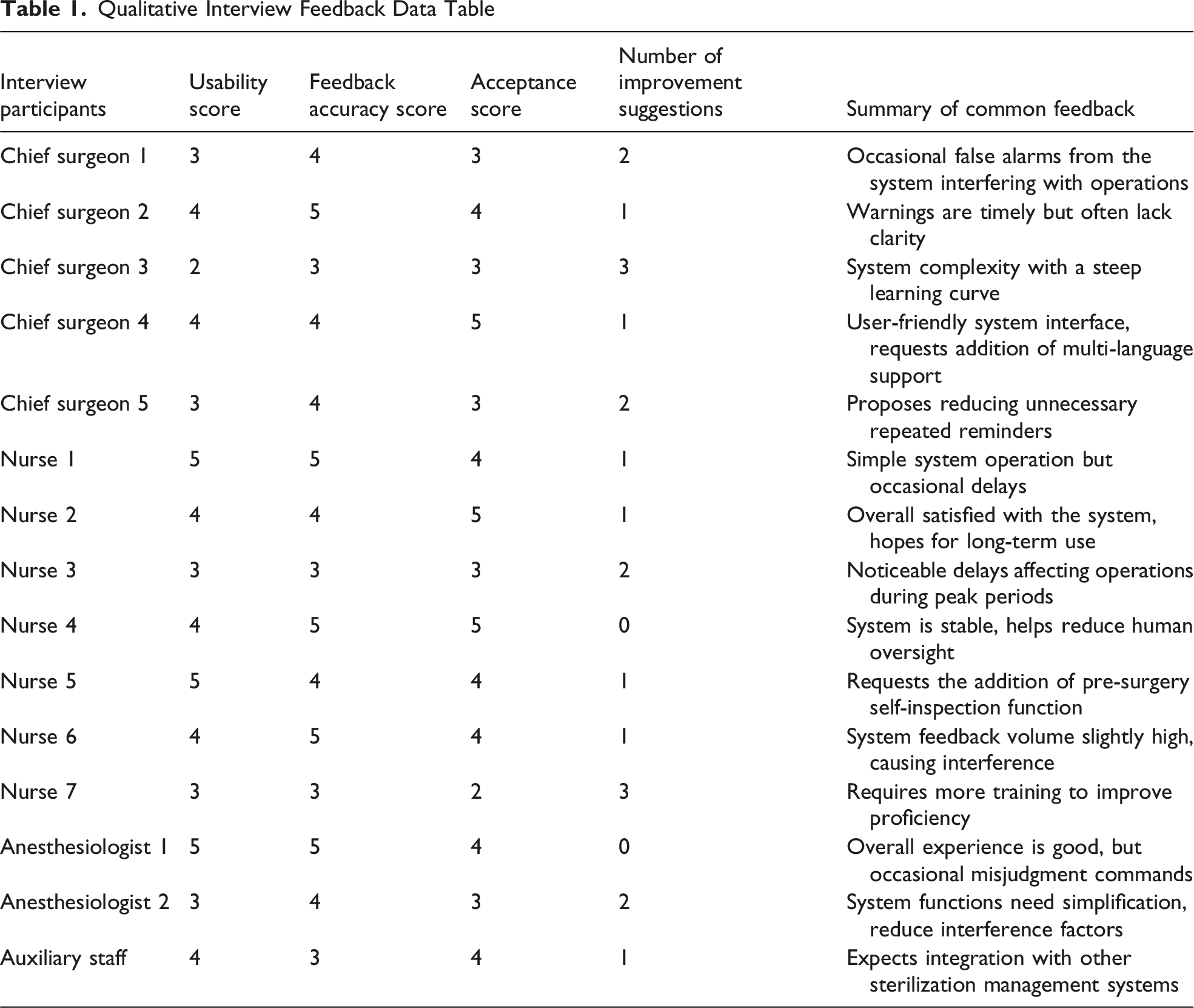
A 4-week comparative study was conducted between the AI intervention group and the conventional manual supervision group. The denominator for calculating the compliance rate was the total number of observed handwashing events (intervention group: n = 437; control group: n = 455). Compliance rate was expressed as a percentage with 95% CI and standard deviation (SD) to reflect data variability.
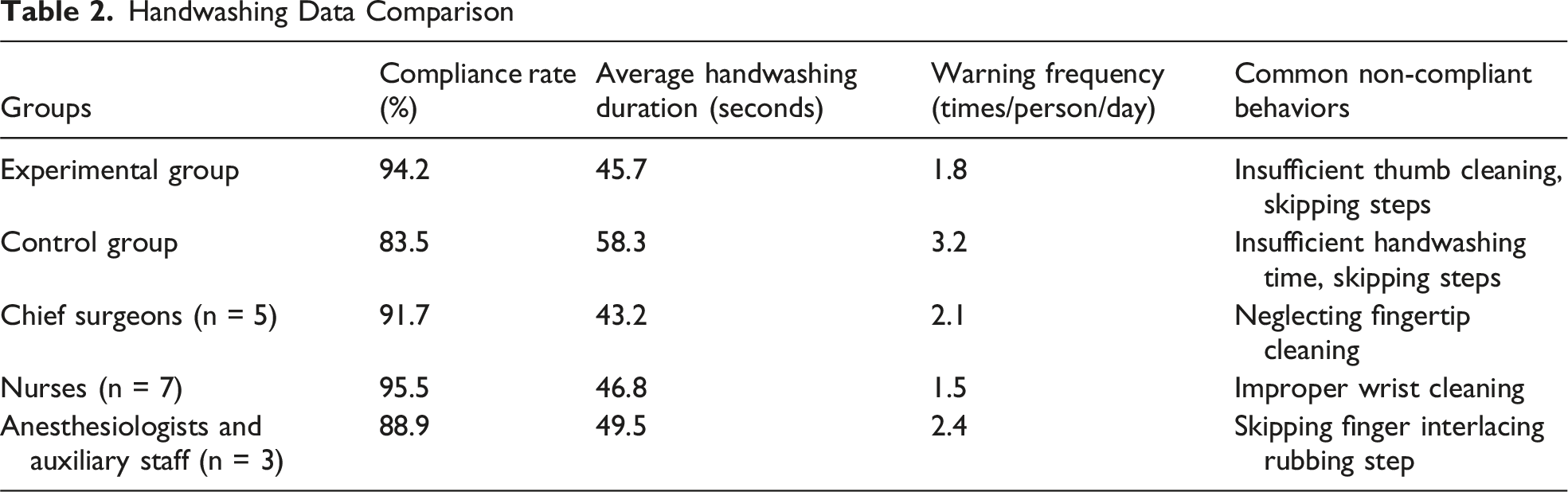
Handwashing Data Comparison
Discussion
The AI-based hand hygiene assessment system developed in this study addresses critical unmet needs in perioperative infection control and surgical team workflow optimization. Beyond its technical advantages in algorithm performance, the system’s core value lies in its direct translation to clinical practice, strengthening SSI prevention, streamlining operating room team coordination, and aligning with infection control standards. Below, we elaborate on its clinical significance for surgical teams and infection control practices, linking technical outcomes to real-world health care impacts.
Enhancing Perioperative Infection Control
Surgical site infections remain a leading cause of health care-associated infections, accounting for 31% of all HAIs, and are closely linked to inadequate hand hygiene.1,2 Traditional manual supervision is limited by subjectivity, resource constraints, and workflow pressures. The AI-based system addresses these gaps, achieving a 94.57% handwashing step recognition rate and 93.25% assessment accuracy, translating to a 10.7% absolute increase in compliance (from 83.5% to 94.2%). For a department performing 50 daily surgeries, this reduces non-compliant events by ∼ 5 per day, lowering pathogen transmission risk. Duration compliance of 92.68% meets the WHO ≥40-second standard, ensuring adequate antiseptic contact.2,3 Real-time feedback through visual and auditory alerts corrects non-compliant behaviors immediately, unlike post-hoc auditing. Automated logs and weekly reports enable infection control teams to identify recurring issues and target training, providing data-driven optimization beyond the capabilities of manual monitoring.
A key limitation and practical strength of this study need to be emphasized: The control group received routine, active manual monitoring, which is known to induce a temporary “observational effect” (Hawthorne effect) and elevate compliance above real-world unmonitored levels. In most clinical practice settings, dedicated, continuous manual supervision is not feasible due to staffing shortages, cost, and competing priorities. Thus, the true baseline compliance in routine, unsupervised clinical care is almost certainly lower than the 83.5% observed in our control group. This limitation actually strengthens the real-world value of the AI system: in settings with no manual monitoring, the AI system would likely yield an even larger improvement in compliance because it provides consistent, automated oversight without requiring human resources. Real-time feedback corrected non-compliant behaviors immediately, unlike post-hoc auditing. Automated logs and weekly reports enabled infection control teams to identify recurring issues and target training, supporting data-driven quality improvement beyond the capabilities of manual monitoring.
Optimizing Surgical Team Workflow
Operating room workflows are highly time-sensitive, and manual hand hygiene supervision can disrupt efficiency through delays and rework, affecting team coordination. 7 The AI system mitigates this tension by standardizing hand hygiene while minimizing interruptions. The experimental group maintained a consistent average handwashing duration of 45.7 seconds, within the WHO-recommended range, compared with 58.3 seconds in the control group, saving ∼12.6 seconds per event. For surgeries requiring 10 handwashing events, this reduces time by ∼ 2 minutes per case, alleviating scheduling pressures.
Aligning With Regulatory and Consistency With Global Guidelines
Health care institutions are required by international standards (eg, WHO, CDC, and The Joint Commission) to document hand hygiene compliance for accreditation and infection control reporting.3,6 Manual monitoring is often incomplete, subjective, and resource-intensive, creating compliance gaps and potential institutional risk. The AI-based hand hygiene assessment system addresses these challenges by providing automated, encrypted logging of each handwashing event, including step completion, duration, and alerts issued. This enables data-driven quality improvement: for example, identifying that “finger interlacing rubbing” is frequently misperformed can prompt targeted training for staff (Figure 2).
The system incorporates all 10 standardized handwashing steps defined by WHO and CDC guidelines, with additional granularity on execution order and motion amplitude, ensuring full alignment with global standards and enhancing objective assessment. To ensure reproducibility across institutions with differing local protocols, the AI model was designed with a modular, configurable protocol engine that allows infection control teams to define institution-specific steps, duration thresholds, and antiseptic requirements without full model retraining. All visual recognition modules remain consistent regardless of local protocol variations, and only rule-based compliance logic is adjusted per site. This architecture ensures generalizability and reproducibility when deployed to hospitals with different local hand hygiene policies, while maintaining core recognition performance. By combining regulatory compliance with precise, step-specific monitoring, the system allows infection control teams to track trends, hospital administrators to generate transparent reports, and surgical staff to maintain high-quality hand hygiene. Overall, this approach strengthens institutional safety culture, supports guideline adherence, and provides actionable insights for continuous improvement in perioperative infection prevention.
Technical Advantages in Clinical Context
Existing hand hygiene tools, such as infrared sensors or basic motion detectors, only detect “washing vs not washing” and cannot assess step-specific compliance or duration, limiting their utility in operating rooms. 2 The proposed AI system combines multimodal data fusion (video, audio, sensors) with an enhanced CNN, achieving a 94.57% recognition rate, outperforming 3D-CNN models (∼85%) in dynamic OR conditions.13,14 Attention mechanisms and adaptive learning ensure robustness across routine and emergency surgeries, while sensor integration verifies antiseptic use, addressing regulatory requirements often missed by vision-only systems.4,5
This holistic monitoring—covering both procedural steps and material compliance—reduces the “false sense of compliance” seen with traditional tools and supports consistent hand hygiene. Improved compliance provides a mechanistic rationale for reducing SSI risk; however, long-term follow-up is needed to confirm clinical outcomes. Future randomized trials with 12-24 months’ follow-up should use SSI incidence as the primary endpoint to validate sustained benefits and patient safety impact.
Limitations and Future Directions
Despite its value, the system requires refinement to fully support surgical and infection control teams. Misclassification of similar steps (eg, “back of hands rubbing” vs “finger interlacing rubbing”), though rare (∼5%), may affect compliance assessment; future integration of transformer models with 3D-CNN architectures aims to improve recognition of subtle motions. 15 Although peak-time latency was minimal and rarely disruptive (average 180 ms, 99th percentile <500 ms), edge computing optimization will further reduce rare delays. Real-time user feedback channels were implemented to capture ongoing experience, and future iterations will integrate these inputs more closely into model adaptation. Occasional feedback latency during peak OR activity can disrupt workflow, addressable via optimized edge computing. Data privacy remains critical, with encrypted storage aligned to medical standards, while decentralized solutions may further enhance protection. Expanding to high-risk units and linking compliance to preventable infections rates via EHR integration could broaden the impact and provide definitive clinical evidence.
Conclusion
The AI-based hand hygiene assessment system enables real-time detection and standardized evaluation of hand hygiene practices in the operating room, improves procedural compliance and monitoring efficiency, and supports consistent adherence to recommended handwashing protocols. The user-centered design and automated feedback help maintain workflow stability and provide objective data for infection control quality improvement. The system demonstrates favorable clinical applicability and potential for perioperative safety enhancement. Preliminary cost estimates suggest a modest upfront investment: approximately US$1200-1800 per handwashing station for hardware (HD camera, display, sensors, and wiring) plus annual software licensing and maintenance fees of around US$300-500 per station. These costs are scalable across stations and institutions, supporting reasonable economic feasibility for most clinical settings. Broader adoption will require further multicenter validation, longer-term clinical follow-up, workflow integration, privacy and cybersecurity compliance, and cost-effectiveness assessment. With appropriate implementation, this system may serve as a useful tool to support standardized hand hygiene and strengthen patient safety efforts in operating rooms.
Supplemental Material
Supplemental Material - Evaluation of an Artificial Intelligence-Based System for Standardized Hand Hygiene Monitoring Among Operating Room Personnel
Supplemental Material for Evaluation of an Artificial Intelligence-Based System for Standardized Hand Hygiene Monitoring Among Operating Room Personnel by Fei Wang, Dong-Mei Bian, and Qian Wang in The American Surgeon™
Footnotes
Ethical Considerations
This study was conducted with approval from the Ethics Committee of Xijing Hospital (Approval Number: XJS20242281-C-1, Approval Date: October 6th 2024). This study was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all participants.
Authors’ contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.