
Abstract
Introduction
The postoperative impact of recent COVID-19 infection on patients undergoing thyroidectomy remains unclear. This study evaluates the 90-day postoperative outcomes in patients with recent COVID-19 compared to those without.
Methods
A retrospective cohort study was conducted using a large multi-institutional database. Adult patients who underwent total thyroidectomy or thyroid lobectomy were divided into 2 cohorts: those with a documented COVID-19 infection within 7 weeks before surgery and those without. Propensity score matching (1:1) was performed to balance age, sex, race, comorbidities, vaccination status, indications for surgery, and surgical procedure performed. Postoperative complications within 90 days were assessed, including hypocalcemia, dysphonia, recurrent laryngeal nerve (RLN) injury, hematoma, surgical site infection (SSI), venous thromboembolism (VTE), pulmonary embolism (PE), pneumonia, acute myocardial infarction (MI), and cerebral infarction. Risk ratios (RRs) with corresponding 95% confidence intervals (CIs) were calculated.
Results
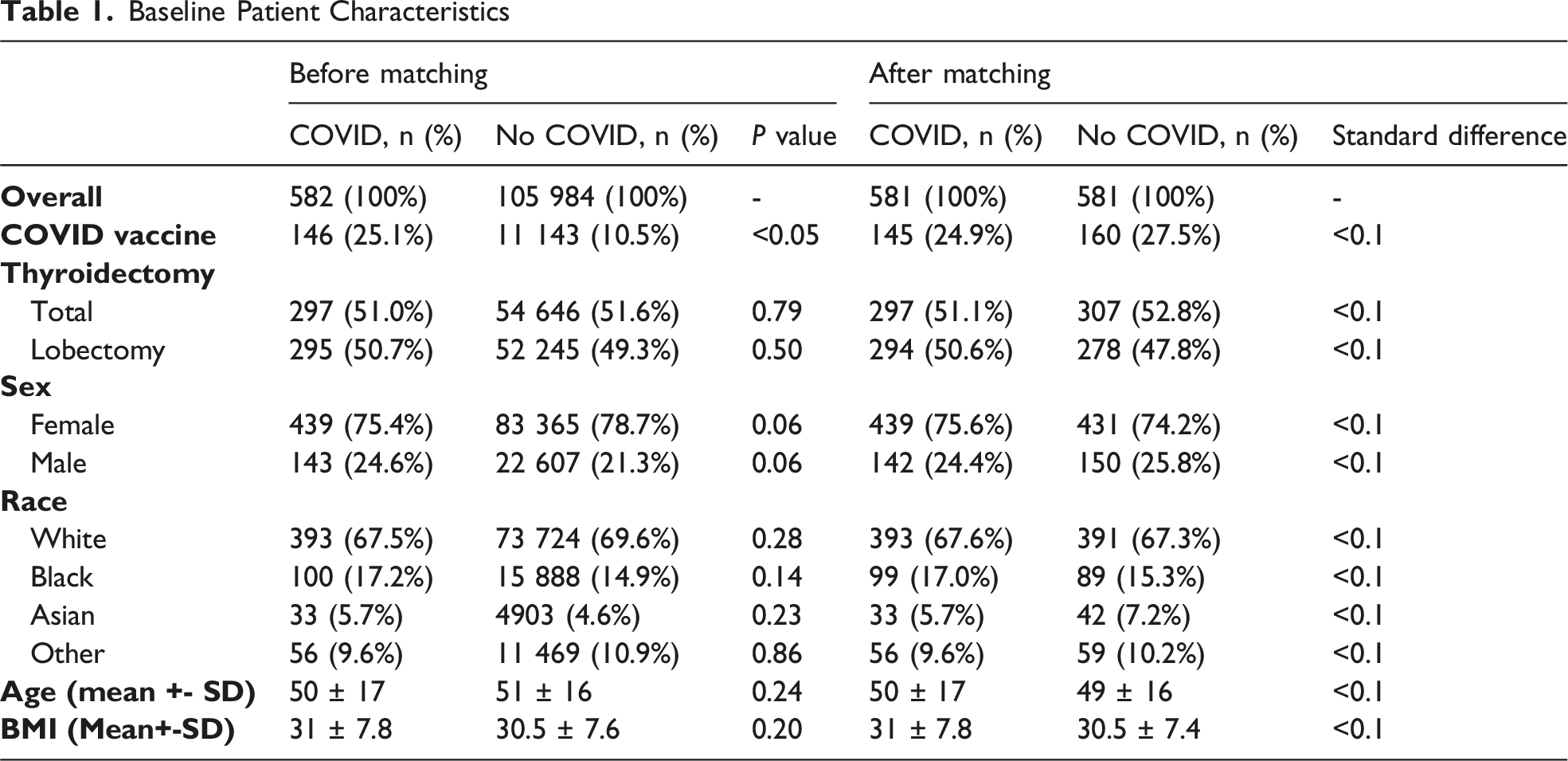
After matching, 581 patients were included in each cohort with similar age (50 vs 49 years) and sex distribution (75.6% vs 74.2% female). COVID-19 vaccination rates were comparable between groups (24.9% vs 27.5%). Thyroidectomy-specific complications were not significantly different. Hypocalcemia occurred in 10.2% of the COVID-19 cohort vs 7.2% (RR: 1.41, CI: 0.96–2.05), RLN injury in 3.3% vs 2.4% (RR: 1.36, CI: 0.69–2.68), and dysphonia in 7.4% vs 4.6% (RR: 1.59, CI: 0.99–2.54). COVID-19–related complications were rare. Pulmonary embolism occurred in 2.6% of COVID-19 patients, while all other events were reported as <10 in each group.
Conclusion
COVID-19 infection was not associated with an increased risk of major postoperative complications following thyroidectomy.
Key Takeaways
• Recent COVID-19 infection within 7 weeks of surgery was not associated with a statistically significant increase in thyroidectomy-specific complications, including hypocalcemia, recurrent laryngeal nerve injury, or dysphonia, compared to matched controls. • Systemic complications potentially related to COVID-19—including pulmonary embolism, venous thromboembolism, pneumonia, and myocardial infarction—were rare in both cohorts, suggesting that the cardiopulmonary risks of proceeding with thyroid surgery after COVID-19 recovery are low. • These findings support the safety of performing thyroidectomy in patients who have recently recovered from COVID-19, and call into question whether the previously recommended 7-week surgical delay remains necessary in the current post-pandemic era.
Introduction
Thyroid surgery is performed approximately 118 000 to 169 000 times per year in the United States. 1 Thyroidectomy is commonly performed for both malignant and benign thyroid conditions. Serious complications such as permanent recurrent laryngeal nerve injury or long-term hypoparathyroidism are relatively uncommon.2,3
The COVID-19 pandemic raised important questions about the timing of elective surgery after an infection. Early in the pandemic, the American Society of Anesthesiologists (ASA) recommended delaying non-urgent surgery for up to 7 weeks after a COVID-19 diagnosis, based on data showing increased risks of postoperative pulmonary complications and mortality in recently infected patients. 4 However, much of the early evidence informing these recommendations was derived from higher-risk surgical populations, limiting its direct applicability to lower-risk procedures such as thyroidectomy. In 2020, the rate of thyroid surgeries dropped by 16-17% and Velez et al found that the pandemic had significantly impacted thyroidectomy-related outcomes, specifically mortality.5,6
Beyond surgical delays, the pandemic also influenced disease presentation. Feier et al found that there was a decline in thyroid surgeries in early pandemic phases, followed by a rebound accompanied by an increase in advanced-stage and malignant thyroid tumors. 7 This suggests that delays in diagnosis and treatment may have contributed to more advanced disease at presentation, highlighting the importance of timely surgical management.7,8
Thyroidectomy is considered a safe, mostly outpatient procedure, 9 but it carries unique risks like recurrent laryngeal nerve injury and hypocalcemia, and it typically requires general anesthesia, which could pose challenges in patients with recent respiratory illness.2,10 It remains unclear whether a recent COVID-19 infection predisposes thyroid surgery patients to higher rates of these complications or other adverse events, such as thromboembolic or pulmonary issues.
Research has demonstrated that widespread vaccination campaigns have led to decreased COVID-19 mortality.11,12,13 With improved population immunity and increased time since the peak of the pandemic, an important question arises: Is the previously recommended delay period still necessary for thyroid surgery? Furthermore, it remains unclear whether perioperative risk following COVID-19 infection should be considered uniformly across all procedures or tailored based on procedure-specific risk. To address this gap, we conducted a retrospective cohort study to evaluate 90-day postoperative outcomes in patients with a recent COVID-19 infection compared with those without a COVID-19 diagnosis before thyroidectomy.
Methods
We conducted a retrospective cohort study using the TriNetX Research Network, a multi-institutional database of deidentified electronic health records (EHR). All analyses were performed using TriNetX analytic functions on deidentified data; therefore, this study was exempt from institutional review board approval. Additional details about the TriNetX platform are available at: https://trinetx.com/about-trinetx/.
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies, and a completed STROBE checklist is provided as Supplemental Material. 14
Patient groups, outcomes, and propensity score matching (PSM) variables were identified using International Classification of Diseases, 10th Edition (ICD-10) diagnosis codes, Current Procedural Terminology (CPT) codes, Logical Observation Identifiers Names and Codes (LOINC), and Clinical Vaccines Administered (CVX) codes (Supplementary File: Table 1). In TriNetX, patient counts of 1-9 are automatically suppressed and displayed as “<10,” and detailed results are not shown to protect patient privacy.
Adult patients who underwent either total thyroidectomy (TT) or thyroid lobectomy (TL) were identified and separated into 2 groups based on the presence of COVID-19 infection. The COVID-19 cohort was defined as those with at least one specific diagnostic code within 7 weeks before surgery (Supplementary File: Table 1). Patients undergoing TT or TL with no recorded diagnosis of COVID-19 during the 7-week preoperative interval served as controls.
Propensity score matching (PSM) was performed in a 1:1 ratio using a greedy nearest-neighbor algorithm. Variables included in the matching process were age, sex, race, ethnicity, body mass index (BMI), nicotine use, alcohol use disorder, diabetes, hypertension, congestive heart failure, cardiac arrhythmias, chronic pulmonary disease, renal failure, coagulopathy, vaccination status, type of surgery (TT vs TL), and indication for surgery (thyroid nodule, non-toxic multinodular goiter (MNG), toxic MNG, or thyroid cancer). All corresponding codes are provided in Supplementary File: Table 1.
Postoperative complications occurring within 90 days after surgery were evaluated. Thyroidectomy-specific outcomes included hypocalcemia, recurrent laryngeal nerve (RLN) injury, dysphonia, surgical site infection (SSI), and hematoma. Outcomes related to COVID-19 included pulmonary embolism (PE), venous thromboembolism (VTE), pneumonia, acute myocardial infarction (MI), and cerebral infarction.
Continuous variables were compared using a two-sided independent Student t-test, with P < 0.05 considered statistically significant. To assess PSM, standardized differences were used, and values <0.1 indicated successful PSM. For postoperative outcomes, risk ratios (RRs) and 95% confidence intervals (CIs) were calculated.
Results
A total of 106 566 adult patients undergoing thyroidectomy were identified: 582 (0.5%) in the COVID-19 cohort and 105 984 (99.5%) in the control cohort. Before matching, there were significant differences in vaccination rates; 25.1% of the COVID-19 cohort had documented vaccination, compared with 10.5% in the control group (P < 0.05).
Baseline Patient Characteristics
Post-operative Outcomes
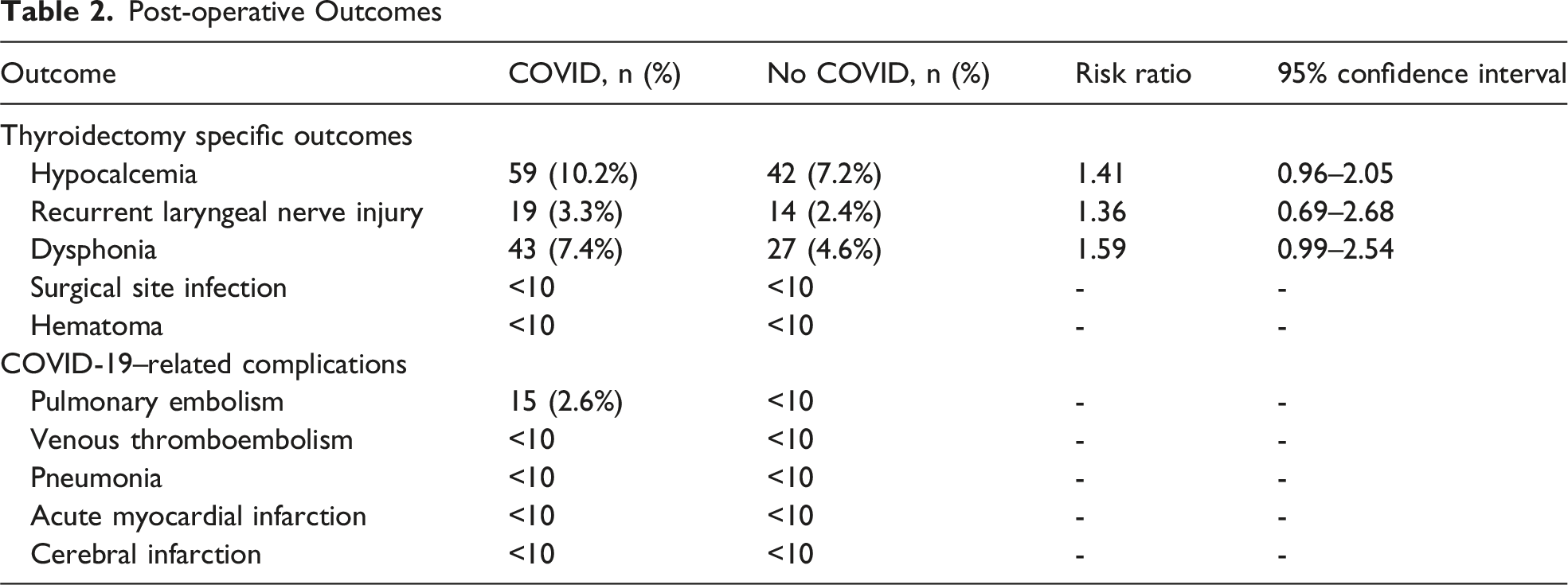
The incidence of COVID-19-related adverse events was low. PE occurred in 15 patients (2.6%) in the COVID-19 cohort, compared to <10 in the control cohort. Incidences of VTE, pneumonia, acute MI, and cerebral infarction were fewer than 10 patients in either group.
Discussion
This multi-institutional analysis demonstrates that a recent COVID-19 diagnosis is not associated with an increased risk of post-thyroidectomy complications. We observed no significant difference in the incidence of thyroid-specific adverse events—such as hypocalcemia, RLN injury, or hematoma—nor in systemic cardiopulmonary complications when compared to the control group.
Importantly, beyond confirming the safety of thyroidectomy after recent COVID-19 infection, our findings provide insight into how perioperative risk may vary based on procedure type and support a more nuanced, procedure-specific approach to surgical timing. These results provide reassurance that proceeding with necessary thyroid surgery in patients recovering from mild to moderate COVID-19 may be safer than initially feared.
Early in the pandemic, there was concern that undergoing surgery soon after a COVID-19 infection could lead to more frequent pulmonary complications or even increased mortality.4,15 The COVIDSurg Collaborative study in 2021 reported a higher postoperative mortality rate in patients who had recent COVID-19 infection, particularly if surgery took place within 6-7 weeks of infection. This led to recommendations to delay elective surgeries by at least 7 weeks when feasible.4,16 However, as the pandemic evolved, subsequent research showed different results. A recent study with approximately 30 000 surgical patients found no significant association between recent COVID-19 infection and adverse surgical outcomes. 17 Our study’s findings are consistent with their results, as we did not observe an increase in 90-day surgical complications. Similarly, Fei et al found no increase in postoperative complications among patients who underwent thyroid surgery within 2-4 weeks of COVID-19 infection, further supporting the safety of early operative intervention in well-selected patients. 18
Thyroidectomy is generally a low-risk procedure, with major complications—such as permanent RLN injury, chronic hypocalcemia, and cardiopulmonary morbidity—occurring infrequently, especially in high-volume, specialized centers.2,19,20,21 Consistent with prior national database studies demonstrating very low rates of pneumonia (0.2-0.3%), PE (0.05-0.1%), and VTE (0.1-0.2%) following thyroid surgery, our study also found low rates of thyroidectomy-specific and systemic complications in both the COVID-19 and control cohorts.22,23 This low baseline risk profile may explain why recent COVID-19 infection did not translate into a measurable increase in postoperative complications in this population.
There was a small numerical increase in PE in the COVID-19 group (2.6%) compared with the control cohort (<10 patients, ∼1.7%). Patients in the COVID-19 cohort had a slightly higher incidence of postoperative PE (2.6%) compared with the control group (<10 patients, approximately 1.7%). Although relative risk could not be calculated due to TriNetX suppression rules, this small numerical difference is biologically plausible given the pro-thrombotic and hyper coagulable state associated with recent COVID-19 infection. 24 However, the overall rarity of thromboembolic and cardiopulmonary events reinforces that thyroidectomy remains safe, even among patients with recent COVID-19, when patients are appropriately selected and optimized preoperatively.
From a clinical perspective, these findings have direct implications for preoperative decision-making, particularly when recent COVID-19 infection is identified shortly before scheduled surgery. Rigid delay paradigms derived from higher-risk surgical populations may not be necessary for low-risk procedures such as thyroidectomy, and surgical timing should instead incorporate both patient-level and procedure-specific risk.
This study has several limitations due to its retrospective design and reliance on EHR data. COVID-19 status was determined by ICD-10 coding, which may have led to misclassification, especially early in the pandemic when testing was limited. We could not assess the severity or timing of infection relative to surgery. We performed PSM to limit confounding factors, but we could not directly match or adjust for COVID-19 severity or for any delays in surgery determined by clinical judgment. Finally, our follow-up was limited to complications recorded within the health systems contributing to TriNetX. If patients sought care for complications outside those networks, some events might not be captured, although this should affect both groups similarly.
Conclusion
In summary, our multi-institutional study demonstrates that recent COVID-19 infection was not associated with increased risk of postoperative complications following thyroidectomy. Our findings suggest that thyroidectomy can be performed safely in patients who have recovered from COVID-19.
Supplemental Material
Supplemental material - Postoperative Outcomes of Thyroid Surgery Following Recent COVID-19 Infection
Supplemental material for Postoperative Outcomes of Thyroid Surgery Following Recent COVID-19 Infection by Hameeda Arif Arain, MBBS, Rachael Caretti, DO, Daniel Gomez Carrillo, MD, Azeem Izhar, MBBS, Andrea Gillis, MD, MSPH, Sophie Dream, MD, MPH, Brenessa Lindeman, MD, MEHP, and Herbert Chen, MD, in The American Surgeon™
Footnotes
Ethical Considerations
All research activities related to this article adhere to the legal and ethical requirements of the United States of America and the Institutional Review Board.
Author Contributions
Hameeda Arif Arain, MBBS: Writing original draft, Formal analysis, Data curation, Conceptualization.
Rachael Caretti, DO: Writing review and editing.
Daniel Gomez Carrillo MD: Writing review and editing.
Azeem Izhar MBBS: Writing review and editing.
Andrea Gillis MD, MSPH: Writing review and editing, Supervision.
Sophie Dream MD, MPH: Writing review and editing, Supervision.
Brenessa Lindeman MD, MEHP: Writing review and editing, Supervision.
Herbert Chen, MD: Writing review and editing, Conceptualization, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Rachael Caretti, DO, is supported by the National Institutes of Health (NIH) under a Ruth L. Kirschstein National Research Service Award (NRSA) Institutional Research Training Grant (T32), grant number T32CA229102, through University of Alabama Medical Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study were obtained from the TriNetX Research Network, a global federated health research platform that provides access to de-identified electronic medical records from participating healthcare organizations. Due to data use agreements and patient privacy regulations, the data cannot be shared publicly.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.